Download as pdf or txt
You might also like
- Grading Systems and The Grading System of The Department of EducationDocument5 pagesGrading Systems and The Grading System of The Department of EducationAngela Quezada Rulete67% (3)
- Patanjali Project ReportDocument56 pagesPatanjali Project ReportJanvi SinghNo ratings yet
- Case Report FenitoinDocument4 pagesCase Report FenitoinDita HarefaNo ratings yet
- Br. J. Anaesth.-2012-Perks-562-71 - Anesthesia and EpilepsyDocument10 pagesBr. J. Anaesth.-2012-Perks-562-71 - Anesthesia and EpilepsyGustavo Viveros MNo ratings yet
- Goulet 1992Document6 pagesGoulet 1992DANIEL - PRISMANo ratings yet
- PIIS1059131122002151Document9 pagesPIIS1059131122002151Francisco XicohtencatlNo ratings yet
- Diagnosis and Management of HIV Drug Hypersensitivity: Current PerspectivesDocument12 pagesDiagnosis and Management of HIV Drug Hypersensitivity: Current Perspectivesdafidpra1612No ratings yet
- Advocating For Demonstration of Disease Modification - Have We Been Approaching Clinical Trials in Early Alzheimer Disease Incorrectly?Document2 pagesAdvocating For Demonstration of Disease Modification - Have We Been Approaching Clinical Trials in Early Alzheimer Disease Incorrectly?Lorrane NevesNo ratings yet
- Venlafaxine demonstrated anti‑arthritic activity possibly through down regulation of TNF‑α, IL‑6, IL‑1β, and COX‑2Document13 pagesVenlafaxine demonstrated anti‑arthritic activity possibly through down regulation of TNF‑α, IL‑6, IL‑1β, and COX‑2thqhospital lalianNo ratings yet
- Antibiotic Associated EncephalopathyDocument9 pagesAntibiotic Associated EncephalopathyAmila Atic JasarevicNo ratings yet
- Beghi Et Al 2011 EpilepsiaDocument5 pagesBeghi Et Al 2011 Epilepsiahendra_padangNo ratings yet
- Api FDocument9 pagesApi FRamon Lopez MartinezNo ratings yet
- Pharmacology of HIV RXDocument10 pagesPharmacology of HIV RXdupuytrenNo ratings yet
- DRESS Syndrome A Literature Review and TreatmentDocument12 pagesDRESS Syndrome A Literature Review and TreatmentAlyando drNo ratings yet
- Antipyretic Efficacy of Acetaminophen And.34Document8 pagesAntipyretic Efficacy of Acetaminophen And.34YULISSA FLORES RONDONNo ratings yet
- 34 1481879445 PDFDocument6 pages34 1481879445 PDFFebby da costaNo ratings yet
- Drug Reaction With Eosinophilia and Systemic Symptoms (DRESS) Syndrome in Pediatrics. Clinical CaseDocument5 pagesDrug Reaction With Eosinophilia and Systemic Symptoms (DRESS) Syndrome in Pediatrics. Clinical CaseKelitaGonzalezNo ratings yet
- Drug Interaction Between Valproic Acid and Carbapenems in Patients With Epileptic SeizuresDocument7 pagesDrug Interaction Between Valproic Acid and Carbapenems in Patients With Epileptic SeizuresAchmad YunusNo ratings yet
- Pharmacogenetics and Pharmacogenomics in Moderate-to-Severe PsoriasisDocument14 pagesPharmacogenetics and Pharmacogenomics in Moderate-to-Severe PsoriasisDian Arief PutraNo ratings yet
- New Drugs ArtritisDocument13 pagesNew Drugs ArtritisqfecrespoNo ratings yet
- Department of Neurology, General Hospital Dr. Soetomo, SurabayaDocument7 pagesDepartment of Neurology, General Hospital Dr. Soetomo, SurabayaSundas Ijaz AwanNo ratings yet
