Download as docx, pdf, or txt
You might also like
- Epidural Technique in Obstetric Anesthesia-Springer International Publishing - Springer (2020) PDFDocument176 pagesEpidural Technique in Obstetric Anesthesia-Springer International Publishing - Springer (2020) PDFomarvillaNo ratings yet
- An Update On Menopause ManagementDocument10 pagesAn Update On Menopause ManagementJuan FranciscoNo ratings yet
- ATS Jurnal DR - HYS, - DR - OKA, - DR - EVP, - DR - RYN MyastheniaDocument6 pagesATS Jurnal DR - HYS, - DR - OKA, - DR - EVP, - DR - RYN MyastheniaAnton Supono Wong TekAnNo ratings yet
- Roth 2015Document5 pagesRoth 2015Raissa Metasari TantoNo ratings yet
- Article 10.1111/tog.12576Document8 pagesArticle 10.1111/tog.12576Keeranmayeeishra0% (1)
- Management of Mysthaenia Gravis During Pregnancy A Report of Eight Cases-1Document6 pagesManagement of Mysthaenia Gravis During Pregnancy A Report of Eight Cases-1rumaisyah alkatiriNo ratings yet
- 28 - NuevoDocument12 pages28 - NuevoJUAN GARCIANo ratings yet
- Case ReportDocument6 pagesCase ReportEka Budi UtamiNo ratings yet
- Endometriosis and Menopause-Management StrategiesDocument6 pagesEndometriosis and Menopause-Management Strategiesm.solorzanoNo ratings yet
- Child Myastenia GravisDocument7 pagesChild Myastenia GravisiuliaNo ratings yet
- Guillain-Barré Syndrome (GBS) and Myasthenia Gravis (MG)Document29 pagesGuillain-Barré Syndrome (GBS) and Myasthenia Gravis (MG)aya84048No ratings yet
- Esclerosis y Embarazo 5Document2 pagesEsclerosis y Embarazo 5povadicNo ratings yet
- Admin, 044 - 838 - Anthonyus S Bima Pakasi - GalleyDocument5 pagesAdmin, 044 - 838 - Anthonyus S Bima Pakasi - GalleyGusprian Paulus HasibuanNo ratings yet
- Dr. Rozhan Yassin Khalil: Presented byDocument37 pagesDr. Rozhan Yassin Khalil: Presented bySyasya NanaNo ratings yet
- Myasthenia GravisDocument5 pagesMyasthenia GravisBj DuquesaNo ratings yet
- Transverse Myelitis Preexisting in Pregnancy A Case ReportDocument6 pagesTransverse Myelitis Preexisting in Pregnancy A Case Reporttam meiNo ratings yet
- Neurological Deseases in PregnancyDocument6 pagesNeurological Deseases in PregnancyOdi KaiNo ratings yet
- Autoimmune Diseases in Pregnancy-5Document89 pagesAutoimmune Diseases in Pregnancy-5Vhutshilo MasithembiNo ratings yet
- Anaesthesia Management Patient With Eclamsia and Unconsciousness: A Case ReportDocument2 pagesAnaesthesia Management Patient With Eclamsia and Unconsciousness: A Case Reportadityo wibhisonoNo ratings yet
- Guidelines EuromyastheniaDocument4 pagesGuidelines Euromyastheniadokter mudaNo ratings yet
- Current Concepts in Migraine and Their Relevance To PregnancyDocument6 pagesCurrent Concepts in Migraine and Their Relevance To PregnancyWiwit Zuriati UnoNo ratings yet
- Autoimmune Myasthenia Gravis: Emerging Clinical and Biological HeterogeneityDocument16 pagesAutoimmune Myasthenia Gravis: Emerging Clinical and Biological HeterogeneityGiuseppeNo ratings yet
- Myasthenia Gravis ReportDocument4 pagesMyasthenia Gravis ReportNURSETOPNOTCHERNo ratings yet
- Kapoor 2018Document8 pagesKapoor 2018angela_karenina_1No ratings yet
- Myasthenia Gravis Foundation of AmericaDocument1 pageMyasthenia Gravis Foundation of AmericaFrancez Anne Guanzon100% (1)
- SRF - Ahmad Arya Sukma Bhakti - 03016006Document7 pagesSRF - Ahmad Arya Sukma Bhakti - 03016006LoserlikemeNo ratings yet
- Au Di Minor Case Study Myasthenia GravisDocument17 pagesAu Di Minor Case Study Myasthenia Gravisapi-301816885No ratings yet
- Successful Maternal and Fetal Outcome of Guillain-Barre Syndrome Complicating Pregnancy: A Case ReportDocument2 pagesSuccessful Maternal and Fetal Outcome of Guillain-Barre Syndrome Complicating Pregnancy: A Case ReportmelvaNo ratings yet
- A Practical Approach To Managing Patients With Myasthenia GravisDocument16 pagesA Practical Approach To Managing Patients With Myasthenia GravisStevanie SesiliaNo ratings yet
