Download as pdf or txt
You might also like
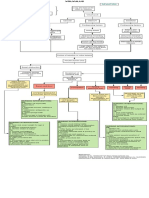
- Concept Map On AppendicitisDocument6 pagesConcept Map On Appendicitisitalisayan_rondario80% (5)
- Shannon Hanchett Autopsy ReportDocument1 pageShannon Hanchett Autopsy ReportOKCFOXNo ratings yet
- Nursing Care Plan CholecystectomyDocument2 pagesNursing Care Plan Cholecystectomyderic87% (23)
- Nursing Care Plan Abruptio PlacentaeDocument2 pagesNursing Care Plan Abruptio Placentaederic93% (29)
- Concept Map of Acute PancreatitisDocument2 pagesConcept Map of Acute Pancreatitissalome carpioNo ratings yet
- Neurogenic BladderDocument11 pagesNeurogenic BladderRoy LiemNo ratings yet
- Jurnal OG 1Document6 pagesJurnal OG 1Wa Ode Meutya ZawawiNo ratings yet
- Catheterization HANDOUTSDocument9 pagesCatheterization HANDOUTSYalc LapidNo ratings yet
- CatheterizationDocument11 pagesCatheterizationSJ MNo ratings yet
- 4.physiology of Micturition PDFDocument20 pages4.physiology of Micturition PDFNaimish VermaNo ratings yet
- Nursing Care Plan Abrubtio PlacentaDocument2 pagesNursing Care Plan Abrubtio PlacentaLei Ortega0% (1)
- Mechanism of MicturitionDocument4 pagesMechanism of MicturitionGerardLum100% (2)
- Lec15 - Renal SystemDocument3 pagesLec15 - Renal SystemGeorge Constante Valiente-SebastianNo ratings yet
- L4 MicturitionDocument26 pagesL4 MicturitionAlimahtabNo ratings yet
- Nursing Care Plan Ectopic PregnancyDocument2 pagesNursing Care Plan Ectopic PregnancyLei Ortega94% (36)
- INTUSSUSCEPTIONDocument1 pageINTUSSUSCEPTIONMaecy PasionNo ratings yet
- Web of Caution (WOC) Ca. ServiksDocument3 pagesWeb of Caution (WOC) Ca. ServiksAndreas Panda BanjalNo ratings yet
- Pathophysiology of Benign Prostatic HyperplasiaDocument1 pagePathophysiology of Benign Prostatic HyperplasiaErika BernardinoNo ratings yet
- Normal KUB-IVP: GUT ViewboxDocument17 pagesNormal KUB-IVP: GUT ViewboxtabatchNo ratings yet
- Impaired Urinary EliminationDocument2 pagesImpaired Urinary EliminationSiafei RabeNo ratings yet
- Seminar 15 - UTIDocument41 pagesSeminar 15 - UTIBONG AIKCHINGNo ratings yet
- PerineumDocument7 pagesPerineumapi-3812135No ratings yet
- Nursing Care Plan Risk For Uterine InfectionDocument4 pagesNursing Care Plan Risk For Uterine Infectionderic97% (30)
- Pathophysiology of Ovarian CystDocument3 pagesPathophysiology of Ovarian CystLuayon FrancisNo ratings yet
- Testicular Torsion, Peds Cases NotesDocument1 pageTesticular Torsion, Peds Cases NotesdzalhcNo ratings yet
- Fisiologi DefekasiDocument9 pagesFisiologi DefekasiAmirullah AbdiNo ratings yet
- Urinary IncontinenceDocument1 pageUrinary IncontinenceZiyad100% (1)
- Testicular Torsion: Journal ReadingDocument14 pagesTesticular Torsion: Journal ReadingRizkiYudaPurnomoNo ratings yet
- MicturitionDocument7 pagesMicturitionOsama MohamedNo ratings yet
- Bladder IrrigationDocument3 pagesBladder IrrigationMyfanway Am-isNo ratings yet
- Abdominal Inury 2Document8 pagesAbdominal Inury 2Chol Koryom CholNo ratings yet
- Chap 23Document25 pagesChap 23Ghazian AdliNo ratings yet
- Physiology of Micturition Reflex PDFDocument37 pagesPhysiology of Micturition Reflex PDFVanathy KarunamoorthyNo ratings yet
- Ipm 2Document3 pagesIpm 2Fritzienico BaskoroNo ratings yet
- PP Exam 4: Everything That Is in Red Came From Test Your Knowledge!Document15 pagesPP Exam 4: Everything That Is in Red Came From Test Your Knowledge!netanya DoanNo ratings yet
