
Ssi-Post-Op-Form Word
Ssi-Post-Op-Form Word
You might also like
- Acute Kidney InjuryDocument3 pagesAcute Kidney InjuryPete Cobra Cobraiti100% (3)
- ESR Verification FormDocument2 pagesESR Verification Formlance tabinas83% (6)
- Microsoft PowerPoint - SSIDocument59 pagesMicrosoft PowerPoint - SSIRatna EkawatiNo ratings yet
- Panduan Praktek Klinis (PPK)Document12 pagesPanduan Praktek Klinis (PPK)anggawisnuNo ratings yet
- Ultrasound and clinically guided Injection techniques on the musculoskeletal systemFrom EverandUltrasound and clinically guided Injection techniques on the musculoskeletal systemNo ratings yet
- Surgical PearlsDocument8 pagesSurgical PearlsJohn Christopher LucesNo ratings yet
- Presentation SSIDocument41 pagesPresentation SSIJawad Mustafa100% (1)
- Introduction To General Pathology: DVM, M SC, DacvpDocument7 pagesIntroduction To General Pathology: DVM, M SC, DacvpCatenaNo ratings yet
- Vet. Clinical Diagnosis 2008Document19 pagesVet. Clinical Diagnosis 2008AbdusaburNo ratings yet
- Surgical Site Infection (SSI) : Event DetailsDocument4 pagesSurgical Site Infection (SSI) : Event DetailsLhaineVennetNo ratings yet
- Asuhan Keperawatan Di Instalasi Gawat DaruratDocument5 pagesAsuhan Keperawatan Di Instalasi Gawat DaruratLatifah khusnul SugiartoNo ratings yet
- Asuhan Keperawatan Di Instalasi Gawat DaruratDocument5 pagesAsuhan Keperawatan Di Instalasi Gawat DaruratAnnaNo ratings yet
- Asuhan Keperawatan Di Instalasi Gawat DaruratDocument5 pagesAsuhan Keperawatan Di Instalasi Gawat DaruratRidha TiomantaNo ratings yet
- Asuhan Keperawatan Di Instalasi Gawat DaruratDocument5 pagesAsuhan Keperawatan Di Instalasi Gawat DaruratDyah PerwaNo ratings yet
- Asuhan Keperawatan Di Instalasi Gawat DaruratDocument5 pagesAsuhan Keperawatan Di Instalasi Gawat DaruratrisaNo ratings yet
- Aefi CifDocument4 pagesAefi CifVic KwanNo ratings yet
- AEFI CIF-ao2013sept10 PDFDocument4 pagesAEFI CIF-ao2013sept10 PDFCHICKYNo ratings yet
- Aefi CifDocument6 pagesAefi CifVic KwanNo ratings yet
- 5.surgical Infections LectureDocument56 pages5.surgical Infections LectureBiruk DesalegnNo ratings yet
- 7 Des - Revisi - BPKM KGD S1 Kep 2023 - NEW-22-23Document2 pages7 Des - Revisi - BPKM KGD S1 Kep 2023 - NEW-22-23Nurul IzzaNo ratings yet
- CSI 201 Skills Lab - 2 - Lumbar - Puncture - Update - 5 - 25 - 2021Document13 pagesCSI 201 Skills Lab - 2 - Lumbar - Puncture - Update - 5 - 25 - 2021Bhupesh KumarNo ratings yet
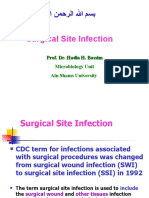
- Surgical Site Infection: Prof. Dr. Hadia H. Bassim Microbiology Unit Ain Shams UniversityDocument98 pagesSurgical Site Infection: Prof. Dr. Hadia H. Bassim Microbiology Unit Ain Shams UniversityHosam GomaaNo ratings yet
- Katelynn Owens - 1.2.1 Autopsy Report GuideDocument3 pagesKatelynn Owens - 1.2.1 Autopsy Report GuideKATELYNN OWENSNo ratings yet
- Surgical Site Infections: Negine Paul Assistant Professor Dept. of General and Upper GI Surgery 17.9.2019Document20 pagesSurgical Site Infections: Negine Paul Assistant Professor Dept. of General and Upper GI Surgery 17.9.2019Akhilesh BabuNo ratings yet
- Communicable DiseaseDocument98 pagesCommunicable DiseasePeach BubbleNo ratings yet
