
Tooth Surface Loss An Overview
Tooth Surface Loss An Overview
You might also like
- Endodontic McqsDocument151 pagesEndodontic McqsHanan Moh91% (22)
- MCQs in DentistryDocument135 pagesMCQs in Dentistrysam4sl98% (85)
- Evidence Plan: Competency Standard: Carpentry Nc2 Unit of Competency: Ways in Which Evidence Will Be CollectedDocument5 pagesEvidence Plan: Competency Standard: Carpentry Nc2 Unit of Competency: Ways in Which Evidence Will Be CollectedBhem Boy100% (1)
- 5 Non Carious Changes To Tooth CrownDocument14 pages5 Non Carious Changes To Tooth CrownjiwanjyotkaurNo ratings yet
- Leader, Commission - 1998 - Dental ErosionDocument11 pagesLeader, Commission - 1998 - Dental Erosionjanvier_89No ratings yet
- Beckett 1994Document8 pagesBeckett 1994Devin Chun Yue KwanNo ratings yet
- Topics of Interest Analyzing The Etiology of An Extremely Worn DentitionDocument10 pagesTopics of Interest Analyzing The Etiology of An Extremely Worn DentitionLuigi BortolottiNo ratings yet
- Johannson - Erosion - 2012 PDFDocument18 pagesJohannson - Erosion - 2012 PDFRusevNo ratings yet
- BSRD Tooth Wear BookletDocument28 pagesBSRD Tooth Wear BookletSalma RafiqNo ratings yet
- 36-1 TunkiwalaDocument16 pages36-1 TunkiwalaSwapnil RastogiNo ratings yet
- A New Look at Erosive Tooth Wear in Elderly People: JADA 2007 138 (9 Supplement) :21S-25SDocument5 pagesA New Look at Erosive Tooth Wear in Elderly People: JADA 2007 138 (9 Supplement) :21S-25SMarek1964No ratings yet
- Tooth Wear and AgingDocument5 pagesTooth Wear and AgingSARA TREJO GONZALEZNo ratings yet
- A Proposed System For Screening Tooth WearDocument3 pagesA Proposed System For Screening Tooth Wear4j6kzvfjytNo ratings yet
- Non Carious Tooth Surface Loss - 48Document4 pagesNon Carious Tooth Surface Loss - 48na huNo ratings yet
- Use of Tooth Colored Restorations in The Management of ToothwearDocument6 pagesUse of Tooth Colored Restorations in The Management of ToothwearCiára MaharajNo ratings yet
- UntitledDocument321 pagesUntitledAnalisse PerezNo ratings yet
- Nature Chapter 2017Document17 pagesNature Chapter 2017Milena AndrićNo ratings yet
- Tooth Wear, Etiology, Diagnosis and Its Management in Elderly: A Literature ReviewDocument0 pagesTooth Wear, Etiology, Diagnosis and Its Management in Elderly: A Literature ReviewmegamarwaNo ratings yet
- Dentine Hypersensitivity - Guidelines For The Management of A Common Oral Health ProblemDocument25 pagesDentine Hypersensitivity - Guidelines For The Management of A Common Oral Health ProblemNaoki MezarinaNo ratings yet
- ADJ2009 - Abfraction Separating Fact From CtionDocument7 pagesADJ2009 - Abfraction Separating Fact From CtionEdward LiuNo ratings yet
- Tooth Wear An Authoritative Reference For Dental Professionals and Students (Andrew Eder, Maurice Faigenblum, (Eds.) ) (Z-Library)Document313 pagesTooth Wear An Authoritative Reference For Dental Professionals and Students (Andrew Eder, Maurice Faigenblum, (Eds.) ) (Z-Library)Diego DuranNo ratings yet
- Sidang Tesis TGL 30 Oktober 2014 Final FixedDocument11 pagesSidang Tesis TGL 30 Oktober 2014 Final Fixedfaizal prabowo KalimanNo ratings yet
- Dental Erosion in Children: A Literature ReviewDocument7 pagesDental Erosion in Children: A Literature ReviewHala LalaNo ratings yet
- Art 6Document8 pagesArt 6Florin Eugen ConstantinescuNo ratings yet
- Tooth Surface Loss Revisited: Classification, Etiology, and ManagementDocument9 pagesTooth Surface Loss Revisited: Classification, Etiology, and Managementkhalida iftikharNo ratings yet
- CASE REPORT Unusual Dental Erosion Caused by A Cola DrinkDocument5 pagesCASE REPORT Unusual Dental Erosion Caused by A Cola DrinkAlina BortaNo ratings yet
- Guia Anterior - Gonzalez Hernandez-61-2Document12 pagesGuia Anterior - Gonzalez Hernandez-61-2Fred TorresNo ratings yet
- Compozitia Smaltului Si DemineralizareaDocument10 pagesCompozitia Smaltului Si DemineralizareaMadalina Elena TapeleaNo ratings yet
- Digital Workflow For The Rehabilitation of The Excessively Worn DentitionDocument26 pagesDigital Workflow For The Rehabilitation of The Excessively Worn Dentitionfloressam2000No ratings yet
- The Dahl Concept Past Present and FutureDocument9 pagesThe Dahl Concept Past Present and FuturevivigaitanNo ratings yet
- Joor 12972Document10 pagesJoor 12972HristoNo ratings yet
- TALLER 1 Erosión Lussi2011Document11 pagesTALLER 1 Erosión Lussi2011Natalia SplashNo ratings yet
- SJ BDJ 2011 1099 PDFDocument11 pagesSJ BDJ 2011 1099 PDFalfredoibcNo ratings yet
- Grande Área: Ciências Da Saúde e Ciências BiológicasDocument4 pagesGrande Área: Ciências Da Saúde e Ciências BiológicasJean PachecoNo ratings yet
- 4752 Wzaripah2Document7 pages4752 Wzaripah2inibuatdaftar101No ratings yet
- Erosion DecisionmakingDocument8 pagesErosion DecisionmakinganushiNo ratings yet
- Non Cervical Lesions Meena MamDocument120 pagesNon Cervical Lesions Meena Mamanshida v pNo ratings yet
- Indice KnightDocument7 pagesIndice Knightandrea caballeroNo ratings yet
- Worn DentitionDocument8 pagesWorn DentitionHassan MoussaouiNo ratings yet
- Delayed Tooth Eruption Pa Tho Genesis, Diagnosis and Treatment.Document14 pagesDelayed Tooth Eruption Pa Tho Genesis, Diagnosis and Treatment.DrFarhana AfzalNo ratings yet
- Tooth Surface Loss RevisitedDocument7 pagesTooth Surface Loss Revisiteddorasani99No ratings yet
- Possible Role of Tensile Stress in The Etiology of Cervical Erosive Lesions of TeethDocument7 pagesPossible Role of Tensile Stress in The Etiology of Cervical Erosive Lesions of TeethRaul Alfonsin SanchezNo ratings yet
- s41415 023 5624 0 LibreDocument6 pagess41415 023 5624 0 LibreAZWATEE BINTI ABDUL AZIZNo ratings yet
- Rehabilitacion de La Denticion Desgastada - Johansson Et Al - JOR 2008Document19 pagesRehabilitacion de La Denticion Desgastada - Johansson Et Al - JOR 2008Pablo BenitezNo ratings yet
- The Cracked Tooth Conundrum: Terminology, Classification, Diagnosis, and ManagementDocument9 pagesThe Cracked Tooth Conundrum: Terminology, Classification, Diagnosis, and ManagementMohd NazrinNo ratings yet
- CrownandExtracoronalRestorations EndodWhitworthDocument11 pagesCrownandExtracoronalRestorations EndodWhitworthMitza CristianNo ratings yet
- Wear of Teeth and RestorationsDocument7 pagesWear of Teeth and RestorationsAya Ibrahim YassinNo ratings yet
- Tooth Wear 1Document11 pagesTooth Wear 1Kcl Knit A SocNo ratings yet
- A Guide To The Clinical Management of Attrition: PracticeDocument5 pagesA Guide To The Clinical Management of Attrition: PracticemmputraNo ratings yet