- Benign Prostatic HyperplasiaDocument5 pagesBenign Prostatic Hyperplasiatabangin_hilario100% (1)
- Clinical Course Discussion: Oregon Health & Science University, Portland, OregonDocument1 pageClinical Course Discussion: Oregon Health & Science University, Portland, OregonperjadanutNo ratings yet
- 6 SURGERY II 6 - Pediatric UrologyDocument6 pages6 SURGERY II 6 - Pediatric UrologyDeann RoscomNo ratings yet
- Nursing Care Plan For Peritonitis NCPDocument2 pagesNursing Care Plan For Peritonitis NCPyamie sulongNo ratings yet
- Case Study: Lower Gastrointestinal Bleeding Secondary To DiverticulitisDocument14 pagesCase Study: Lower Gastrointestinal Bleeding Secondary To DiverticulitisKevin Cloyd BragasNo ratings yet
- Fluid and ElectrolytesDocument21 pagesFluid and ElectrolytesKc Cabanilla LizardoNo ratings yet
- SABISTON AnoDocument24 pagesSABISTON AnosantigarayNo ratings yet
- Fecal Elimination, Hayam?Document5 pagesFecal Elimination, Hayam?Aryam SNo ratings yet
- Shoulder 1 PDFDocument3 pagesShoulder 1 PDFRyan Joseph GaholNo ratings yet
- Normal Deviation: Imbalanced Nutrtion: Less Than Body Requirements R/T Gastrointestinal ObstructionDocument1 pageNormal Deviation: Imbalanced Nutrtion: Less Than Body Requirements R/T Gastrointestinal ObstructionMaecy PasionNo ratings yet
- Bladder Innervation Physiology of Micturition Voiding DysfunctionDocument77 pagesBladder Innervation Physiology of Micturition Voiding DysfunctionKoushik Sharma AmancharlaNo ratings yet
- Chapter-7-Pathophysiology Nephrotic SyndromeDocument3 pagesChapter-7-Pathophysiology Nephrotic SyndromeCxarina RamirezNo ratings yet
- The Perfect Ic Diet Cookbook The Complete Nutrition Guide To Healing Chronic Pelvic Pain And Managing Symptoms Of Interstitial Cystitis With Delectable And Nourishing RecipesFrom EverandThe Perfect Ic Diet Cookbook The Complete Nutrition Guide To Healing Chronic Pelvic Pain And Managing Symptoms Of Interstitial Cystitis With Delectable And Nourishing RecipesNo ratings yet
- Dictionary of Veterinary Terms: Vet-Speak Deciphered for the Non VeterinarianFrom EverandDictionary of Veterinary Terms: Vet-Speak Deciphered for the Non VeterinarianNo ratings yet
- Conquering Incontinence: A new and physical approach to a freer lifestyleFrom EverandConquering Incontinence: A new and physical approach to a freer lifestyleNo ratings yet
- Female Arousal and Orgasm: Anatomy, Physiology, Behaviour and EvolutionFrom EverandFemale Arousal and Orgasm: Anatomy, Physiology, Behaviour and EvolutionNo ratings yet
- The Perfect Pancreatitis Diet Cookbook; The Complete Nutrition Guide To Managing And Healing Pancreatitis With Delectable And Nourishing Recipes;From EverandThe Perfect Pancreatitis Diet Cookbook; The Complete Nutrition Guide To Managing And Healing Pancreatitis With Delectable And Nourishing Recipes;No ratings yet
- Drug Study of FluoxetineDocument2 pagesDrug Study of FluoxetineLance De GuzmanNo ratings yet
- Genetics and Oral HealthDocument16 pagesGenetics and Oral Healthsalah jerbiNo ratings yet
- 63c18da748714 Basic Geriatric Nursing 7th Edition Williams Test Bank px8nzf PDFDocument108 pages63c18da748714 Basic Geriatric Nursing 7th Edition Williams Test Bank px8nzf PDFerickomusiq7100% (1)