- Surgical Case Presentation SchemeDocument4 pagesSurgical Case Presentation SchemeVasilescu LauraNo ratings yet
- Aefi Cif 2014 Seriuos CaseDocument4 pagesAefi Cif 2014 Seriuos CaseJoanna Michelle VidasNo ratings yet
- Medical ExaminationDocument7 pagesMedical ExaminationSergey PoluboyarinovNo ratings yet
- Mr. H, 41YO, Multiple Vulnus Apertum, Dr. Saktrio D. Subarno, SP - BP-REDocument23 pagesMr. H, 41YO, Multiple Vulnus Apertum, Dr. Saktrio D. Subarno, SP - BP-REMusayada Dawua Part IINo ratings yet
- Primary Bloodstream Infection (BSI) : Risk FactorsDocument4 pagesPrimary Bloodstream Infection (BSI) : Risk Factorsdewi septianingrumNo ratings yet
- Definition SSIDocument2 pagesDefinition SSIAgungNo ratings yet
- Surgical Site Infections SSIDocument8 pagesSurgical Site Infections SSIkavimd21No ratings yet
- The Use of Cone Beam CT (CBCT) in Di of True From Mimicking Eagle's SyndromeDocument10 pagesThe Use of Cone Beam CT (CBCT) in Di of True From Mimicking Eagle's Syndromeleeperlhan2000No ratings yet
- General PathologyDocument50 pagesGeneral PathologyAhd BelalNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2)Divin MatthewNo ratings yet
- Introduction To General Pathology VPM 152: Web ReviewDocument41 pagesIntroduction To General Pathology VPM 152: Web ReviewRenien Khim BahayaNo ratings yet
- ESR Verification Form - Revise-Dina JoyDocument3 pagesESR Verification Form - Revise-Dina Joymawab.rhuNo ratings yet
- Mbbs Cbme Phase III Part IDocument1 pageMbbs Cbme Phase III Part IIlangovan RNo ratings yet
- Uid 1776Document12 pagesUid 1776IsaacJ22No ratings yet
- Sosialissi KPRS 2017Document20 pagesSosialissi KPRS 2017riaNo ratings yet
- Surgical Site InfectionsDocument78 pagesSurgical Site InfectionsBashiru AminuNo ratings yet
- Ent FinalsDocument40 pagesEnt Finalstwgp6pg5ghNo ratings yet
- How To Evaluate A Case of LeprosyDocument35 pagesHow To Evaluate A Case of LeprosyBarath Kumar SinghNo ratings yet
- SSI ProtocolDocument13 pagesSSI Protocolgechworkneh38No ratings yet
- Segmento 004 de 1466556889Document37 pagesSegmento 004 de 1466556889denis alvarezNo ratings yet
- Pi Is 0015028214002982Document10 pagesPi Is 0015028214002982Gomedi WuNo ratings yet
- Basic SurgeryDocument52 pagesBasic SurgeryMusabbirNo ratings yet
- Nosocomial InfectionsDocument12 pagesNosocomial InfectionsPehovelo JohannesNo ratings yet
- Shekhawati Form - FDocument2 pagesShekhawati Form - FArchit Champanekar100% (1)
- Dr. Rasul Dr. Orencia: Surgery ER Orthopedics Ward OR ENT OPD Ophthalmology ClerkDocument12 pagesDr. Rasul Dr. Orencia: Surgery ER Orthopedics Ward OR ENT OPD Ophthalmology ClerkApmc Schwartz100% (1)
- 021wound Infection 2018Document110 pages021wound Infection 2018Sam TitusNo ratings yet
- The EMERGENCY SEVERITY INDEXDocument6 pagesThe EMERGENCY SEVERITY INDEXWindyNo ratings yet
- Management of Open Fractures Prof A Sárváry Septic and Non Septic Complications in Traumatology Fractures of The Tibia and FibulaDocument52 pagesManagement of Open Fractures Prof A Sárváry Septic and Non Septic Complications in Traumatology Fractures of The Tibia and FibulaHurulaeniNo ratings yet
- New 1Document23 pagesNew 1api-3701377No ratings yet
- SURGICAL SITE INFECTIONS (By Naveed)Document39 pagesSURGICAL SITE INFECTIONS (By Naveed)Mahar NaveedNo ratings yet