- Sedative Effects of Antihistamines: Safety, Performance, Learning, and Quality of LifeDocument17 pagesSedative Effects of Antihistamines: Safety, Performance, Learning, and Quality of Lifesaurabhvij82No ratings yet
- Diclocenaco Ynitratos CPREDocument9 pagesDiclocenaco Ynitratos CPREPaola LastraNo ratings yet
- Drug Interaction Between Valproic Acid and CarbapeDocument7 pagesDrug Interaction Between Valproic Acid and CarbapefiqriNo ratings yet
- Standards of Laboratory Practice: Antiepileptic Drug MonitoringDocument11 pagesStandards of Laboratory Practice: Antiepileptic Drug MonitoringDiegoAndrésYiZapataNo ratings yet
- EtravirineDocument3 pagesEtravirineRosher Deliman JanoyanNo ratings yet
- Anaesthesia and EpilepsyDocument10 pagesAnaesthesia and EpilepsyrYanDYNo ratings yet
- Severe Interaction Between Ritonavir and Acenocoumarol: Annals of Pharmacotherapy May 2002Document4 pagesSevere Interaction Between Ritonavir and Acenocoumarol: Annals of Pharmacotherapy May 2002Alexandra AioaneiNo ratings yet
- For The Clinician: Pharmacology Behind Common Drug NephrotoxicitiesDocument12 pagesFor The Clinician: Pharmacology Behind Common Drug NephrotoxicitiesKarla HernándezNo ratings yet
- Therapeutic Drug Monitoring: An Overview of Commonly Monitored DrugsDocument7 pagesTherapeutic Drug Monitoring: An Overview of Commonly Monitored DrugsSerley WulandariNo ratings yet
- Prevention of Contrast Induced Renal FailureDocument13 pagesPrevention of Contrast Induced Renal Failurenaxo128No ratings yet
- Status Convulsivus RefractarioDocument10 pagesStatus Convulsivus RefractarioMisael Moreno SanchezNo ratings yet
- The Patterns of Toxicity and Management of Acute Nonsteroidal Anti-Inflammatory Drug (NSAID) OverdoseDocument10 pagesThe Patterns of Toxicity and Management of Acute Nonsteroidal Anti-Inflammatory Drug (NSAID) OverdoseDevi Dwi AmaliaNo ratings yet
- Clinical Microbiology: Open Access: The Mechanisms of Adverse Reactions To Oseltamivir: Part II. Delayed Type ReactionsDocument10 pagesClinical Microbiology: Open Access: The Mechanisms of Adverse Reactions To Oseltamivir: Part II. Delayed Type ReactionsAryanto DedyNo ratings yet
- Journal ReadingDocument6 pagesJournal ReadingInka Nadya TriayeshaNo ratings yet
- Update On The Management of Status EpilepticusDocument10 pagesUpdate On The Management of Status EpilepticusDr RICHARD PEÑA VENEZUELANo ratings yet
- Norepinephrine Kinetics and Dynamics in Septic Shock and Trauma PatientsDocument7 pagesNorepinephrine Kinetics and Dynamics in Septic Shock and Trauma PatientsMoh SuriyawalNo ratings yet
- Wang 2017Document10 pagesWang 2017vania adheliaNo ratings yet
- IJBMS Volume 12 Issue 3 Pages 146-149Document4 pagesIJBMS Volume 12 Issue 3 Pages 146-149TanveerNo ratings yet
- Nejmoa 1804092Document11 pagesNejmoa 1804092Daniel GuérinNo ratings yet
- 2013 Article 325 PDFDocument14 pages2013 Article 325 PDFKadek MahariniNo ratings yet
- Levetiracetam in Refractory Pediatric EpilepsyDocument11 pagesLevetiracetam in Refractory Pediatric EpilepsyAdlinaNo ratings yet
- Optimizar Anticonvul, VIHDocument4 pagesOptimizar Anticonvul, VIHDra Carolina Escalante Neurologa de AdultosNo ratings yet
