
BREATHE Diagnosis and Management PAH
BREATHE Diagnosis and Management PAH
You might also like
- Diagnosis and Treatment of Pulmonary Arterial Hypertension A ReviewDocument13 pagesDiagnosis and Treatment of Pulmonary Arterial Hypertension A ReviewLuis Enrique Giraldo PenicheNo ratings yet
- Update Dec 06Document18 pagesUpdate Dec 06api-27370939No ratings yet
- Metabolic Dysfunction in Pulmonary Hypertension FR PDFDocument11 pagesMetabolic Dysfunction in Pulmonary Hypertension FR PDFWayan GunawanNo ratings yet
- 449 FullDocument6 pages449 Fullwael aboelmagdNo ratings yet
- RCCM 202012-4317soDocument16 pagesRCCM 202012-4317soRhahahaNo ratings yet
- Pulmonary HypertensionDocument25 pagesPulmonary Hypertensionavinashvyas2007No ratings yet
- Jim 2020 001291.fullDocument7 pagesJim 2020 001291.fullAlessioNavarraNo ratings yet
- New Progress in Diagnosis and Treatment of Pulmonary Arterial HypertensionDocument9 pagesNew Progress in Diagnosis and Treatment of Pulmonary Arterial HypertensionRhahahaNo ratings yet
- Pulmonary Hipertension PDFDocument481 pagesPulmonary Hipertension PDFRadhiatul AdillahNo ratings yet
- Diagnosis of Pulmonary HypertensionDocument12 pagesDiagnosis of Pulmonary HypertensionFaridaFaradillaPutryCherewetNo ratings yet
- Pulmonary HipertensionDocument481 pagesPulmonary HipertensionFransiskus A Danu KrisbiantoroNo ratings yet
- WSPH 2019Document15 pagesWSPH 2019Faisol SiddiqNo ratings yet
- Jama 2022 327 1379Document13 pagesJama 2022 327 1379silviaNo ratings yet
- Revised Definition of Pulmonary Hypertension and Approach To Management: A Clinical PrimerDocument8 pagesRevised Definition of Pulmonary Hypertension and Approach To Management: A Clinical PrimerRhahahaNo ratings yet
- Vias Moleculares HapDocument24 pagesVias Moleculares Hapdayanachuquimia95No ratings yet
- Pharmaceuticals 15 01242Document29 pagesPharmaceuticals 15 01242gadangNo ratings yet
- Clinical Update On Pulmonary Hypertension: Salim Yaghi, Anastasia Novikov, Theo TrandafirescuDocument7 pagesClinical Update On Pulmonary Hypertension: Salim Yaghi, Anastasia Novikov, Theo TrandafirescuIs DGNo ratings yet
- 肺动脉高压诊治临床路径Document13 pages肺动脉高压诊治临床路径zjjszflNo ratings yet
- JR Hipertensi Pulmonal Rizki AmaliyahDocument11 pagesJR Hipertensi Pulmonal Rizki AmaliyahnengahdarmawanNo ratings yet
- Maron 2023 Revised Definition of Pulmonary Hypertension and Approach To Management A Clinical PrimerDocument8 pagesMaron 2023 Revised Definition of Pulmonary Hypertension and Approach To Management A Clinical PrimerDaniel ForeroNo ratings yet
- Guideline USA 2020Document16 pagesGuideline USA 2020Rodrigo Felipe Albuquerque Paiva de OliveiraNo ratings yet
- Circulationaha 114 006971Document11 pagesCirculationaha 114 006971RhahahaNo ratings yet
- Pulmonary Arterial Hypertension: The Burden of Disease and Impact On Quality of LifeDocument9 pagesPulmonary Arterial Hypertension: The Burden of Disease and Impact On Quality of LifeMeilani Azaria SNo ratings yet
- Ijms 24 08462Document4 pagesIjms 24 08462RhahahaNo ratings yet
- Err 0099 2020Document12 pagesErr 0099 2020Faradiba MaricarNo ratings yet
- Pulmon AlDocument1 pagePulmon AlBrisney AureliaNo ratings yet