- SSTi Diabetic PETRI 2019Document36 pagesSSTi Diabetic PETRI 2019intermoska soloNo ratings yet
- Format Askep KGD KritisDocument14 pagesFormat Askep KGD KritisRirin Alfiah RiantiNo ratings yet
- Nosocomial Infection and Surgical Site InfectionDocument48 pagesNosocomial Infection and Surgical Site InfectionFranz BalponNo ratings yet
- Tumors by SadekDocument22 pagesTumors by SadekAhmed El SayedNo ratings yet
- Little Known Facts About Infectious Diseases/ Imaging On CrossroadsFrom EverandLittle Known Facts About Infectious Diseases/ Imaging On CrossroadsNo ratings yet
- Hemiplegia LectureDocument37 pagesHemiplegia LectureRancesh FamoNo ratings yet
- Checklist For Administering Oxygen by Nasal CannulaDocument3 pagesChecklist For Administering Oxygen by Nasal CannulaNasrah TalusobNo ratings yet
- 34 Journal of Periodontology - 2018 - H Mmerle - The Etiology of Hard and Soft Tissue Deficiencies at Dental Implants ADocument13 pages34 Journal of Periodontology - 2018 - H Mmerle - The Etiology of Hard and Soft Tissue Deficiencies at Dental Implants AMax Flores RuizNo ratings yet
- Post-Operative Instructions: Laparoscopic CholecystectomyDocument2 pagesPost-Operative Instructions: Laparoscopic Cholecystectomyrizwan234No ratings yet
- Injury Patterns in Danish Competitive SwimmingDocument5 pagesInjury Patterns in Danish Competitive SwimmingSebastian VicolNo ratings yet
- Biological Forms of Tooth Preparation (Lecture by DR - Wedad Etman @AmCoFam)Document15 pagesBiological Forms of Tooth Preparation (Lecture by DR - Wedad Etman @AmCoFam)AmericanCornerFamilyNo ratings yet
- Table of Comparison On Cardiopulmonary Resuscitation For Adul1Document1 pageTable of Comparison On Cardiopulmonary Resuscitation For Adul1Luigi GeduqueNo ratings yet
- Clinically Diagnosed Postoperative Venous Thromboembolism in A NeurosurgeryDocument7 pagesClinically Diagnosed Postoperative Venous Thromboembolism in A Neurosurgerydonira73No ratings yet
- ... Rapid Complete Recovery From An Autism Spectrum Disorder After Treatment... With... Antifungal Drugs ...Document8 pages... Rapid Complete Recovery From An Autism Spectrum Disorder After Treatment... With... Antifungal Drugs ...Daniel GilbertoNo ratings yet
- Hans Selye. The General Adaptation SyndromeDocument16 pagesHans Selye. The General Adaptation SyndromeCelso Sánchez Ramírez100% (2)
- Allergy Blood Test (IgE)Document5 pagesAllergy Blood Test (IgE)Muhammad RaheemNo ratings yet
- Ga F 2012 AbstractDocument326 pagesGa F 2012 AbstractAkash Agarwal100% (1)
- Written - Notes General Survey Vitals Pain 2Document1 pageWritten - Notes General Survey Vitals Pain 2Sheryl LaffertyNo ratings yet
- Case StudyDocument1 pageCase StudyGemina Leah MaeNo ratings yet
- Disease-Wise Suggested Homeopathic RemediesDocument8 pagesDisease-Wise Suggested Homeopathic RemediesNikunjNo ratings yet
- NP1Document14 pagesNP1rexinne noahNo ratings yet
- Review & Revision Schedule Hyderabad - CerebellumDocument1 pageReview & Revision Schedule Hyderabad - CerebellumCrassy RajeshNo ratings yet
- List of Rapid Antigen Kits 11052021Document13 pagesList of Rapid Antigen Kits 11052021Subhankar SahaNo ratings yet