- 17 Chhibber 2012 - Evidence-Based Review of Therapeutic Plasma Exchange in Neurological DisordersDocument9 pages17 Chhibber 2012 - Evidence-Based Review of Therapeutic Plasma Exchange in Neurological DisordersfitriNo ratings yet
- Encefalitis Autoinmune Clínica y Avances en BiologíaDocument14 pagesEncefalitis Autoinmune Clínica y Avances en BiologíaalmarazneurologiaNo ratings yet
- Neuropsychiatric Adverse Effects of Antibacterial Agents: Santa Treasa Cyriac, Divya Sara IypeDocument8 pagesNeuropsychiatric Adverse Effects of Antibacterial Agents: Santa Treasa Cyriac, Divya Sara IypevinayNo ratings yet
- Sup Ped 121401Document28 pagesSup Ped 121401PRINCESASLUKNo ratings yet
- Nephrotic SyndromeDocument13 pagesNephrotic SyndromeImanuel Far-FarNo ratings yet
- Inmuno NefritisDocument6 pagesInmuno Nefritisjuan david castillo campoNo ratings yet
- 2008 - Antituberculosis Drug-Induced Hepatotoxicity Concise Up-To-Date ReviewDocument12 pages2008 - Antituberculosis Drug-Induced Hepatotoxicity Concise Up-To-Date ReviewCarlos LuqueNo ratings yet
- The Effect of Non-Steroidal Anti-Inflammatory Drugs On Severity of Acute Pancreatitis and Pancreatic NecrosisDocument4 pagesThe Effect of Non-Steroidal Anti-Inflammatory Drugs On Severity of Acute Pancreatitis and Pancreatic NecrosisAracelyAcostaNo ratings yet
- Efficacy of Minor Analgesics in Primary Dysmenorrhoea: Systematic ReviewDocument10 pagesEfficacy of Minor Analgesics in Primary Dysmenorrhoea: Systematic Reviewadi saputraNo ratings yet
- Sugammadex Associated Anaphylaxis Summary And.777Document5 pagesSugammadex Associated Anaphylaxis Summary And.777Gabriela TeránNo ratings yet
- JCCM 06 089Document2 pagesJCCM 06 089filianalefaanNo ratings yet
- TCRM 7 459 PDFDocument13 pagesTCRM 7 459 PDFMikhael JHNo ratings yet
- Farmacos Antiepileptico Durante El EmbarazoDocument10 pagesFarmacos Antiepileptico Durante El EmbarazoAdán TreminioNo ratings yet
- Drug Hypersensitivity: Pharmacogenetics and Clinical SyndromesDocument7 pagesDrug Hypersensitivity: Pharmacogenetics and Clinical SyndromesdentsavvyNo ratings yet
- Updates in Refractory Epilepticus 2018Document11 pagesUpdates in Refractory Epilepticus 2018Syareevah Fachria ZahraNo ratings yet
- Effectiveness and Adverse Drug Reactions of Levetiracetam and Midazolam in Refractory Neonatal Seizure: A Cross Sectional Comparative StudyDocument6 pagesEffectiveness and Adverse Drug Reactions of Levetiracetam and Midazolam in Refractory Neonatal Seizure: A Cross Sectional Comparative StudySultan Rahmat SeptianNo ratings yet
- Best Vasopressor For Advanced Vasodilatory Shock Should Vasopressin Be Part of The MixDocument4 pagesBest Vasopressor For Advanced Vasodilatory Shock Should Vasopressin Be Part of The MixSurachai PraimaiNo ratings yet
- Recognition of Gout in RADocument4 pagesRecognition of Gout in RAsaphena parvaNo ratings yet
- Frontiers in Clinical Drug Research - CNS and Neurological Disorders: Volume 10From EverandFrontiers in Clinical Drug Research - CNS and Neurological Disorders: Volume 10No ratings yet
- KSB Surge PublicationDocument34 pagesKSB Surge PublicationDiego AguirreNo ratings yet