- 1 s2.0 S1053077021005723 MainDocument13 pages1 s2.0 S1053077021005723 Main8mjy475v9mNo ratings yet
- Additional 3Document12 pagesAdditional 3Bagus Radityo AmienNo ratings yet
- Pulmonary HypertensionDocument8 pagesPulmonary HypertensionSebastian BarreraNo ratings yet
- Hipertensión PulmonarDocument13 pagesHipertensión PulmonarBrayam Emerson Calderón RecaldeNo ratings yet
- Approach To Pulmonary Hypertension From CT To Clinical DiagnosisDocument17 pagesApproach To Pulmonary Hypertension From CT To Clinical DiagnosisnancyNo ratings yet
- Epidemiology of Pulmonary HypertensionDocument19 pagesEpidemiology of Pulmonary HypertensionzulemerlanoNo ratings yet
- Jama Ruopp 2022 RV 220007 1662040577.72953Document13 pagesJama Ruopp 2022 RV 220007 1662040577.72953Yo MeNo ratings yet
- PAH Ann Intern Med 2013Document15 pagesPAH Ann Intern Med 2013waterprincess100% (1)
- Póster 1Document3 pagesPóster 1Dan Medina OrtizNo ratings yet
- Chest Julio 2022 Hipertension Pulm en ILDDocument11 pagesChest Julio 2022 Hipertension Pulm en ILDnoeliaNo ratings yet
- Updated 20 Classification 20 and 20 Management 20 of 20 Pulmonary 20 HypertensionDocument10 pagesUpdated 20 Classification 20 and 20 Management 20 of 20 Pulmonary 20 HypertensionAarlettejimenezNo ratings yet
- Pulmonary Veno-Occlusive Disease An Important Consideration in PatientsDocument7 pagesPulmonary Veno-Occlusive Disease An Important Consideration in PatientsأنيسNo ratings yet
- Hipertensi PulmonalDocument5 pagesHipertensi PulmonalSteven RichardNo ratings yet
- 1 s2.0 S0012369219300029 MainDocument22 pages1 s2.0 S0012369219300029 MainbrandusaNo ratings yet
- Hipertension Pulmonar Tto Lancet 2023Document16 pagesHipertension Pulmonar Tto Lancet 2023alejandro RodriguezNo ratings yet
- HTPAnnals 2005Document12 pagesHTPAnnals 2005api-3703544No ratings yet
- Tratment Oh HIV-PAHDocument34 pagesTratment Oh HIV-PAHFelisa Nur KhayanaNo ratings yet
- Recent Advances in Pulmonary HypertensionDocument12 pagesRecent Advances in Pulmonary Hypertensionflying highNo ratings yet
- Psychosocial Aspects of Pulmonary Hypertension: A Review: J M. W, P .D., G L, M.D. V M L, M.D., M R, M.D. M R, M.DDocument9 pagesPsychosocial Aspects of Pulmonary Hypertension: A Review: J M. W, P .D., G L, M.D. V M L, M.D., M R, M.D. M R, M.DNedelcuCMNo ratings yet
- Pulmonary HTN. ESC POCKET GLS 2022. Larger Font. For PrintingDocument79 pagesPulmonary HTN. ESC POCKET GLS 2022. Larger Font. For PrintingGeoNo ratings yet
- Prognostic Factors in Pulmonary Arterial Hypertension: Literature ReviewDocument5 pagesPrognostic Factors in Pulmonary Arterial Hypertension: Literature Reviewhuda riyambodoNo ratings yet
- South Africa A Global View of Pulmonary HypertensionDocument17 pagesSouth Africa A Global View of Pulmonary HypertensionDhan RamadhanNo ratings yet
- Hoeper 2016Document14 pagesHoeper 2016riyad saksakNo ratings yet
- Medicina: Pulmonary Hypertension in COPD: A Case Study and Review of The LiteratureDocument8 pagesMedicina: Pulmonary Hypertension in COPD: A Case Study and Review of The Literatureguhan taraNo ratings yet