- Moderate and Extreme HypofractionationDocument32 pagesModerate and Extreme HypofractionationsamuelfsjNo ratings yet
- Knockout Paralysis FlyerDocument1 pageKnockout Paralysis FlyerJessika KattahNo ratings yet
- Patient Satisfaction Following Orthognathic Surgical Correction of Skeletal Class III MalocclusionDocument9 pagesPatient Satisfaction Following Orthognathic Surgical Correction of Skeletal Class III MalocclusionAbles227 BlessNo ratings yet
- EdCaN Specialty Module 4Document23 pagesEdCaN Specialty Module 4cindy8127No ratings yet
- Karnofsky Performance Status Scale - Karnofsky Performance Status ScaleDocument2 pagesKarnofsky Performance Status Scale - Karnofsky Performance Status ScaleNungkiNo ratings yet
- ASGE 2012 Endoscopy in Pregnant and Lactating WomenDocument7 pagesASGE 2012 Endoscopy in Pregnant and Lactating WomenjordanNo ratings yet
- Author: Heidi Hanes: Aaasedre Asds ReviesionDocument14 pagesAuthor: Heidi Hanes: Aaasedre Asds ReviesionmmNo ratings yet
- Royal Bournemouth Hospital Site Plan: A338 Wessex Wa yDocument1 pageRoyal Bournemouth Hospital Site Plan: A338 Wessex Wa ydolar buhaNo ratings yet
- Update On Stemi Management: Dr. Adi Purnawarman, SP - JP (K) - Fiha.,FasccDocument39 pagesUpdate On Stemi Management: Dr. Adi Purnawarman, SP - JP (K) - Fiha.,FasccArfiska Ridha Fausa 'ucha'No ratings yet
- Outcome 2016 (Khoá gây tê vùng dưới hướng dẫn siêu âm ĐHYHN)Document40 pagesOutcome 2016 (Khoá gây tê vùng dưới hướng dẫn siêu âm ĐHYHN)Rùa’s Anesthesia HanoiNo ratings yet
- In-Vitro FertilizationDocument48 pagesIn-Vitro FertilizationRenz L. Salumbre100% (2)
























































































Download as docx, pdf, or txt
You might also like
- Acute Kidney InjuryDocument3 pagesAcute Kidney InjuryPete Cobra Cobraiti100% (3)
- ESR Verification FormDocument2 pagesESR Verification Formlance tabinas83% (6)
- Microsoft PowerPoint - SSIDocument59 pagesMicrosoft PowerPoint - SSIRatna EkawatiNo ratings yet
- Panduan Praktek Klinis (PPK)Document12 pagesPanduan Praktek Klinis (PPK)anggawisnuNo ratings yet
- Ultrasound and clinically guided Injection techniques on the musculoskeletal systemFrom EverandUltrasound and clinically guided Injection techniques on the musculoskeletal systemNo ratings yet
- Surgical PearlsDocument8 pagesSurgical PearlsJohn Christopher LucesNo ratings yet
- Presentation SSIDocument41 pagesPresentation SSIJawad Mustafa100% (1)
- Introduction To General Pathology: DVM, M SC, DacvpDocument7 pagesIntroduction To General Pathology: DVM, M SC, DacvpCatenaNo ratings yet
- Vet. Clinical Diagnosis 2008Document19 pagesVet. Clinical Diagnosis 2008AbdusaburNo ratings yet
- Surgical Site Infection (SSI) : Event DetailsDocument4 pagesSurgical Site Infection (SSI) : Event DetailsLhaineVennetNo ratings yet
- Asuhan Keperawatan Di Instalasi Gawat DaruratDocument5 pagesAsuhan Keperawatan Di Instalasi Gawat DaruratLatifah khusnul SugiartoNo ratings yet
- Asuhan Keperawatan Di Instalasi Gawat DaruratDocument5 pagesAsuhan Keperawatan Di Instalasi Gawat DaruratAnnaNo ratings yet
- Asuhan Keperawatan Di Instalasi Gawat DaruratDocument5 pagesAsuhan Keperawatan Di Instalasi Gawat DaruratRidha TiomantaNo ratings yet