- Dental Wear - A Scanning Electron Microscope Study - 2014Document8 pagesDental Wear - A Scanning Electron Microscope Study - 2014Ana CondeNo ratings yet
- Abrasi DLLDocument9 pagesAbrasi DLLDiana Gita MentariNo ratings yet
- Restorative Management of The Worn Dentition Pt1Document6 pagesRestorative Management of The Worn Dentition Pt1Sherif ReffatNo ratings yet
- Reviewing The Concept of Dahl: S S A J. SDocument5 pagesReviewing The Concept of Dahl: S S A J. Spablogdv956No ratings yet
- Australian Dental Journal - 2013 - Meyers - Minimum Intervention Dentistry and The Management of Tooth Wear in GeneralDocument6 pagesAustralian Dental Journal - 2013 - Meyers - Minimum Intervention Dentistry and The Management of Tooth Wear in GeneralEdmund KwongNo ratings yet
- 7.caries and Other Reasons For Restoring TeethDocument16 pages7.caries and Other Reasons For Restoring TeethramenatttNo ratings yet
- Non Carious Tooth Surface LossDocument4 pagesNon Carious Tooth Surface LossmirfanulhaqNo ratings yet
- Dental Attrition - Aetiology, Diagnosis and Treatment Planning: A ReviewDocument7 pagesDental Attrition - Aetiology, Diagnosis and Treatment Planning: A ReviewInternational Organization of Scientific Research (IOSR)No ratings yet
- Dental Erosion. Definition, Classification and LinksDocument5 pagesDental Erosion. Definition, Classification and LinksRusevNo ratings yet
- Pulp IrritantsDocument8 pagesPulp IrritantsKarma YogaNo ratings yet
- Lussi - Dec 2006Document7 pagesLussi - Dec 2006Anda MihaelaNo ratings yet
- Effect of Occlusal Vertical Dimension of CompleteDocument7 pagesEffect of Occlusal Vertical Dimension of CompletedrlenaaaNo ratings yet
- Worksheet My HobbiesDocument2 pagesWorksheet My HobbiesdrlenaaaNo ratings yet
- كراسة الخط لغة عربيةDocument29 pagesكراسة الخط لغة عربيةdrlenaaaNo ratings yet
- Transfusion of Blood & Blood ProductsDocument18 pagesTransfusion of Blood & Blood ProductsdrlenaaaNo ratings yet
- Pinelands National ReserveDocument2 pagesPinelands National ReservesallyNo ratings yet
- 1 PBDocument9 pages1 PBFriga FmNo ratings yet
- Intelligent Gesture Controlled Wireless Wheelchair For The Physically HandicappedDocument6 pagesIntelligent Gesture Controlled Wireless Wheelchair For The Physically HandicappedshivaramreddyNo ratings yet
- Audio Channel Layout Mapping Between Audio Formats PDFDocument5 pagesAudio Channel Layout Mapping Between Audio Formats PDFalvcardxNo ratings yet
- United States Patent: Serban Et AlDocument9 pagesUnited States Patent: Serban Et AlMutia Herlisa14No ratings yet
- L4Tnm-Psa: Product ClassificationDocument4 pagesL4Tnm-Psa: Product Classificationhassan329No ratings yet
- Assessment 1 IMINT Exercise BRAVODocument6 pagesAssessment 1 IMINT Exercise BRAVOYousef Al HashemiNo ratings yet
- Starter Case 580M 1Document4 pagesStarter Case 580M 1JESUSNo ratings yet
- Political Culture in Post Communist Countries Albanian CaseDocument10 pagesPolitical Culture in Post Communist Countries Albanian CaseArditÇekaNo ratings yet
- Summer Farm: By: Norman Maccaig Group: Camila Luna and Estrella LinDocument8 pagesSummer Farm: By: Norman Maccaig Group: Camila Luna and Estrella LinJamieDuncanNo ratings yet
- BEE301Document4 pagesBEE301cshohil300No ratings yet
- PGM List R1 - 05.04.2018Document58 pagesPGM List R1 - 05.04.2018Shubham Shinde100% (1)
- Chemistry Test 11 Chap 1-5Document2 pagesChemistry Test 11 Chap 1-5Sabitra RudraNo ratings yet
- Sodium Sulfite: Product Safety SummaryDocument5 pagesSodium Sulfite: Product Safety SummaryMannar1No ratings yet
- Mels Subtype DescriptionsDocument11 pagesMels Subtype DescriptionsclaraNo ratings yet
- Rizals First Published Essay El Amor PatDocument23 pagesRizals First Published Essay El Amor PatNelly MesiasNo ratings yet
- GCT LTE Module Software Development Guide: Aquila Solutions IncDocument26 pagesGCT LTE Module Software Development Guide: Aquila Solutions IncLionel MusonzaNo ratings yet
- State Centric Theories of International Relations Belong To The Past in Security StudiesDocument3 pagesState Centric Theories of International Relations Belong To The Past in Security StudiesshoufiiNo ratings yet
- Desjoyaux PoolsDocument25 pagesDesjoyaux Poolslina casadiegoNo ratings yet
- Tyler Street News November 2010Document4 pagesTyler Street News November 2010tsumcNo ratings yet
- Exercise Sheet: A. Grammar Exercise 1: Fill in Where, Whose, Who, Which, When and WhyDocument6 pagesExercise Sheet: A. Grammar Exercise 1: Fill in Where, Whose, Who, Which, When and WhyArthasNo ratings yet
- E1695-01 CT System Performance MeasurementDocument4 pagesE1695-01 CT System Performance MeasurementsanthakumarNo ratings yet
- Bharat Heavy Electricals LimitedDocument4 pagesBharat Heavy Electricals LimitedkmbkrisNo ratings yet
- Instructions For Use: 1. To Ensure An Effective Molecular WeldDocument2 pagesInstructions For Use: 1. To Ensure An Effective Molecular WeldQuy RomNo ratings yet
- G. Vrbová (Auth.), Professor Dr. W. A. Nix, Professor Dr. G. Vrbová (Eds.) - Electrical Stimulation and Neuromuscular Disorders-Springer-Verlag Berlin Heidelberg (1986)Document148 pagesG. Vrbová (Auth.), Professor Dr. W. A. Nix, Professor Dr. G. Vrbová (Eds.) - Electrical Stimulation and Neuromuscular Disorders-Springer-Verlag Berlin Heidelberg (1986)Harshavardhan SNo ratings yet
- 12 Architecture & Methodology ENDocument36 pages12 Architecture & Methodology ENYash BhatnagarNo ratings yet
- 2.15 Punching Shear Strength of RC Slabs Using Lightweight ConcreteDocument8 pages2.15 Punching Shear Strength of RC Slabs Using Lightweight Concretejack21abNo ratings yet
- A Handbook of Art SmithingDocument232 pagesA Handbook of Art SmithingArtisan Ideas100% (3)
- Energy Recovery From Landing AircraftDocument8 pagesEnergy Recovery From Landing AircraftRaniero FalzonNo ratings yet






























































































See discussions, stats, and author profiles for this publication at: https://www.researchgate.
net/publication/13210542
Tooth surface loss: An overview
Article in British dental journal official journal of the British Dental Association: BDJ online · February 1999
DOI: 10.1038/sj.bdj.4800020a2 · Source: PubMed
CITATIONS READS
117 3,631
2 authors, including:
Martin Kelleher
King's College London
92 PUBLICATIONS 1,762 CITATIONS
SEE PROFILE
All content following this page was uploaded by Martin Kelleher on 09 September 2016.