- 9 Illness Script 9Document2 pages9 Illness Script 9burnermyth2No ratings yet
- Whats New in Myasthenia GravisDocument39 pagesWhats New in Myasthenia Gravisadoorableepets.1o1No ratings yet
- Spinal Muscular AtrophyDocument7 pagesSpinal Muscular AtrophyJulia SalvioNo ratings yet
- Neurocritical Care of The Pregnant PatientDocument24 pagesNeurocritical Care of The Pregnant PatientRicardo Robles AlfaroNo ratings yet
- Spinal Muscular Atrophy 5Q Treatment With Nusinersen Brasilian Guideline REV MED BRAS 2018Document8 pagesSpinal Muscular Atrophy 5Q Treatment With Nusinersen Brasilian Guideline REV MED BRAS 2018Valentina GiraldoNo ratings yet
- A Study of Comorbidities in Myasthenia Gravis: Usha K. Misra Jayantee Kalita Varun K. Singh Surendra KumarDocument6 pagesA Study of Comorbidities in Myasthenia Gravis: Usha K. Misra Jayantee Kalita Varun K. Singh Surendra KumarCaroline OktarinaNo ratings yet
- Menopause 1 Bu MaeDocument7 pagesMenopause 1 Bu Maesetya riniNo ratings yet
- Myasthenia Gravis in The Elderly: NeurologyDocument4 pagesMyasthenia Gravis in The Elderly: NeurologyAirin QueNo ratings yet
- PIIS0016508506008651Document29 pagesPIIS0016508506008651Ongoongoseven b. e. bNo ratings yet
- Pumonary Tuberculosis in Pregnancy PALLAVIDocument42 pagesPumonary Tuberculosis in Pregnancy PALLAVIJyothsna DeepNo ratings yet
- Myasthenia Gravis in Clinical Practice: Miastenia Gravis Na Prática ClínicaDocument9 pagesMyasthenia Gravis in Clinical Practice: Miastenia Gravis Na Prática ClínicaMasDhedotNo ratings yet
- Metformin Vs Insulin in Gestational DiabetesDocument17 pagesMetformin Vs Insulin in Gestational Diabetesmiguel alejandro zapata olayaNo ratings yet
- NIH Public Access: Author ManuscriptDocument15 pagesNIH Public Access: Author ManuscriptAngelNo ratings yet
- NIH Public Access: Author ManuscriptDocument15 pagesNIH Public Access: Author ManuscriptAngelNo ratings yet
- Myasthenia Gravis and PregnancyDocument8 pagesMyasthenia Gravis and PregnancykalakrasiaNo ratings yet
- Putra Et Al 55-58Document4 pagesPutra Et Al 55-58arga setyo adjiNo ratings yet
- Status Epilepticus in Pregnancy A Literature Review and A ProtocolDocument12 pagesStatus Epilepticus in Pregnancy A Literature Review and A Protocolmaria arenas de ita100% (1)
- Myasthenia Gravis: Dr. Ken Wirastuti, Mkes, SP.S Bagian Ilmu Penyakit Saraf Fk. UnissulaDocument30 pagesMyasthenia Gravis: Dr. Ken Wirastuti, Mkes, SP.S Bagian Ilmu Penyakit Saraf Fk. UnissulafemmytaniaNo ratings yet
- Diabetes y EmbarazoDocument10 pagesDiabetes y EmbarazocochipinkNo ratings yet
- Dr. Andhika Djajadi - Hiperemesis GravidarumDocument12 pagesDr. Andhika Djajadi - Hiperemesis GravidarumAndhika DjajadiNo ratings yet
- Anesthetics and AnesthesiologyDocument3 pagesAnesthetics and Anesthesiologydaily of sinta fuNo ratings yet
- Referensi Jurnal Dismenore PrimerDocument7 pagesReferensi Jurnal Dismenore PrimerDanella BonivaniaNo ratings yet
- Minimising Menopausal Side Effects WhilstDocument8 pagesMinimising Menopausal Side Effects WhilstUmaimah ShahabNo ratings yet
- Migraine Is A Risk Factor For Hypertensive Disorders in Pregnancy: A Prospective Cohort StudyDocument7 pagesMigraine Is A Risk Factor For Hypertensive Disorders in Pregnancy: A Prospective Cohort Studyandrea murilloNo ratings yet
- Kung Doris Chronic MigraineDocument19 pagesKung Doris Chronic MigraineAnonymous tG35SYROzENo ratings yet
- ShowText-1 (1) UnlockedDocument5 pagesShowText-1 (1) Unlocked12ock312No ratings yet
- Final Power Point PresentationDocument69 pagesFinal Power Point PresentationjyayNo ratings yet
- Treatment of Ocular Myasthenia Gravis: Scott R. Haines, MD Matthew J. Thurtell, MBBSDocument10 pagesTreatment of Ocular Myasthenia Gravis: Scott R. Haines, MD Matthew J. Thurtell, MBBSTarun MathurNo ratings yet
- GROUP 4 (Myasthenia Gravis)Document53 pagesGROUP 4 (Myasthenia Gravis)gabrielle magdaraogNo ratings yet