- Asuhan Keperawatan Di Instalasi Gawat DaruratDocument5 pagesAsuhan Keperawatan Di Instalasi Gawat DaruratDyah PerwaNo ratings yet
- Asuhan Keperawatan Di Instalasi Gawat DaruratDocument5 pagesAsuhan Keperawatan Di Instalasi Gawat DaruratrisaNo ratings yet
- Aefi CifDocument4 pagesAefi CifVic KwanNo ratings yet
- AEFI CIF-ao2013sept10 PDFDocument4 pagesAEFI CIF-ao2013sept10 PDFCHICKYNo ratings yet
- Aefi CifDocument6 pagesAefi CifVic KwanNo ratings yet
- 5.surgical Infections LectureDocument56 pages5.surgical Infections LectureBiruk DesalegnNo ratings yet
- 7 Des - Revisi - BPKM KGD S1 Kep 2023 - NEW-22-23Document2 pages7 Des - Revisi - BPKM KGD S1 Kep 2023 - NEW-22-23Nurul IzzaNo ratings yet
- CSI 201 Skills Lab - 2 - Lumbar - Puncture - Update - 5 - 25 - 2021Document13 pagesCSI 201 Skills Lab - 2 - Lumbar - Puncture - Update - 5 - 25 - 2021Bhupesh KumarNo ratings yet
- Surgical Site Infection: Prof. Dr. Hadia H. Bassim Microbiology Unit Ain Shams UniversityDocument98 pagesSurgical Site Infection: Prof. Dr. Hadia H. Bassim Microbiology Unit Ain Shams UniversityHosam GomaaNo ratings yet
- Katelynn Owens - 1.2.1 Autopsy Report GuideDocument3 pagesKatelynn Owens - 1.2.1 Autopsy Report GuideKATELYNN OWENSNo ratings yet
- Surgical Site Infections: Negine Paul Assistant Professor Dept. of General and Upper GI Surgery 17.9.2019Document20 pagesSurgical Site Infections: Negine Paul Assistant Professor Dept. of General and Upper GI Surgery 17.9.2019Akhilesh BabuNo ratings yet
- Communicable DiseaseDocument98 pagesCommunicable DiseasePeach BubbleNo ratings yet
- Surgical Case Presentation SchemeDocument4 pagesSurgical Case Presentation SchemeVasilescu LauraNo ratings yet
- Aefi Cif 2014 Seriuos CaseDocument4 pagesAefi Cif 2014 Seriuos CaseJoanna Michelle VidasNo ratings yet
- Medical ExaminationDocument7 pagesMedical ExaminationSergey PoluboyarinovNo ratings yet
- Mr. H, 41YO, Multiple Vulnus Apertum, Dr. Saktrio D. Subarno, SP - BP-REDocument23 pagesMr. H, 41YO, Multiple Vulnus Apertum, Dr. Saktrio D. Subarno, SP - BP-REMusayada Dawua Part IINo ratings yet
- Primary Bloodstream Infection (BSI) : Risk FactorsDocument4 pagesPrimary Bloodstream Infection (BSI) : Risk Factorsdewi septianingrumNo ratings yet
- Definition SSIDocument2 pagesDefinition SSIAgungNo ratings yet
- Surgical Site Infections SSIDocument8 pagesSurgical Site Infections SSIkavimd21No ratings yet
- The Use of Cone Beam CT (CBCT) in Di of True From Mimicking Eagle's SyndromeDocument10 pagesThe Use of Cone Beam CT (CBCT) in Di of True From Mimicking Eagle's Syndromeleeperlhan2000No ratings yet
- General PathologyDocument50 pagesGeneral PathologyAhd BelalNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2)Divin MatthewNo ratings yet
- Introduction To General Pathology VPM 152: Web ReviewDocument41 pagesIntroduction To General Pathology VPM 152: Web ReviewRenien Khim BahayaNo ratings yet
- ESR Verification Form - Revise-Dina JoyDocument3 pagesESR Verification Form - Revise-Dina Joymawab.rhuNo ratings yet
- Mbbs Cbme Phase III Part IDocument1 pageMbbs Cbme Phase III Part IIlangovan RNo ratings yet
- Uid 1776Document12 pagesUid 1776IsaacJ22No ratings yet