The user has requested enhancement of the downloaded file.
PRACTICE
tooth surface loss
1 Tooth surface loss:
an overview
M. Kelleher,1 and K. Bishop,2
The management of tooth surface loss (TSL) aetiological factors which are associated with
demands a full understanding of its aetiology the loss of tooth tissue. Eccles suggested that Pathological,
and presentation. This paper provides the intro- the term ‘tooth surface loss’ should be used non-carious loss of
duction to the series and an overview of patho- when a single aetiological factor was often dif- tooth tissue is an
logical, non-carious loss of tooth tissue. ficult to identify.7 Smith and Knight, however, increasing problem to
Emphasis is placed on the aetiological factors considered that ‘TSL’ belittled the severity of
the dental profession,
which are currently thought to be major causes the problem and, therefore, advocated the use
of this problem. This directs the paper toward of the term ‘tooth-wear’ to embrace all three with young
those agents that produce erosive tooth surface aetiological conditions.2 Broad terms to individuals especially
loss. This is appropriate given the increasing describe the processes involved are helpful at risk. This paper
incidence and severity of this type of tooth wear. since a single aetiology is less common.8,9 For provides an overview
The article attempts only relatively brief clarity, ‘TSL’ will be used throughout this
descriptions of the presentation and aetiology paper to describe the pathological, non-cari- of the problem with an
of attritional and abrasive tooth surface loss. ous loss of tooth tissue although ‘tooth-wear’ emphasis on the
This does not imply that they are less important and ‘TSL’ are often interchangeable. The possible causes,
but rather reflects the increased concern over terms, ‘erosion’, ‘abrasion’ and ‘attrition’ are particularly those
the need for prevention, early detection and still useful where there is a clear indication of a
factors which may
control of acid erosion. Later articles in the specific aetiology or where aetiological factors
series will return to the presentation and man- are being discussed. account for the
agement of the other types of TSL. The preven- increased incidence.
tive management of bruxism is described in the Erosion The clinical
third and sixth paper. It would appear that erosion is a major cause of appearance produced
Non carious loss of tooth tissue is a normal TSL. Smith and Knight, for example, could
physiological process and occurs throughout exclude it as a cause of TSL in only 11% of by the various
life.1 If the rate of loss is likely to prejudice the patients examined.10 Traditionally, factors aetiological factors is
survival of the teeth, or is a source of concern to which may cause erosion have been described discussed and
the patient, then it may be considered ‘patholog- as originating from the following sources:11 recommendations
ical’.2 The dental management of patients with • Dietary
made on the
such loss of tooth tissue has provided difficulties • Regurgitation
for the dental profession for many years and it is • Environmental. objectives of the
generally agreed that the problem is increasing. immediate and
Table 1 Definitions of attrition, erosion, and
This can only partly be explained by the fact that abrasion long-term
the population is retaining more natural teeth management of
into old age.2,3 It is not only the middle-aged and Attrition The loss by wear of tooth substance or a
restoration caused by mastication or the problem.
elderly who exhibit pathological loss of tooth tis- contact between occluding or
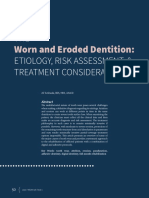
sue, but also younger age groups (fig. 1).4 Robb approximal surfaces
reported that the prevalence of pathological loss
Erosion The progressive loss of hard dental
of tooth tissue in patients less than 26 years of age tissues by chemical process not
was greater than in many older age groups.5 The involving bacterial action
Child Dental Health Survey (1994)6 confirmed
Abrasion The loss by wear of tooth substance or The Series Editors are Richard Ibbetson
this when 32% of 14-year-olds had evidence of a restoration caused by factors other and Andrew Eder of the Eastman Dental
erosion affecting the palatal surfaces of their per- than tooth contact Institute for Oral Healthcare Sciences
manent incisors. This cannot be explained as an and the Eastman Dental Hospital
age-related phenomenon. It may, however, be Table 2 pH of commonly consumed drinks
the result of changing lifestyles and social pres-
Manufacturer Brand pH
sures which have led to the increased promi-
nence of particular aetiological factors. 1Consultant in Restorative Dentistry,
Pepsi-Cola Diet 2.95
Coca Cola Regular 3.15 King’s Dental Institute, London;
Aetiology Caffeine free – diet 3.30
2Consultant in Restorative Dentistry,
Traditionally, the terms ‘erosion’, ‘abrasion’ Tab clear – diet 3.20 Maxillofacial Unit, Morriston
and ‘attrition’ have been used to describe the Lucozade Sport Orange 3.78 Hospital, Swansea SA6 6NL
REFEREED PAPER
non-carious, pathological loss of tooth tissue Tango Diet Orange 2.80
Orange Juice 3.50 © British Dental Journal
(Table 1). These terms reflect the specific 1999; 186: 61–66
BRITISH DENTAL JOURNAL, VOLUME 186, NO. 2, JANUARY 23 1999 61
PRACTICE
tooth surface loss
sales in the UK, since 1970 and a 7-fold
increase since 1950 (Fig. 2).9 Adolescents and
children account for 65% of sales with 42% of
fruit drinks consumed by children between
the ages of 2 and 9 years old.9,14 This con-
sumption of soft drinks by this age group has
been identified as the probable cause for the
erosion recorded in the Child Dental Health
Survey (1994).6
Slimness and ‘healthy eating’ are now per-
ceived to be important in western society. This
has helped the newer ‘diet’ drinks to achieve a
greater share of the sales market (fig. 3). These
low calorie drinks are also acidic (Table 2) with,
Fig. 1 Palatal view of maxillary teeth of a 16-year-old female who except for the sugar, similar constituents to the
had drunk a litre of ‘diet’ carbonated drinks a day for the past two traditional beverages. The potential for erosive
years. There is marked tooth surface loss affecting the anterior damage by these ‘diet’ beverages may be less
teeth, particularly the central incisors where the pulps are visible
well appreciated. The acidic nature of soft
drinks, therefore, makes them a significant aeti-
ological factor in TSL, particularly in younger
patients. Eccles confirmed the importance of
8000
Millions of
these beverages when he reported that they
litres were implicated as aetiological factors in 40%
6000 of patients with TSL.15
A ‘healthy’ diet may also contain substantial
4000 acidic foods16–18 and cause further loss of
tooth tissue. Furthermore, the abrasive nature
of many of the components of these diets may
2000
accelerate TSL. (Certain dietary components,
such as curries, also have the potential to
0 cause TSL indirectly, by causing gastric
1950 1960 1970 1980 1990
reflux.19)
Year
Regurgitation erosion
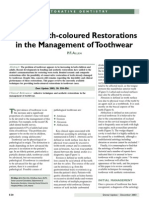
Fig. 2 Total soft drink sales in the UK 1950–1990
(Source: British Soft Drinks Association, 1994) Regurgitation results in gastric acid entering
the mouth. The regurgitation may be involun-
tary or self-induced as in bulimia nervosa.5,20
Involuntary regurgitation: Involuntary regur-
50 gitation is a common complication of gastro-
Percentage intestinal problems such as hiatus hernia (fig.