- Disorders of Parathyroid GlandsDocument52 pagesDisorders of Parathyroid GlandsDr. Akash GuptaNo ratings yet
- CheatsheetsDocument2 pagesCheatsheetsprosie392No ratings yet
- SCP Infection ControlDocument7 pagesSCP Infection ControlNoreen PunjwaniNo ratings yet
- Belize Medical Fitness CertificateDocument2 pagesBelize Medical Fitness CertificateSea BlackNo ratings yet
- OceanofPDF - Com Why Charlie Brown Why - Charles M SchulzDocument70 pagesOceanofPDF - Com Why Charlie Brown Why - Charles M SchulzKarabo LetsholoNo ratings yet
- Nursing Worksheet Template 1 1Document2 pagesNursing Worksheet Template 1 1api-651287771No ratings yet
- Flagellates LabDocument4 pagesFlagellates LabWilliam RamirezNo ratings yet
- Large: Primary Adrenocortical Deficiency Pernicious AnemiaDocument28 pagesLarge: Primary Adrenocortical Deficiency Pernicious Anemiawaqasmumtaz12No ratings yet
- Dr. Ali's Uworld Notes For Step 2 CKDocument15 pagesDr. Ali's Uworld Notes For Step 2 CKBoogy WoogyNo ratings yet
- Surgical Treatment of Gastric Cancer Then and NowDocument8 pagesSurgical Treatment of Gastric Cancer Then and NowConstantin BudinNo ratings yet
- Department of Education Division of Leyte Taberna National High SchoolDocument6 pagesDepartment of Education Division of Leyte Taberna National High SchoolSheila May Tapales TabonNo ratings yet
- PESTEL AnalysisDocument7 pagesPESTEL AnalysiszenerdiodeNo ratings yet
- Rs Foreign Body AspirationDocument50 pagesRs Foreign Body AspirationDr.P.NatarajanNo ratings yet
- Solid Waste ManagementDocument40 pagesSolid Waste ManagementMark Jacartny TuyongNo ratings yet
- Full Download PDF of Medical Secrets 6th Edition Mary P. Harward - Ebook PDF All ChapterDocument69 pagesFull Download PDF of Medical Secrets 6th Edition Mary P. Harward - Ebook PDF All Chapterphakhijayahr100% (7)
- Midterm Psych NSG Nclex Test BanksDocument19 pagesMidterm Psych NSG Nclex Test BanksAliza AlyyNo ratings yet
- Varicose Vein - Management, DVT: BY Anandhu Lal Anjali P K AnjusjDocument108 pagesVaricose Vein - Management, DVT: BY Anandhu Lal Anjali P K AnjusjAsif AbbasNo ratings yet
- Eü Szaknyelvi AngolDocument44 pagesEü Szaknyelvi AngolKissné Makai KataNo ratings yet
- Smoking, Mental Illness, and Public Health: FurtherDocument24 pagesSmoking, Mental Illness, and Public Health: FurtherIndriani BaharuddinNo ratings yet
- Minimally Invasive Gynecologic SurgeryDocument25 pagesMinimally Invasive Gynecologic SurgerySamir CastilloNo ratings yet
- DR Suraya Hani Kamsani Paediatrics Dept Hosp SegamatDocument25 pagesDR Suraya Hani Kamsani Paediatrics Dept Hosp Segamatshk229No ratings yet
- Government of Rajasthan Finance Department Rules DivisionDocument2 pagesGovernment of Rajasthan Finance Department Rules DivisionSadanand PariharNo ratings yet
- Werewolf - Curse of The Otolleys BurgerDocument7 pagesWerewolf - Curse of The Otolleys BurgerVictor LewisNo ratings yet
- 10 Penyakit Terbanyak Di Rawat Jalan Di Puskesmas Provinsi Dki Jakarta TW I Tahun 2019Document9 pages10 Penyakit Terbanyak Di Rawat Jalan Di Puskesmas Provinsi Dki Jakarta TW I Tahun 2019Klinik pratama Iqra' medical centreNo ratings yet
- Wound Management in Urgent CareDocument93 pagesWound Management in Urgent CareFahmi RizalNo ratings yet
- Microbiology and ParasitologyDocument55 pagesMicrobiology and ParasitologyJade BuriNo ratings yet