Download as pdf or txt
You might also like
- Eu Private International Law PDFDocument2 pagesEu Private International Law PDFRojo0% (1)
- Personal Best A1 Unit 8 Reading TestDocument3 pagesPersonal Best A1 Unit 8 Reading TestLuis Fernando Osorio SanchezNo ratings yet
- Ipaf 2019Document10 pagesIpaf 2019Edoardo CavigliNo ratings yet
- Caracterizacion IpafDocument9 pagesCaracterizacion Ipafpkh5qpp8j5No ratings yet
- Richeldi Et Al 2021 Utility of A Molecular Classifier As A Complement To High Resolution Computed Tomography ToDocument10 pagesRicheldi Et Al 2021 Utility of A Molecular Classifier As A Complement To High Resolution Computed Tomography Toحسام الوجيهNo ratings yet
- Analisis Comparativo Ipaf Vs EasDocument9 pagesAnalisis Comparativo Ipaf Vs Easpkh5qpp8j5No ratings yet
- Fimmu 15 1353012Document9 pagesFimmu 15 1353012tatiana.balanici13No ratings yet
- Fungalinfections in The Icu: Marya D. Zilberberg,, Andrew F. ShorrDocument18 pagesFungalinfections in The Icu: Marya D. Zilberberg,, Andrew F. ShorrGiselle BaiãoNo ratings yet
- Ipaf 2022Document8 pagesIpaf 2022pkh5qpp8j5No ratings yet
- Jurnal 9 OKKDocument4 pagesJurnal 9 OKKpencari pencerahan45No ratings yet
- Diagnostic Utility of Clinical Laboratory Data Determinations For Patients With The Severe COVID-19Document18 pagesDiagnostic Utility of Clinical Laboratory Data Determinations For Patients With The Severe COVID-19Carla CANo ratings yet
- JMV 26509Document12 pagesJMV 26509a27091No ratings yet
- Severe Covid and Autoimmune DiseaseDocument4 pagesSevere Covid and Autoimmune DiseaseYudha SatriaNo ratings yet
- AzithromycinDocument7 pagesAzithromycinRoamersiaNo ratings yet
- Improving Risk Stratification of Rheumatoid Arthritis Patients For Intestinal Lung DiseasesDocument11 pagesImproving Risk Stratification of Rheumatoid Arthritis Patients For Intestinal Lung DiseasesdopiorototoNo ratings yet
- PIIS0022510X20304998Document7 pagesPIIS0022510X20304998dhea handyaraNo ratings yet
- RMV 2225Document18 pagesRMV 2225Iziza LunaskhiNo ratings yet
- 699-Article Text-1085-1-10-20181101Document6 pages699-Article Text-1085-1-10-20181101Shahid HussainNo ratings yet
- Idiopathic Pulmonary Fibrosis: Diagnosis, Epidemiology and Natural HistoryDocument11 pagesIdiopathic Pulmonary Fibrosis: Diagnosis, Epidemiology and Natural HistorySuwandi AlghozyNo ratings yet
- Systemic Immune-In Ammatory Index Predicts Prognosis of Patients With COVID-19: A Retrospective StudyDocument37 pagesSystemic Immune-In Ammatory Index Predicts Prognosis of Patients With COVID-19: A Retrospective StudyJuliana SanjayaNo ratings yet
- NIH Public Access: Author ManuscriptDocument23 pagesNIH Public Access: Author ManuscriptntnquynhproNo ratings yet
- JAPI0200 p19-24 CompressedDocument6 pagesJAPI0200 p19-24 Compressedsachin kulkarniNo ratings yet
- Alopecia y CovidDocument9 pagesAlopecia y CovidFernanda cisneros ContrerasNo ratings yet
- Acute Respiratory Failure Due To Pneumocystis Pneumonia: Outcome and Prognostic FactorsDocument8 pagesAcute Respiratory Failure Due To Pneumocystis Pneumonia: Outcome and Prognostic FactorszikryauliaNo ratings yet
- Gouzien 2021Document4 pagesGouzien 2021Andreea CiorneaNo ratings yet
- Neumonia AspirativaDocument9 pagesNeumonia AspirativaMileth GonzalezNo ratings yet
- Interstitial Pneumonia With Autoimmune Features IPAF Time To Redefine The Classification CriteriaDocument4 pagesInterstitial Pneumonia With Autoimmune Features IPAF Time To Redefine The Classification CriteriaLuis Guillermo Buitrago BuitragoNo ratings yet
- Journal Pone 0252599Document12 pagesJournal Pone 0252599sririniaNo ratings yet
- D'alessandro 2020Document5 pagesD'alessandro 2020Flip Flop ChartNo ratings yet
- 1 s2.0 S0163445320302085 Main PDFDocument7 pages1 s2.0 S0163445320302085 Main PDFJorgeNo ratings yet
- Impacto NeumologíaDocument13 pagesImpacto NeumologíaNilda MoraNo ratings yet
- 2023 9371Document6 pages2023 9371Ibad RahmanNo ratings yet
- Review Mortality in Tocilizumab-Treated Patients With COVID-19: A Systematic Review and Meta-AnalysisDocument8 pagesReview Mortality in Tocilizumab-Treated Patients With COVID-19: A Systematic Review and Meta-AnalysisJacobNo ratings yet