- Tata Sky ALC Channel ListDocument13 pagesTata Sky ALC Channel ListIndianMascot33% (3)
- Case Study: Distributed Scrum Project For Dutch RailwaysDocument7 pagesCase Study: Distributed Scrum Project For Dutch RailwaysDark LordNo ratings yet
- Stepless Drive-1Document3 pagesStepless Drive-1Mehul BawaNo ratings yet
- Class XII Phase Test I - SubDocument2 pagesClass XII Phase Test I - SubFariha KhanNo ratings yet
- The Importance of Segmentation in MarketingDocument8 pagesThe Importance of Segmentation in MarketingTPO SYSITSNo ratings yet
- Letters, Memoranda, Email, and Other Media For EngineersDocument5 pagesLetters, Memoranda, Email, and Other Media For EngineersOsama RashaydaNo ratings yet
- SDLC ModelDocument11 pagesSDLC Modeladititech724No ratings yet
- Code of Practice For Foundations 2017Document7 pagesCode of Practice For Foundations 2017Louis BrightonNo ratings yet
- Tipnis v. Emery Telephone Et Al - Document No. 3Document4 pagesTipnis v. Emery Telephone Et Al - Document No. 3Justia.comNo ratings yet
- Setting Up An Inventory Valuation Report in Dynamics AX Part 1 & 2Document18 pagesSetting Up An Inventory Valuation Report in Dynamics AX Part 1 & 2Fathy TahaNo ratings yet
- Facts About Tropical Rainforest EcosystemsDocument6 pagesFacts About Tropical Rainforest EcosystemsingridNo ratings yet
- EM2U70HLP 115-127 V 60 HZ 1Document4 pagesEM2U70HLP 115-127 V 60 HZ 1Carlos MouraNo ratings yet
- Mepl CPCLCBR Eil Qap&ds 001 2022 2023Document7 pagesMepl CPCLCBR Eil Qap&ds 001 2022 2023Mathi Vinoth PillaiNo ratings yet
- Be Computer Engineering Semester 4 2019 May Analysis of Algorithms CbcgsDocument19 pagesBe Computer Engineering Semester 4 2019 May Analysis of Algorithms CbcgsMysterious Mr.MisterNo ratings yet
- Acquisition of Property in The Philippines: Problems, Issues and Possible SolutionsDocument23 pagesAcquisition of Property in The Philippines: Problems, Issues and Possible SolutionsRonald AgustinNo ratings yet
- Informatica Mapping ScenariosDocument81 pagesInformatica Mapping ScenariosSri Kanth SriNo ratings yet
- MM30 743Document4 pagesMM30 743sigmasurat100% (1)
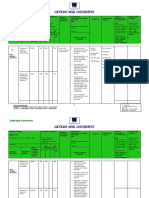
- Risk Assessment Hot WorkDocument5 pagesRisk Assessment Hot WorkRanjit DasNo ratings yet
- Comparison Chart: (Conduction, Convection, Radiation)Document5 pagesComparison Chart: (Conduction, Convection, Radiation)RandyNo ratings yet
- Jacked in 3 PDFDocument3 pagesJacked in 3 PDFPrïč ÎtčhNo ratings yet
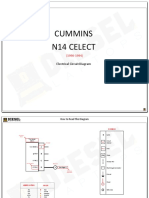
- Cummins N14 Celect: Electrical Circuit DiagramDocument9 pagesCummins N14 Celect: Electrical Circuit DiagramDiego Lira100% (1)
- Building SSR 2012-13Document411 pagesBuilding SSR 2012-13Nagabhushanam PayapalleNo ratings yet
- Law On SalesDocument45 pagesLaw On SalesRaiel B. Buenviaje RN100% (1)
- Revise Chap 12Document14 pagesRevise Chap 12RACHEL DAMALERIONo ratings yet
- Obdprog mt401 Pro Mileage Correction ToolDocument6 pagesObdprog mt401 Pro Mileage Correction ToolYounes YounesNo ratings yet
- BigData Avro-1Document30 pagesBigData Avro-1Sanjeeta ChauhanNo ratings yet
- The Declaration of IndependenceDocument20 pagesThe Declaration of IndependenceEdisonSambiliNo ratings yet