- Sosialissi KPRS 2017Document20 pagesSosialissi KPRS 2017riaNo ratings yet
- Surgical Site InfectionsDocument78 pagesSurgical Site InfectionsBashiru AminuNo ratings yet
- Ent FinalsDocument40 pagesEnt Finalstwgp6pg5ghNo ratings yet
- How To Evaluate A Case of LeprosyDocument35 pagesHow To Evaluate A Case of LeprosyBarath Kumar SinghNo ratings yet
- SSI ProtocolDocument13 pagesSSI Protocolgechworkneh38No ratings yet
- Segmento 004 de 1466556889Document37 pagesSegmento 004 de 1466556889denis alvarezNo ratings yet
- Pi Is 0015028214002982Document10 pagesPi Is 0015028214002982Gomedi WuNo ratings yet
- Basic SurgeryDocument52 pagesBasic SurgeryMusabbirNo ratings yet
- Nosocomial InfectionsDocument12 pagesNosocomial InfectionsPehovelo JohannesNo ratings yet
- Shekhawati Form - FDocument2 pagesShekhawati Form - FArchit Champanekar100% (1)
- Dr. Rasul Dr. Orencia: Surgery ER Orthopedics Ward OR ENT OPD Ophthalmology ClerkDocument12 pagesDr. Rasul Dr. Orencia: Surgery ER Orthopedics Ward OR ENT OPD Ophthalmology ClerkApmc Schwartz100% (1)
- 021wound Infection 2018Document110 pages021wound Infection 2018Sam TitusNo ratings yet
- The EMERGENCY SEVERITY INDEXDocument6 pagesThe EMERGENCY SEVERITY INDEXWindyNo ratings yet
- Management of Open Fractures Prof A Sárváry Septic and Non Septic Complications in Traumatology Fractures of The Tibia and FibulaDocument52 pagesManagement of Open Fractures Prof A Sárváry Septic and Non Septic Complications in Traumatology Fractures of The Tibia and FibulaHurulaeniNo ratings yet
- New 1Document23 pagesNew 1api-3701377No ratings yet
- SURGICAL SITE INFECTIONS (By Naveed)Document39 pagesSURGICAL SITE INFECTIONS (By Naveed)Mahar NaveedNo ratings yet
- SSTi Diabetic PETRI 2019Document36 pagesSSTi Diabetic PETRI 2019intermoska soloNo ratings yet
- Format Askep KGD KritisDocument14 pagesFormat Askep KGD KritisRirin Alfiah RiantiNo ratings yet
- Nosocomial Infection and Surgical Site InfectionDocument48 pagesNosocomial Infection and Surgical Site InfectionFranz BalponNo ratings yet
- Tumors by SadekDocument22 pagesTumors by SadekAhmed El SayedNo ratings yet
- Little Known Facts About Infectious Diseases/ Imaging On CrossroadsFrom EverandLittle Known Facts About Infectious Diseases/ Imaging On CrossroadsNo ratings yet
- Hemiplegia LectureDocument37 pagesHemiplegia LectureRancesh FamoNo ratings yet
- Checklist For Administering Oxygen by Nasal CannulaDocument3 pagesChecklist For Administering Oxygen by Nasal CannulaNasrah TalusobNo ratings yet
- 34 Journal of Periodontology - 2018 - H Mmerle - The Etiology of Hard and Soft Tissue Deficiencies at Dental Implants ADocument13 pages34 Journal of Periodontology - 2018 - H Mmerle - The Etiology of Hard and Soft Tissue Deficiencies at Dental Implants AMax Flores RuizNo ratings yet
- Post-Operative Instructions: Laparoscopic CholecystectomyDocument2 pagesPost-Operative Instructions: Laparoscopic Cholecystectomyrizwan234No ratings yet
- Injury Patterns in Danish Competitive SwimmingDocument5 pagesInjury Patterns in Danish Competitive SwimmingSebastian VicolNo ratings yet
- Biological Forms of Tooth Preparation (Lecture by DR - Wedad Etman @AmCoFam)Document15 pagesBiological Forms of Tooth Preparation (Lecture by DR - Wedad Etman @AmCoFam)AmericanCornerFamilyNo ratings yet