- PIIS1076633220302464Document1 pagePIIS1076633220302464India SunshineNo ratings yet
- Rjme 63 2 413Document7 pagesRjme 63 2 413angelNo ratings yet
- Vaccines 10 01233Document21 pagesVaccines 10 01233FERNANDO CHEVARRIA MUÑIZNo ratings yet
- COVID 19 Articulo MilordDocument11 pagesCOVID 19 Articulo MilordHector MartinezNo ratings yet
- RISK of Thromboembolism in Patient With Covid 19 MétaanalysisDocument14 pagesRISK of Thromboembolism in Patient With Covid 19 MétaanalysisDelgado OnthemixNo ratings yet
- RASmodelforCOVID 19publishedinternationalarticleDocument13 pagesRASmodelforCOVID 19publishedinternationalarticleJulio VelazquezNo ratings yet
- All Articles Certs 27 Aug UpdatedDocument42 pagesAll Articles Certs 27 Aug Updatedmohammadrezahajian12191No ratings yet
- Characteristics of Chronic Cough in Adults in Pakistani Population: A Cross Sectional StudyDocument5 pagesCharacteristics of Chronic Cough in Adults in Pakistani Population: A Cross Sectional StudylupNo ratings yet
- Journal Pre-Proof: International Journal of Infectious DiseasesDocument14 pagesJournal Pre-Proof: International Journal of Infectious DiseasesKenya EspinozaNo ratings yet
- Rüthrich2021 Article COVID-19InCancerPatientsClinicDocument11 pagesRüthrich2021 Article COVID-19InCancerPatientsClinicdianaNo ratings yet
- Mortalidad PardsDocument9 pagesMortalidad PardsBarbara Seminario RamirezNo ratings yet
- Risk Factors For Community-Acquired Pneumonia in Adults in Europe: A Literature ReviewDocument11 pagesRisk Factors For Community-Acquired Pneumonia in Adults in Europe: A Literature ReviewKorwin TitlaNo ratings yet
- Immune Response To Sars-Cov-2 and Mechanisms of Immunopathological Changes in Covid-19Document18 pagesImmune Response To Sars-Cov-2 and Mechanisms of Immunopathological Changes in Covid-19Ayu MayangsariNo ratings yet
- COVID-19-Associated Pulmonary Aspergillosis (CAPA)Document11 pagesCOVID-19-Associated Pulmonary Aspergillosis (CAPA)Awal SafarNo ratings yet
- Diagnostic Utility of Clinical Laboratory Data Determinationsfor Patients With The Severe COVID 19Document6 pagesDiagnostic Utility of Clinical Laboratory Data Determinationsfor Patients With The Severe COVID 19junior rodriguesNo ratings yet
- The Hemocyte Counts As A Potential Biomarker For Predicting Disease Progression in COVID-19: A Retrospective StudyDocument10 pagesThe Hemocyte Counts As A Potential Biomarker For Predicting Disease Progression in COVID-19: A Retrospective StudygiovannaNo ratings yet
- Coronavirus (2019 Ncov) Selected Bibliographic References 12 02 2020 v1Document6 pagesCoronavirus (2019 Ncov) Selected Bibliographic References 12 02 2020 v1Andi SanapatiNo ratings yet
- Neutrofilos y LinfocitosDocument2 pagesNeutrofilos y LinfocitosOscarNo ratings yet
- Early Intervention Can Improve Clinical Outcome of Acute Interstitial PneumoniaDocument9 pagesEarly Intervention Can Improve Clinical Outcome of Acute Interstitial PneumoniaHerbert Baquerizo VargasNo ratings yet
- Chest X Ray in CAPDocument7 pagesChest X Ray in CAPsahatmanurungNo ratings yet
- Ahead of Print: Establishment of Diagnostic Protocols For COVID-19 PatientsDocument6 pagesAhead of Print: Establishment of Diagnostic Protocols For COVID-19 PatientsSana AbbasNo ratings yet
- Pneumonia Severity Index in Viral Community Acquired Pneumonia in AdultsDocument12 pagesPneumonia Severity Index in Viral Community Acquired Pneumonia in Adultsmuhammad_ariefNo ratings yet
- Plasma Cytokine Profile On Admission Related To Aetiology in Community Acquired PneumoniaDocument9 pagesPlasma Cytokine Profile On Admission Related To Aetiology in Community Acquired Pneumoniahusni gunawanNo ratings yet
- Ann Clin Transl Neurol - 2021 - Han - Increased Atrial Fibrillation Risk in Parkinson S Disease A NationwideDocument9 pagesAnn Clin Transl Neurol - 2021 - Han - Increased Atrial Fibrillation Risk in Parkinson S Disease A NationwideFrancisco Silvosa FernandezNo ratings yet
- Automatic COVID 19 Severity Assessment From HRVDocument10 pagesAutomatic COVID 19 Severity Assessment From HRVCarlos Eduardo NorteNo ratings yet