40 4). The effect of the regurgitated acid on the
teeth is well documented.21,22 Furthermore,
30
medication used to treat such problems may
20 also be a cause of TSL.22
Gastritis and acid regurgitation are com-
10 mon complications of chronic alcoholism,
although patients may not be aware of the
0 problem.23,24 Often the patient is secretive
1989 1990 1990 1990 1990 Projected
about the habit and confirmation is usually
2000
Year difficult. There is also a group of patients, for
example the young adult, who have frequent
Fig. 3 Market share of ‘diet’ carbonated drinks in the UK alcoholic ‘binges’. Such binges are often associ-
(Source: British Soft Drinks Association, 1994) ated with episodes of vomiting. These patients
tend to be less secretive about their alcohol
consumption. Soft drinks which are fre-
Dietary erosion quently used as ‘mixers’ with alcoholic drinks
Dietary erosion may result from food or may also contribute to TSL.
drinks containing a variety of acids, especially One of the major roles of saliva is to dilute
citric acid which may chelate as well as dis- and buffer any acid which enters the mouth and
solve calcium ions.12 Citric and phosphoric lubricate the occluding surfaces during masti-
acid are common constituents of soft drinks cation. If salivary flow is reduced, the potential
and fruit juices (Table 2).13 These beverages for erosive and attritional damage increases.25
are now widely available, with a doubling of As medical science advances and life
62 BRITISH DENTAL JOURNAL, VOLUME 186, NO. 2, JANUARY 23 1999
PRACTICE
tooth surface loss
expectancy increases, the use of drugs within
the population is more widespread.26 Many of
these drugs cause a dry mouth and, as such, the
associated problems are likely to become more
prevalent.27 The problem may be compounded
if patients consume acidic drinks in an attempt
to alleviate the symptoms and stimulate sali-
vary flow.
Voluntary regurgitation:Voluntary regurgita-
tion may be practised by patients with an eating
disorder. Such disorders are a feature of a body-
conscious society and often begin in early
adolescence, frequently running a chronic
course with substantial complications.28 The
prevalence of eating disorders in the general Fig. 4 Palatal view of maxillary teeth of a 35-year-old male with a
population would appear to be increasing with history of hiatus hernia. There is general ‘erosive’ tooth surface
figures reported for anorexia nervosa of loss, with the teeth having a rounded appearance with ‘cupping’
between 0.1–0.2% and 1–2% for bulimia on the palatal cusps of the premolars. The damage is limited to the
palatal aspects of the teeth
nervosa. However, eating disorder patients may
actively avoid detection or be reluctant to
disclose details of their problem and as such the
true prevalence may be underestimated.28,29
The effect of acid regurgitation in eating
disorder patients has been well docu-
mented.30–34 The most common sign is peri-
molysis — erosive lesions localised to the
palatal aspects of the maxillary teeth (fig. 5).
These lesions are thought to be the result of the
tongue directing gastric contents forward dur-
ing voluntary and prepared vomiting with the
lateral spread of the tongue protecting the lower
teeth.16,32
The pattern of TSL in eating disorder patients
may also be affected by other aetiological fac-
tors such as:16
• Erosive ‘diet’ beverages and ‘healthy’ foods as
patients strive to control their weight
• Xerostomia, caused by vomit-induced dehy- Fig. 5 Mirror view of the palatal aspects of the
maxillary teeth of a 22-year-old female
dration or drugs such as diuretics, appetite bulimic. Note the extensive ‘erosive’ tooth
suppressants and anti-depressants surface loss with the teeth having a rounded
• Long-term complications such as gastric appearance and the surface characteristics lost.
ulcers and hiatus hernia.28 The 1| and 4| have been root-filled following
pulpal necrosis
Environmental erosion
Environmental erosion occurs when patients
are exposed to acids in their work-place or dur-
ing leisure activities.35,36 Health and safety laws
have probably reduced the risk of environmen-
tal erosion although it should not be ignored as
a possible aetiological factor.
Environmental erosion predominantly affects
the labial surfaces of the maxillary and
mandibular incisors.
Attrition
Attritional TSL primarily affects the occlusal
and incisal surfaces of teeth although slight
loss may occur at the approximal contact
areas (fig. 6). This type of TSL can be particu-
larly significant in patients with a vegetarian Fig. 6 Labial view of mandibular anterior teeth in a 40-year-old
or a modern ‘healthy’ diet.37 Attritional TSL male bruxist. The teeth have flattened incisal edges as the enamel
and dentine wear at the same rate. The teeth ‘match’ the palatal
may also be a consequence of parafunctional surfaces of the maxillary teeth in excursive movements
activity.38,39
BRITISH DENTAL JOURNAL, VOLUME 186, NO. 2, JANUARY 23 1999 63
PRACTICE
tooth surface loss
Body image
In the 1980s, fashion designers and image mak-
ers have promoted the concept that ‘slimness’
equates with ‘attractive’ or ‘successful’. This
concept is supported by role models who may
have significantly influenced young people’s
perception of the ‘ideal’ body shape. In an
attempt to control body weight patients may
consume acidic foods such as fruit and diet
drinks rather than high calorie alternatives.
This struggle to achieve the ‘ideal’ body shape
may also partly account for the increased preva-
lence of eating disorders.
Soft drink manufacturers
Fig. 7 Labial view of |3 showing ‘V’-shaped labial cervical lesion The soft drink industry is a multi-million
pound business. Coca-Cola, for example, is the
biggest brand label in the world with an esti-
Abrasion mated brand value of nearly $9,000 million.
Abrasion is caused by abnormal rubbing of Marketing of soft drinks, traditionally, has been
tooth tissue or restoration by a non-dental directed to the young adult by associating the
object eg pipe-smoking, hair-grips etc.11 How- beverages with peer group acceptability. More
ever, the most common cause is probably incor- recently, the drinks have been promoted as
rect or over vigorous toothbrushing37; although ‘healthy’ and linked to high profile sportsmen
Smith and Knight10 found that the occurrence and women. Consumption of acidic beverages
of abrasion was infrequent compared with other following exercise may be more dangerous
types of TSL (fig. 7). Furthermore, the location because of dehydration and a subsequent reduc-
of some ‘abrasive’ lesions cannot be explained tion in the buffering capacity of the saliva.
by toothbrushing alone and other TSL factors
such as erosion may contribute to the prob- Refrigeration
lem.9,37 Recently, interest has grown in the role Refrigeration has aided widespread accessibil-
1 Flint S, Scully C. Orofacial age
changes and related disease. Dent of occlusal stresses in the development of cervi- ity to fruits, fruit-juices and soft drinks. It has
Update 1988; 15: 337-342. cal ‘abrasive’ lesions and the term abfraction has allowed many fruits and vegetables to be avail-
2 Smith B G N, Knight J K. An index been used to describe these. able continually rather than when ‘in season’.
for measuring the wear of teeth. Br
Consequently, diets can contain highly acidic
Dent J 1984; 156: 435-438.
3 Watson I B, Tulloch E N. Clinical Prevalence foods and drinks all year round whereas previ-
assessment of cases of tooth surface It is generally accepted that the prevalence of ously many elements were restricted to particu-
loss. Br Dent J 1985; 159: 144-148. TSL increases with age.5,40–42 However, the lar times of the year.