- Practice FullDocument4 pagesPractice FullAya SorayaNo ratings yet
- Acog Committee Opinion: Dysmenorrhea and Endometriosis in The AdolescentDocument10 pagesAcog Committee Opinion: Dysmenorrhea and Endometriosis in The AdolescentYosep SutandarNo ratings yet
- Fardaic CurrentDocument7 pagesFardaic CurrentlecturioNo ratings yet
- Case StudyDocument1 pageCase StudyGemina Leah MaeNo ratings yet
- Eye Imaging - SAMPLE ROP Toolkit 2021Document11 pagesEye Imaging - SAMPLE ROP Toolkit 2021Johana OsorioNo ratings yet
- WHO 2018 Health at A Glance Mortality Asia Pac Region OctoberDocument3 pagesWHO 2018 Health at A Glance Mortality Asia Pac Region Octoberbiko97jcjNo ratings yet
- Hepatitis A Virus - HAV: DiagnosisDocument6 pagesHepatitis A Virus - HAV: DiagnosisnurmaliarizkyNo ratings yet
- Pathophysiology NG CandidiasisDocument2 pagesPathophysiology NG CandidiasisJan Rae Barnatia AtienzaNo ratings yet
- DIAGNOSIS: Chronic Pain Related To Disease Process As Manifested by Presence of Mass On The LegDocument5 pagesDIAGNOSIS: Chronic Pain Related To Disease Process As Manifested by Presence of Mass On The LeggrizolaNo ratings yet
- Development of The Nervous SystemDocument5 pagesDevelopment of The Nervous SystemChaGonzalesNo ratings yet
- Metabolic Responses To ExerciseDocument16 pagesMetabolic Responses To ExerciseKanyakorn AnothipNo ratings yet
- Quizlet PDFDocument4 pagesQuizlet PDFsgkismetNo ratings yet
- Presentation of Neurogenic Shock Within The Emergency Department - TaylorDocument6 pagesPresentation of Neurogenic Shock Within The Emergency Department - TaylorAnprtma kaunangNo ratings yet
- Psychological Aspect of AgingDocument4 pagesPsychological Aspect of AgingMuhammad Wachid100% (1)
- D AbuseDocument8 pagesD AbuseFrancis AngtudNo ratings yet
- Nursing ProcessDocument45 pagesNursing ProcessSukmaErfiana100% (1)
- Combine Class Chronic Inflammation & Wound Healing (Power Point)Document35 pagesCombine Class Chronic Inflammation & Wound Healing (Power Point)Suleiman KikulweNo ratings yet
- Microsoft Word - NBME 12 ANSWERS LongDocument13 pagesMicrosoft Word - NBME 12 ANSWERS LongoffdanNo ratings yet
- MS Vision Problems - How MS Causes Blurry Vision and Eye PainDocument3 pagesMS Vision Problems - How MS Causes Blurry Vision and Eye PainAndreea PleșaNo ratings yet
- Update On Stemi Management: Dr. Adi Purnawarman, SP - JP (K) - Fiha.,FasccDocument39 pagesUpdate On Stemi Management: Dr. Adi Purnawarman, SP - JP (K) - Fiha.,FasccArfiska Ridha Fausa 'ucha'No ratings yet
- Vice and DrugDocument8 pagesVice and DrugTIPAY, EMELIE L.No ratings yet
- Breast Cancer Differential DiagnosesDocument5 pagesBreast Cancer Differential DiagnosesRayhanun MardhatillahNo ratings yet
- Chronic Transaminitis 07Document39 pagesChronic Transaminitis 07Jessica GarletsNo ratings yet
- Nutrition During Infancy: Presented By: Group 3Document50 pagesNutrition During Infancy: Presented By: Group 3Lynette EspejoNo ratings yet
- Nephrology TestDocument22 pagesNephrology TestRishi KNair100% (1)
- Muskuloskelatal (English) : Senin Selasa Rabu Kamis JumatDocument3 pagesMuskuloskelatal (English) : Senin Selasa Rabu Kamis JumatArsul RNo ratings yet
- 5ykgogrgmtd3pwbpedotjsidDocument10 pages5ykgogrgmtd3pwbpedotjsidKartik SharmaNo ratings yet
- Clinically Diagnosed Postoperative Venous Thromboembolism in A NeurosurgeryDocument7 pagesClinically Diagnosed Postoperative Venous Thromboembolism in A Neurosurgerydonira73No ratings yet
- Respiratory Diagnostic ProceduresDocument41 pagesRespiratory Diagnostic Proceduresseigelystic100% (23)
- Concurrent Acute Poststreptococcal Glomerulonephritis andDocument42 pagesConcurrent Acute Poststreptococcal Glomerulonephritis andKardio UndipNo ratings yet
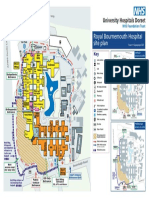
- Royal Bournemouth Hospital Site Plan: A338 Wessex Wa yDocument1 pageRoyal Bournemouth Hospital Site Plan: A338 Wessex Wa ydolar buhaNo ratings yet