- Aspergillus Galactomannan Lateral FlowDocument13 pagesAspergillus Galactomannan Lateral FlowLuiseNo ratings yet
- RMV 2107Document6 pagesRMV 2107Ahmed AllamNo ratings yet
- Covid UpdateDocument25 pagesCovid UpdateAndreea PostolacheNo ratings yet
- Living on the Frontline of COVID-19 in MCO And CMCOFrom EverandLiving on the Frontline of COVID-19 in MCO And CMCONo ratings yet
- Superior Court of California County of Santa Clara Civil DivisionDocument30 pagesSuperior Court of California County of Santa Clara Civil DivisionMitchNo ratings yet
- CS1352 May07Document19 pagesCS1352 May07sridharanc23No ratings yet
- Air Is Allowed To Flow From A Large Reservoir ThroDocument3 pagesAir Is Allowed To Flow From A Large Reservoir Throsid202pkNo ratings yet
- HZ2322 EM250 Series 100mW ZigBee Module (ENG)Document10 pagesHZ2322 EM250 Series 100mW ZigBee Module (ENG)MicroComSolutionsNo ratings yet
- (Lines - of - Thought - ) Robert - C. - Stalnaker-Our - Knowledge - of - The - Internal - World - (Lines - of - Thought) - Oxford - University - Press, - USA (2008) (1) by Stalnaker PDFDocument20 pages(Lines - of - Thought - ) Robert - C. - Stalnaker-Our - Knowledge - of - The - Internal - World - (Lines - of - Thought) - Oxford - University - Press, - USA (2008) (1) by Stalnaker PDFPriyanka DeNo ratings yet
- Tifr SSRDocument972 pagesTifr SSRAbhishek UpadhyayNo ratings yet
- Module 2 TheoDocument6 pagesModule 2 TheoMichlee Joy Paguila LagocNo ratings yet
- MIJIDocument17 pagesMIJIpranilNo ratings yet
- Standard Precautions Knowledge and Practice Among Radiographers in Sri LankaDocument8 pagesStandard Precautions Knowledge and Practice Among Radiographers in Sri LankaSachin ParamashettiNo ratings yet
- Install Ruby On Rails in RVMDocument5 pagesInstall Ruby On Rails in RVMAsep MulyanaNo ratings yet
- The God in The Flower Pot Mary BarnardDocument4 pagesThe God in The Flower Pot Mary BarnarddianaNo ratings yet
- Rle Week 7 Bed Bath DocsDocument2 pagesRle Week 7 Bed Bath DocsCHRISTINE KEITH NEPOMUCENONo ratings yet
- The Manchester Gamba BookDocument180 pagesThe Manchester Gamba BookFredrik Hildebrand100% (2)
- Ceramic TilesDocument340 pagesCeramic TilesMihai ȘtefanNo ratings yet
- General Knowlege QuestionsDocument36 pagesGeneral Knowlege QuestionsSarahNo ratings yet
- Unit 19 p3Document10 pagesUnit 19 p3api-344079053No ratings yet
- Kariuki, Alex K - Impact of Information Technology On Organizational Performance Case of Population Services KenyaDocument52 pagesKariuki, Alex K - Impact of Information Technology On Organizational Performance Case of Population Services KenyaJack JaviNo ratings yet
- 21B Oracle Workforce ManagementDocument27 pages21B Oracle Workforce ManagementRam81No ratings yet
- Letter of Inquiry About Internship Opportunities - HardDocument1 pageLetter of Inquiry About Internship Opportunities - Hardapi-370641050% (2)
- Course Title Understanding Culture, Society, & Politics Instructor Mieca Aguinaldo Course Code Course DescriptionDocument6 pagesCourse Title Understanding Culture, Society, & Politics Instructor Mieca Aguinaldo Course Code Course DescriptionSJHC 21No ratings yet
- Korea IT TimesDocument76 pagesKorea IT TimesDilek KarahocaNo ratings yet
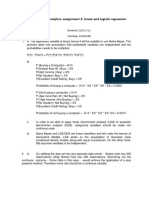
- Business Analytics AssignmentDocument3 pagesBusiness Analytics AssignmentDevansh RaiNo ratings yet
- The Champion Legal Ads: 06-30-22Document46 pagesThe Champion Legal Ads: 06-30-22Donna S. SeayNo ratings yet
- Lesson Plan For BEEEDocument18 pagesLesson Plan For BEEEdineshanand810100% (1)
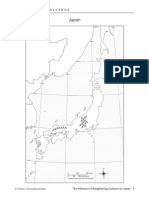
- Influence of Nieghbors On Japan Student NotebookDocument9 pagesInfluence of Nieghbors On Japan Student Notebookapi-233464494No ratings yet
- Fy2023 FWS Budget RequestDocument8 pagesFy2023 FWS Budget RequestinforumdocsNo ratings yet
- Chapter04.pdf - How To Write A Project Report - ResearchDocument8 pagesChapter04.pdf - How To Write A Project Report - Researchbrownsugar26No ratings yet
- Angela's Infantwear and Accessories: InvoiceDocument1 pageAngela's Infantwear and Accessories: InvoiceAngelas InfantwearNo ratings yet