4 Bishop K A, Briggs P F A, Kelleher M
G D. The aetiology and management
exact prevalence is unclear, primarily because
of localized anterior tooth wear in the of differing assessment criteria.42 Hugoson et Healthcare workers
young adult. Dent Update 1994; 21: al.,39 for example, reported that 13–24% of sur- Healthcare workers, such as doctors and dieti-
153-161. faces showed evidence of occlusal wear. Other cians, advocate that fresh fruit should be a com-
5 Robb, N. Epidemiological study of
tooth wear. London: University of studies have observed that between 25% and ponent of a ‘balanced’ diet. These foods are,
London, 1991. PhD Thesis. 50% of subjects had evidence of TSL.9 Some therefore, promoted as a ‘healthy’ option to
6 O’Brien M. Childrens dental health in loss of tooth tissue is normal during a patients’ ‘harmful’ alternatives. Patients are unlikely to
the United Kingdom. London:
HMSO, 1994.
lifetime as a result of ‘wear and tear’. The loss is be warned of the damage associated with acidic
7 Eccles J D. Tooth surface loss from likely to be a problem only when the degree foods. Dentists may indirectly support this
abrasion, attrition and erosion. Dent exceeds what would be considered ‘normal’ for concept by advising their patients to avoid
Update 1982; 35: 373-381. a particular age. Studies which consider only sugar. Patients may perceive that foods and
8 Smith B G N. Some facets of
toothwear. Ann R Aust Coll Dent Surg ‘pathological’ TSL may, therefore, be more rele- drinks that do not contain sugar must there-
1991; 11: 37-51. vant to clinical dentistry. The tooth wear index fore, be less damaging to their teeth. Dentists
9 Shaw L, Smith A. Erosion in children: (TWI)2 attempted to achieve this by proposing often suggest that patients should brush their
An increasing clinical problem? Dent
maximum acceptable tooth tissue loss for each teeth after exposure to foods and drinks con-
Update 1994; 21: 103-106.
10 Smith B G N, Knight J K. A decade of life. Tooth surface loss in excess of taining sugar or acid, but such practices may
comparison of patterns of tooth wear these figures was considered ‘pathological’. accelerate TSL.43
with aetiological factors. Br Dent J Using this index, between 4.5 and 5.7% of sur-
1984; 157: 16-19.
11 Mair L H. Wear in dentistry —
faces examined exhibited TSL.2,5 Restorative materials
current terminology. J Dent 1992; 20: Although the actual prevalence of TSL is Dentists often use ‘aesthetic’ restorations,
140-144. unclear, there is general agreement that the pop- irrespective of whether the restoration is visi-
12 Jarvinen V K, Rytomaa I I, Heinonen, ulation, particularly the young, is experiencing ble. Many of these materials have the poten-
O P. Risk factors in dental erosion. J
Dent Res 1991; 70: 942-947. increased exposure to elements which cause tial to accelerate TSL, particularly if used on
13 Kelleher M, Bishop K. Personal TSL.4,5 The exact reason for this is unclear but occluding surfaces in parafunctional patients
communication, 1994. the following factors may be implicated: (fig. 8).44,45
64 BRITISH DENTAL JOURNAL, VOLUME 186, NO. 2, JANUARY 23 1999
PRACTICE
tooth surface loss
14 Rugg-Gunn A J, Hackett A F,
Appleton D R, Jenkins G N, Eastoe J
E. Relationship between dietary
habits and caries increment assessed
over two years in 405 English
adolescent school children. Arch Oral
Biol 1984; 29: 983-987.
15 Eccles J D. Erosion affecting the
palatal surfaces of upper anterior
teeth in young people. Br Dent J
1982; 152: 375-378.
16 Hellstrom, I. Oral complications in
anorexia nervosa. Scand J Dent Res
1977; 85: 71-86.
17 Giunta J L. Dental erosion resulting
from chewable vitamin C tablets. J
Am Dent Assoc 1983; 107: 253-256.
18 Linkosalo E, Markkanen H. Dental
erosions in relation to lactovegetarian
Fig. 8 Labial view of anterior teeth of a 60-year-old male with diet. Scand J Dent Res 1985; 93: 436-
marked tooth surface loss affecting 12|caused by the abrasive 441.
porcelain palatal surface of 1| 19 Bartlett D W, Evans D F, Smith, B G
N. Simultaneous oral and
oesophageal pH measurement after a
Clinical appearance of TSL has been a deterioration in the appearance of reflux provoking meal. J Dent Res
1994; Spec Issue Abst 70.
Although a ‘classical’ clinical appearance has the teeth. The earliest changes are because of 20 Jarvinen V, Meurman J H, Hyvarinen
been described for erosion, attrition and abra- the loss of enamel. This may cause an increase H et al. Dental erosion and upper
sion it is unlikely that the appearances described in tooth translucency, both interproximally and gastrointestinal disorders. Oral Surg
Oral Med Oral Pathol 1988; 65:
are a result of a single factor.46 If dietary acid is at the incisal edges.46 Continued TSL may pro- 298-303.
applied to a tooth surface then the surface duce fractures of the enamel and shortening of 21 Howden G F. Erosion as the
becomes frosty and white. However, the clinical the teeth.47 The loss of enamel may also presenting symptom in hiatus hernia.
‘erosive’ lesion is smooth and polished.37 There- increase the visibility of the underlying dentine, Br Dent J 1971; 131: 455-456
22 Rytomaa I, Jarvinen V, Heinonen, O
fore attrition and/or abrasion is probably also producing a more yellow tooth colour.4 P. Etiological factors in dental
present additionally. Even so, certain clinical fea- erosion. J Dent Res 1990; 69: Spec.
tures can indicate a dominant aetiological factor. Conservation of tooth structure Issue. Abst 587.
23 Simmons M S, Thompson D C.
Teeth affected by erosion become rounded The loss of tooth tissue is often substantial and Dental erosion secondary to ethanol-
and lose their surface characteristics (figs. 4 and the need to conserve remaining tooth structure is induced emesis. Oral Surg Oral Med
5). Attrition, however, is associated with flat- vital. This is particularly important in the young, Oral Path 1987; 64: 731-713.
tening of the cusp tips or incisal edges and where tooth tissue is at a premium because of the 24 Smith B G N, Robb N D. Dental
erosion in patients with chronic
localised facets on the occlusal or palatal sur- lack of secondary dentine. For this reason, ‘adhe- alcoholism. J Dent 1987; 17:
faces (fig. 6). Following dentine exposure, the sive’ restorations should be considered before 219-221.
clinical appearance is determined by the rela- ‘conventional’ methods since the latter require 25 Bloem T J, McDowell G C, Lang B R
tive contributions of the aetiological factors. If further loss of tooth tissue. et al. In vitro wear. Part II wear and
abrasion of composite restorative
the TSL is primarily attritional then the dentine materials. J Prosthet Dent 1988; 60:
will wear at the same rate as the surrounding Sensitivity and pain 242-249.
enamel. In this situation the shape of the facet Exposure of dentinal tubules and their subse- 26 Seymour R A. Dental pharmacology
problems in the elderly. Dent Update
will be determined by the movement of the quent bacterial colonisation can lead to both 1988; 15: 375-380.
opposing tooth. Traditionally it is suggested pulpal inflammation and sensitivity.48 In 27 Levine R.S. Saliva: 3. Xerostomia -
that when an erosive factor is present, ‘cupping’ younger patients with rapid erosion, this is fur- aetiology and management. Dent
or ‘grooves’ form in the dentine and the base of ther exacerbated by the lack of secondary den- Update 1989; 16: 197-201.
28 Treasure J. Long-term management
the defect is not in contact with the opposing tine and large pulps. In extreme cases, pulpal of eating disorders. Int Rev Psych
tooth (fig. 4).11 However, this may be an over- exposure can occur, further complicating man- 1991; 3: 43-58.
simplification of the changes that take place. agement (fig. 5). 29 Kidd E A M, Smith B G N. Toothwear
histories: a sensitive issue. Dent
Cervical lesions caused by an abrasive tend to Update 1989; 20: 174-178.
be angular and ‘V’-shaped while erosion results Inter-occlusal space 30 Allen D N. Dental Erosion from
in shallow, rounded lesions (fig. 7). Berry and Poole,49 suggested that occlusal TSL Vomiting. Br Dent J 1969; 126:
The clinical appearance of restorations may is compensated by alveolar growth which 311-312.