- Table of Comparison On Cardiopulmonary Resuscitation For Adul1Document1 pageTable of Comparison On Cardiopulmonary Resuscitation For Adul1Luigi GeduqueNo ratings yet
- Clinically Diagnosed Postoperative Venous Thromboembolism in A NeurosurgeryDocument7 pagesClinically Diagnosed Postoperative Venous Thromboembolism in A Neurosurgerydonira73No ratings yet
- ... Rapid Complete Recovery From An Autism Spectrum Disorder After Treatment... With... Antifungal Drugs ...Document8 pages... Rapid Complete Recovery From An Autism Spectrum Disorder After Treatment... With... Antifungal Drugs ...Daniel GilbertoNo ratings yet
- Hans Selye. The General Adaptation SyndromeDocument16 pagesHans Selye. The General Adaptation SyndromeCelso Sánchez Ramírez100% (2)
- Allergy Blood Test (IgE)Document5 pagesAllergy Blood Test (IgE)Muhammad RaheemNo ratings yet
- Ga F 2012 AbstractDocument326 pagesGa F 2012 AbstractAkash Agarwal100% (1)
- Written - Notes General Survey Vitals Pain 2Document1 pageWritten - Notes General Survey Vitals Pain 2Sheryl LaffertyNo ratings yet
- Case StudyDocument1 pageCase StudyGemina Leah MaeNo ratings yet
- Disease-Wise Suggested Homeopathic RemediesDocument8 pagesDisease-Wise Suggested Homeopathic RemediesNikunjNo ratings yet
- NP1Document14 pagesNP1rexinne noahNo ratings yet
- Review & Revision Schedule Hyderabad - CerebellumDocument1 pageReview & Revision Schedule Hyderabad - CerebellumCrassy RajeshNo ratings yet
- List of Rapid Antigen Kits 11052021Document13 pagesList of Rapid Antigen Kits 11052021Subhankar SahaNo ratings yet
- Moderate and Extreme HypofractionationDocument32 pagesModerate and Extreme HypofractionationsamuelfsjNo ratings yet
- Knockout Paralysis FlyerDocument1 pageKnockout Paralysis FlyerJessika KattahNo ratings yet
- Patient Satisfaction Following Orthognathic Surgical Correction of Skeletal Class III MalocclusionDocument9 pagesPatient Satisfaction Following Orthognathic Surgical Correction of Skeletal Class III MalocclusionAbles227 BlessNo ratings yet
- EdCaN Specialty Module 4Document23 pagesEdCaN Specialty Module 4cindy8127No ratings yet
- Karnofsky Performance Status Scale - Karnofsky Performance Status ScaleDocument2 pagesKarnofsky Performance Status Scale - Karnofsky Performance Status ScaleNungkiNo ratings yet
- ASGE 2012 Endoscopy in Pregnant and Lactating WomenDocument7 pagesASGE 2012 Endoscopy in Pregnant and Lactating WomenjordanNo ratings yet
- Author: Heidi Hanes: Aaasedre Asds ReviesionDocument14 pagesAuthor: Heidi Hanes: Aaasedre Asds ReviesionmmNo ratings yet
- Royal Bournemouth Hospital Site Plan: A338 Wessex Wa yDocument1 pageRoyal Bournemouth Hospital Site Plan: A338 Wessex Wa ydolar buhaNo ratings yet
- Update On Stemi Management: Dr. Adi Purnawarman, SP - JP (K) - Fiha.,FasccDocument39 pagesUpdate On Stemi Management: Dr. Adi Purnawarman, SP - JP (K) - Fiha.,FasccArfiska Ridha Fausa 'ucha'No ratings yet
- Outcome 2016 (Khoá gây tê vùng dưới hướng dẫn siêu âm ĐHYHN)Document40 pagesOutcome 2016 (Khoá gây tê vùng dưới hướng dẫn siêu âm ĐHYHN)Rùa’s Anesthesia HanoiNo ratings yet
- In-Vitro FertilizationDocument48 pagesIn-Vitro FertilizationRenz L. Salumbre100% (2)