31 Andrew F F H. Dental erosion due to
also indicate a possible major aetiological fac- maintains the occlusal vertical dimension anorexia nervosa with bulimia. Br
tor. Amalgam and composite restorations, for (OVD). However, if the rate of loss is greater Dent J 1982; 152: 89-90.
example, tend to be unaffected by erosive fac- than the compensatory mechanism then the 32 Stege P, Visco-Dangler L, Rye L.
tors and remain ‘proud’ of the surrounding OVD is reduced. The effect of TSL on the Anorexia nervosa: review including
oral & dental manifestations. J Am
tooth tissue. However, both restorations show occlusal vertical dimension is neither pre- Dent Assoc 1982; 104: 648-652.
evidence of faceting if attrition is the major dictable nor uniform. 33 Abrams R A, Ruff L C. Oral signs and
aetiological factor.11 symptoms in the diagnosis of
bulimia. J Am Dent Assoc 1986; 113:
Patient compliance and expectations 761-764.
Clinical problems Self-awareness and peer or social pressures may 34 Gilmour A G, Beckett H A. The
Aesthetics lead patients to refuse to comply with advice voluntary reflux phenomenon. Br
Often a patient is only aware of TSL when there concerning the management of TSL. These Dent J 1993; 175: 368-371.
BRITISH DENTAL JOURNAL, VOLUME 186, NO. 2, JANUARY 23 1999 65
PRACTICE
tooth surface loss
35 Petersen P E, Gormsen C. Oral concerns may result in the rejection of a pro- tion of the patient’s response to initial care.
conditions among German battery
factory workers. Community Dent
posed restorative treatment plan: metal palatal The reassessment should include whether the
Oral Epidemiol 1991; 19: 104-106. restorations, for example, may be unacceptable original aetiological factors are still present
36 Centerwall B S, Armstrong C W, because of ‘grey-out’.4 It is important that the although this can be difficult to determine.
Funkerhouser L S, Elzay R. Erosion of implications of non-compliance and treatment Treatment needs can also be evaluated during
dental enamel among competitive
swimmers at a gas-chlorinated alternatives are fully discussed with the patient. this time and the patient’s views and expecta-
swimming pool. Am J Epidemiol tions considered.
1986; 123: 641-647. Management
37 Smith B G N. Toothwear: aetiology
Long-term management
and diagnosis. Dent Update 1989; 16:
204-212. Immediate therapy The treatment planning options available
38 Krogh-Poulson W, Carlsen O R. The aim of the immediate phase of therapy is are:
Bidfunktion/Bettfysiologi. Denmark: to:
Munksgaard, Kobenhavn. 1979, p269.
39 Dahl B L, Krogstad O, Karlsen K. An
• Relieve sensitivity and pain Review and monitoring
alternative treatment in cases with • Identify aetiological factors Providing the patient has no functional,
advanced localized attrition. J Oral • Protect remaining tooth tissue. occlusal, aesthetic or sensitivity problems fol-
Rehabil 1975; 2: 209-214. All aetiological factors for the TSL should lowing stabilisation then close monitoring of
40 Hugoson A, Bergendal T, Ekfeldt A,
Helkimo M. Prevalence and severity be identified and eliminated although full the situation is acceptable. This should involve
of incisal and occlusal tooth wear in compliance may be difficult. At the very least the construction of accurate study casts: a set
an adult Swedish population. Acta a ‘damage limitation’ policy should be initi- of casts should be given to the patient so that if
Odontol Scand 1988; 46: 255-265. ated. This should involve identification, con- there is a change in dentist, the records are
41 Ekfeldt A, Hugoson A, Bergendal T,
Helkimo M. An individual tooth wear trol and advice relating to the causative available. Colour transparencies or pho-
index and an analysis of factors factors. Consideration should be given to the tographs are also useful. A regular recall regime
correlated to incisal and occlusal wear following: should be initiated and the patient instructed
in an adult Swedish population. Acta
Odontol Scand 1990; 48: 343-349.
• Diet analysis and counselling to control or to return if they suspect any deterioration. If
42 Donachie M A. The dental health of reduce the effect of aetiological factors.50 the rate of TSL is likely to jeopardise the tooth’s
the ageing population of Newcastle • Advice to consume erosive beverages through long-term viability, then monitoring of the sit-
upon Tyne. Newcastle: University of a wide-bore straw and to swallow immedi- uation alone is unwise and restoration
Newcastle, 1992. MDS thesis .
43 Davis W B, Winter P J. The effect of ately and not ‘swish’ the drink around the becomes necessary.
abrasion on enamel and dentine after mouth. Although teeth should not be
exposure to dietary acid. Br Dent J brushed immediately following exposure to Restorative treatment
1980; 148: 253-256. erosive factors, the exact ‘safe’ time period Restorative treatment is indicated when sta-
44 Jacobi R, Shillingburg H H T,
Duncanson M G. A comparison of when oral hygiene can be carried out is bilisation techniques have failed to resolve the
the abrasiveness of six ceramic unknown. This may reduce the risk of abra- patient’s dental problems. It is a widely-held
surfaces and gold. J Prosthet Dent sive TSL.9,43 view that restorative treatment in the pres-
1991; 66: 303-309.
45 Ratledge D K, Smith B G N, Wilson,
• Prescription of a neutral, sodium fluoride ence of ongoing TSL is unwise. Nevertheless,
R F. The effect of restorative materials mouthrinse or gel for daily use to combat there are occasions when control proves
on the wear of human enamel. J acid damage and control pulpal sensitivity.51 impossible and, to preserve the teeth, restora-
Prosthet Dent 1994; 72: 194-203. Acidulated phosphate fluoride should be tion becomes essential. The patients should
46 Eccles J D, Jenkins W G. Dental
erosion and diet. J Dent 1974; 2:
avoided because of its obvious acidity. be aware of both the advantages and disad-
153-159. • Construction of a close fitting occlusal guard vantages of any proposed treatment. Restora-
47 Eccles J D. Dental erosion of non in those suspected of parafunctioning or tion should be based on the following
industrial origin. A clinical survey where the aetiology is uncertain.52 A guard principles:
and classification. J Pros Dent 1979;
42: 649-653. may also be useful in bulimics to protect the • Protection and conservation of remaining
48 Brannstrom M. The cause of teeth during periods of vomiting. Alkali, such tooth structure
postrestorative sensitivity and its as milk of magnesia, can be applied to the fit- • Resolution of pulpal sensitivity
prevention. J Endodont 1986; 10:
475-481.
ting surface of the guard to neutralise any • Improvement in aesthetics if necessary.
49 Berry D C, Poole D F G. Attrition: acid pooling or alternatively a neutral fluo-
possible mechanisms of compensa- ride gel placed in the appliance.53 Appliances Conclusion
tion. J Oral Rehabil 1976; 3: 201-206. covering teeth must be used with extreme The paper has placed considerable emphasis on
50 Kidd A M, Joyston-Bechal S.
Essentials of dental caries: the disease
caution if there is a chance of acid being the aetiology of tooth surface loss as without an
and its management. Chapts 6 and 7. trapped beneath them. understanding of this, prevention and control
Bristol: Wright, 1987. • Direct application of glass ionomer and/or are impossible. One of the major concerns in
51 Bartlett D W, Smith B G N, Wilson, composite to sensitive areas. the United Kingdom is the increased incidence
R F. Comparison of the effect of
fluoride and non-fluoride toothpaste • Consultation with the general medical prac- of TSL caused by acid erosion. Many of the rea-
on tooth wear in vitro and the titioner regarding involuntary acidic reflux sons for this are dietary but others relate to
influence of enamel fluoride and/or psychiatrists to evaluate the patient’s regurgitation of acid. The next article in this
concentration and hardness of
psychological status and background, espe- series will discuss eating disorders in detail and
enamel. Br Dent J 1994; 176: 346-348.
52 Gierdrys-Leeper E. Night guards and cially in cases of bulimia nervosa. the management of patients who are affected by
occlusal splints. Dent Update 1990; this seemingly increasingly common condition.
17: 325-329. Reassessment
53 Kleier D J, Aragon S B, Averbach, R E.
Dental management of the chronic
Following immediate therapy, a period of This article is based on a presentation at The Medical Society of
vomiting patient. J Am Dent Assoc time should elapse before a long-term treat- London on 5 October 1994 as part of the Alpha Omega lecture
1984; 108: 618-621. ment plan is considered allowing an evalua- programme.
66 BRITISH DENTAL JOURNAL, VOLUME 186, NO. 2, JANUARY 23 1999
View publication stats
You might also like
- Endodontic McqsDocument151 pagesEndodontic McqsHanan Moh91% (22)
- MCQs in DentistryDocument135 pagesMCQs in Dentistrysam4sl98% (85)
- Evidence Plan: Competency Standard: Carpentry Nc2 Unit of Competency: Ways in Which Evidence Will Be CollectedDocument5 pagesEvidence Plan: Competency Standard: Carpentry Nc2 Unit of Competency: Ways in Which Evidence Will Be CollectedBhem Boy100% (1)
- 5 Non Carious Changes To Tooth CrownDocument14 pages5 Non Carious Changes To Tooth CrownjiwanjyotkaurNo ratings yet
- Leader, Commission - 1998 - Dental ErosionDocument11 pagesLeader, Commission - 1998 - Dental Erosionjanvier_89No ratings yet
- Beckett 1994Document8 pagesBeckett 1994Devin Chun Yue KwanNo ratings yet
- Topics of Interest Analyzing The Etiology of An Extremely Worn DentitionDocument10 pagesTopics of Interest Analyzing The Etiology of An Extremely Worn DentitionLuigi BortolottiNo ratings yet
- Johannson - Erosion - 2012 PDFDocument18 pagesJohannson - Erosion - 2012 PDFRusevNo ratings yet
- BSRD Tooth Wear BookletDocument28 pagesBSRD Tooth Wear BookletSalma RafiqNo ratings yet
- 36-1 TunkiwalaDocument16 pages36-1 TunkiwalaSwapnil RastogiNo ratings yet
- A New Look at Erosive Tooth Wear in Elderly People: JADA 2007 138 (9 Supplement) :21S-25SDocument5 pagesA New Look at Erosive Tooth Wear in Elderly People: JADA 2007 138 (9 Supplement) :21S-25SMarek1964No ratings yet
- Tooth Wear and AgingDocument5 pagesTooth Wear and AgingSARA TREJO GONZALEZNo ratings yet
- A Proposed System For Screening Tooth WearDocument3 pagesA Proposed System For Screening Tooth Wear4j6kzvfjytNo ratings yet
- Non Carious Tooth Surface Loss - 48Document4 pagesNon Carious Tooth Surface Loss - 48na huNo ratings yet
- Use of Tooth Colored Restorations in The Management of ToothwearDocument6 pagesUse of Tooth Colored Restorations in The Management of ToothwearCiára MaharajNo ratings yet
- UntitledDocument321 pagesUntitledAnalisse PerezNo ratings yet
- Nature Chapter 2017Document17 pagesNature Chapter 2017Milena AndrićNo ratings yet
- Tooth Wear, Etiology, Diagnosis and Its Management in Elderly: A Literature ReviewDocument0 pagesTooth Wear, Etiology, Diagnosis and Its Management in Elderly: A Literature ReviewmegamarwaNo ratings yet
- Dentine Hypersensitivity - Guidelines For The Management of A Common Oral Health ProblemDocument25 pagesDentine Hypersensitivity - Guidelines For The Management of A Common Oral Health ProblemNaoki MezarinaNo ratings yet
- ADJ2009 - Abfraction Separating Fact From CtionDocument7 pagesADJ2009 - Abfraction Separating Fact From CtionEdward LiuNo ratings yet
- Tooth Wear An Authoritative Reference For Dental Professionals and Students (Andrew Eder, Maurice Faigenblum, (Eds.) ) (Z-Library)Document313 pagesTooth Wear An Authoritative Reference For Dental Professionals and Students (Andrew Eder, Maurice Faigenblum, (Eds.) ) (Z-Library)Diego DuranNo ratings yet
- Sidang Tesis TGL 30 Oktober 2014 Final FixedDocument11 pagesSidang Tesis TGL 30 Oktober 2014 Final Fixedfaizal prabowo KalimanNo ratings yet
- Dental Erosion in Children: A Literature ReviewDocument7 pagesDental Erosion in Children: A Literature ReviewHala LalaNo ratings yet
- Art 6Document8 pagesArt 6Florin Eugen ConstantinescuNo ratings yet
- Tooth Surface Loss Revisited: Classification, Etiology, and ManagementDocument9 pagesTooth Surface Loss Revisited: Classification, Etiology, and Managementkhalida iftikharNo ratings yet
- CASE REPORT Unusual Dental Erosion Caused by A Cola DrinkDocument5 pagesCASE REPORT Unusual Dental Erosion Caused by A Cola DrinkAlina BortaNo ratings yet
- Guia Anterior - Gonzalez Hernandez-61-2Document12 pagesGuia Anterior - Gonzalez Hernandez-61-2Fred TorresNo ratings yet
- Compozitia Smaltului Si DemineralizareaDocument10 pagesCompozitia Smaltului Si DemineralizareaMadalina Elena TapeleaNo ratings yet
- Digital Workflow For The Rehabilitation of The Excessively Worn DentitionDocument26 pagesDigital Workflow For The Rehabilitation of The Excessively Worn Dentitionfloressam2000No ratings yet
- The Dahl Concept Past Present and FutureDocument9 pagesThe Dahl Concept Past Present and FuturevivigaitanNo ratings yet
- Joor 12972Document10 pagesJoor 12972HristoNo ratings yet
- TALLER 1 Erosión Lussi2011Document11 pagesTALLER 1 Erosión Lussi2011Natalia SplashNo ratings yet
- SJ BDJ 2011 1099 PDFDocument11 pagesSJ BDJ 2011 1099 PDFalfredoibcNo ratings yet
- Grande Área: Ciências Da Saúde e Ciências BiológicasDocument4 pagesGrande Área: Ciências Da Saúde e Ciências BiológicasJean PachecoNo ratings yet
- 4752 Wzaripah2Document7 pages4752 Wzaripah2inibuatdaftar101No ratings yet
- Erosion DecisionmakingDocument8 pagesErosion DecisionmakinganushiNo ratings yet
- Non Cervical Lesions Meena MamDocument120 pagesNon Cervical Lesions Meena Mamanshida v pNo ratings yet
- Indice KnightDocument7 pagesIndice Knightandrea caballeroNo ratings yet
- Worn DentitionDocument8 pagesWorn DentitionHassan MoussaouiNo ratings yet
- Delayed Tooth Eruption Pa Tho Genesis, Diagnosis and Treatment.Document14 pagesDelayed Tooth Eruption Pa Tho Genesis, Diagnosis and Treatment.DrFarhana AfzalNo ratings yet
- Tooth Surface Loss RevisitedDocument7 pagesTooth Surface Loss Revisiteddorasani99No ratings yet
- Possible Role of Tensile Stress in The Etiology of Cervical Erosive Lesions of TeethDocument7 pagesPossible Role of Tensile Stress in The Etiology of Cervical Erosive Lesions of TeethRaul Alfonsin SanchezNo ratings yet
- s41415 023 5624 0 LibreDocument6 pagess41415 023 5624 0 LibreAZWATEE BINTI ABDUL AZIZNo ratings yet
- Rehabilitacion de La Denticion Desgastada - Johansson Et Al - JOR 2008Document19 pagesRehabilitacion de La Denticion Desgastada - Johansson Et Al - JOR 2008Pablo BenitezNo ratings yet
- The Cracked Tooth Conundrum: Terminology, Classification, Diagnosis, and ManagementDocument9 pagesThe Cracked Tooth Conundrum: Terminology, Classification, Diagnosis, and ManagementMohd NazrinNo ratings yet
- CrownandExtracoronalRestorations EndodWhitworthDocument11 pagesCrownandExtracoronalRestorations EndodWhitworthMitza CristianNo ratings yet
- Wear of Teeth and RestorationsDocument7 pagesWear of Teeth and RestorationsAya Ibrahim YassinNo ratings yet
- Tooth Wear 1Document11 pagesTooth Wear 1Kcl Knit A SocNo ratings yet
- A Guide To The Clinical Management of Attrition: PracticeDocument5 pagesA Guide To The Clinical Management of Attrition: PracticemmputraNo ratings yet
- Dental Wear - A Scanning Electron Microscope Study - 2014Document8 pagesDental Wear - A Scanning Electron Microscope Study - 2014Ana CondeNo ratings yet
- Abrasi DLLDocument9 pagesAbrasi DLLDiana Gita MentariNo ratings yet
- Restorative Management of The Worn Dentition Pt1Document6 pagesRestorative Management of The Worn Dentition Pt1Sherif ReffatNo ratings yet
- Reviewing The Concept of Dahl: S S A J. SDocument5 pagesReviewing The Concept of Dahl: S S A J. Spablogdv956No ratings yet
- Australian Dental Journal - 2013 - Meyers - Minimum Intervention Dentistry and The Management of Tooth Wear in GeneralDocument6 pagesAustralian Dental Journal - 2013 - Meyers - Minimum Intervention Dentistry and The Management of Tooth Wear in GeneralEdmund KwongNo ratings yet
- 7.caries and Other Reasons For Restoring TeethDocument16 pages7.caries and Other Reasons For Restoring TeethramenatttNo ratings yet
- Non Carious Tooth Surface LossDocument4 pagesNon Carious Tooth Surface LossmirfanulhaqNo ratings yet
- Dental Attrition - Aetiology, Diagnosis and Treatment Planning: A ReviewDocument7 pagesDental Attrition - Aetiology, Diagnosis and Treatment Planning: A ReviewInternational Organization of Scientific Research (IOSR)No ratings yet
- Dental Erosion. Definition, Classification and LinksDocument5 pagesDental Erosion. Definition, Classification and LinksRusevNo ratings yet
- Pulp IrritantsDocument8 pagesPulp IrritantsKarma YogaNo ratings yet
- Lussi - Dec 2006Document7 pagesLussi - Dec 2006Anda MihaelaNo ratings yet
- Effect of Occlusal Vertical Dimension of CompleteDocument7 pagesEffect of Occlusal Vertical Dimension of CompletedrlenaaaNo ratings yet
- Worksheet My HobbiesDocument2 pagesWorksheet My HobbiesdrlenaaaNo ratings yet
- كراسة الخط لغة عربيةDocument29 pagesكراسة الخط لغة عربيةdrlenaaaNo ratings yet
- Transfusion of Blood & Blood ProductsDocument18 pagesTransfusion of Blood & Blood ProductsdrlenaaaNo ratings yet
- Pinelands National ReserveDocument2 pagesPinelands National ReservesallyNo ratings yet
- 1 PBDocument9 pages1 PBFriga FmNo ratings yet
- Intelligent Gesture Controlled Wireless Wheelchair For The Physically HandicappedDocument6 pagesIntelligent Gesture Controlled Wireless Wheelchair For The Physically HandicappedshivaramreddyNo ratings yet
- Audio Channel Layout Mapping Between Audio Formats PDFDocument5 pagesAudio Channel Layout Mapping Between Audio Formats PDFalvcardxNo ratings yet
- United States Patent: Serban Et AlDocument9 pagesUnited States Patent: Serban Et AlMutia Herlisa14No ratings yet
- L4Tnm-Psa: Product ClassificationDocument4 pagesL4Tnm-Psa: Product Classificationhassan329No ratings yet
- Assessment 1 IMINT Exercise BRAVODocument6 pagesAssessment 1 IMINT Exercise BRAVOYousef Al HashemiNo ratings yet
- Starter Case 580M 1Document4 pagesStarter Case 580M 1JESUSNo ratings yet
- Political Culture in Post Communist Countries Albanian CaseDocument10 pagesPolitical Culture in Post Communist Countries Albanian CaseArditÇekaNo ratings yet
- Summer Farm: By: Norman Maccaig Group: Camila Luna and Estrella LinDocument8 pagesSummer Farm: By: Norman Maccaig Group: Camila Luna and Estrella LinJamieDuncanNo ratings yet
- BEE301Document4 pagesBEE301cshohil300No ratings yet
- PGM List R1 - 05.04.2018Document58 pagesPGM List R1 - 05.04.2018Shubham Shinde100% (1)
- Chemistry Test 11 Chap 1-5Document2 pagesChemistry Test 11 Chap 1-5Sabitra RudraNo ratings yet
- Sodium Sulfite: Product Safety SummaryDocument5 pagesSodium Sulfite: Product Safety SummaryMannar1No ratings yet
- Mels Subtype DescriptionsDocument11 pagesMels Subtype DescriptionsclaraNo ratings yet
- Rizals First Published Essay El Amor PatDocument23 pagesRizals First Published Essay El Amor PatNelly MesiasNo ratings yet
- GCT LTE Module Software Development Guide: Aquila Solutions IncDocument26 pagesGCT LTE Module Software Development Guide: Aquila Solutions IncLionel MusonzaNo ratings yet
- State Centric Theories of International Relations Belong To The Past in Security StudiesDocument3 pagesState Centric Theories of International Relations Belong To The Past in Security StudiesshoufiiNo ratings yet
- Desjoyaux PoolsDocument25 pagesDesjoyaux Poolslina casadiegoNo ratings yet
- Tyler Street News November 2010Document4 pagesTyler Street News November 2010tsumcNo ratings yet
- Exercise Sheet: A. Grammar Exercise 1: Fill in Where, Whose, Who, Which, When and WhyDocument6 pagesExercise Sheet: A. Grammar Exercise 1: Fill in Where, Whose, Who, Which, When and WhyArthasNo ratings yet
- E1695-01 CT System Performance MeasurementDocument4 pagesE1695-01 CT System Performance MeasurementsanthakumarNo ratings yet
- Bharat Heavy Electricals LimitedDocument4 pagesBharat Heavy Electricals LimitedkmbkrisNo ratings yet
- Instructions For Use: 1. To Ensure An Effective Molecular WeldDocument2 pagesInstructions For Use: 1. To Ensure An Effective Molecular WeldQuy RomNo ratings yet
- G. Vrbová (Auth.), Professor Dr. W. A. Nix, Professor Dr. G. Vrbová (Eds.) - Electrical Stimulation and Neuromuscular Disorders-Springer-Verlag Berlin Heidelberg (1986)Document148 pagesG. Vrbová (Auth.), Professor Dr. W. A. Nix, Professor Dr. G. Vrbová (Eds.) - Electrical Stimulation and Neuromuscular Disorders-Springer-Verlag Berlin Heidelberg (1986)Harshavardhan SNo ratings yet
- 12 Architecture & Methodology ENDocument36 pages12 Architecture & Methodology ENYash BhatnagarNo ratings yet
- 2.15 Punching Shear Strength of RC Slabs Using Lightweight ConcreteDocument8 pages2.15 Punching Shear Strength of RC Slabs Using Lightweight Concretejack21abNo ratings yet
- A Handbook of Art SmithingDocument232 pagesA Handbook of Art SmithingArtisan Ideas100% (3)
- Energy Recovery From Landing AircraftDocument8 pagesEnergy Recovery From Landing AircraftRaniero FalzonNo ratings yet