- Modern Invasive Hemodynamic Assessment of Pulmonary HypertensionDocument11 pagesModern Invasive Hemodynamic Assessment of Pulmonary HypertensionfabiolaNo ratings yet
- British J Pharmacology - 2021 - DignamDocument27 pagesBritish J Pharmacology - 2021 - DignamLinda Silvana SariNo ratings yet
- HT PedDocument18 pagesHT PedLina María CañónNo ratings yet
- Pulmonary HypertensionDocument20 pagesPulmonary Hypertensionyelsinosmin romeroalvaradoNo ratings yet
- Hemodynamic Indices in Pulmonary Hypertension: A Narrative ReviewDocument15 pagesHemodynamic Indices in Pulmonary Hypertension: A Narrative ReviewfabiolaNo ratings yet
- Pulmonary Hypertension: Annals of Internal MedicinetDocument16 pagesPulmonary Hypertension: Annals of Internal MedicinetAlicia TGNo ratings yet
- 2022 PH Guidelines - Essential MessagesDocument10 pages2022 PH Guidelines - Essential MessagesRoyNo ratings yet
- Management Strategies For Patients With Pulmonary Hypertension in The Intensive Care UnitDocument14 pagesManagement Strategies For Patients With Pulmonary Hypertension in The Intensive Care Unitanon-374465No ratings yet
- Pulmonary Hypertension Mediastinal FibrosisDocument10 pagesPulmonary Hypertension Mediastinal FibrosisAndreiSefNo ratings yet
- PAH Lessons From A Cancer Final VersionDocument11 pagesPAH Lessons From A Cancer Final VersionAndreiSefNo ratings yet
- COPD: A Guide to Diagnosis and Clinical ManagementFrom EverandCOPD: A Guide to Diagnosis and Clinical ManagementNicola A. HananiaNo ratings yet
- Potential of Non-Conventional Source of Energy and Associated Environmental Issue: An Indian ScenarioDocument6 pagesPotential of Non-Conventional Source of Energy and Associated Environmental Issue: An Indian ScenarioSanchit PatilNo ratings yet
- A Review On Tecoma StansDocument3 pagesA Review On Tecoma StansBaru Chandrasekhar RaoNo ratings yet
- 5085DL / 5055DL SeriesDocument2 pages5085DL / 5055DL SeriesMinh TranNo ratings yet
- Cakes and IcingsDocument2 pagesCakes and Icingsgian jorgioNo ratings yet
- Summer Training Report On: "Consumer Perception Towards Online Shopping"Document83 pagesSummer Training Report On: "Consumer Perception Towards Online Shopping"Swati TanwarNo ratings yet
- Full Text 01Document113 pagesFull Text 01Anonymous GUitcVONo ratings yet
- Long-Term Effects Fertilizers Yield Soil Fertility Winter Wheat-Maize System in Jiangsu, China 'Document8 pagesLong-Term Effects Fertilizers Yield Soil Fertility Winter Wheat-Maize System in Jiangsu, China 'wisnuaji wibowoNo ratings yet
- Mark Scheme (Results) November 2009: IGCSE Biology (4325) Paper 2HDocument16 pagesMark Scheme (Results) November 2009: IGCSE Biology (4325) Paper 2HmuhajireenNo ratings yet
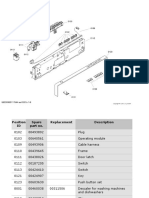
- ΕΓΧΕΙΡΙΔΙΟ ΠΛΥΝΤΗΡΙΟΥ ΠΙΑΤΩΝ - ΑΝΤΑΛΛΑΚΤΙΚΑDocument16 pagesΕΓΧΕΙΡΙΔΙΟ ΠΛΥΝΤΗΡΙΟΥ ΠΙΑΤΩΝ - ΑΝΤΑΛΛΑΚΤΙΚΑΤΣΙΜΠΙΔΗΣ ΠΑΝΑΓΙΩΤΗΣNo ratings yet
- Added Scenes For - Tattered FatesDocument19 pagesAdded Scenes For - Tattered FatesRadosław KwiecińskiNo ratings yet
- GRI 180-12-B-W1K Data SheetDocument3 pagesGRI 180-12-B-W1K Data SheetJMAC SupplyNo ratings yet
- One Dimensional Heat EquationDocument30 pagesOne Dimensional Heat Equation20-317 RithvikNo ratings yet
- Basic Summary of X-Ray Equipment - Naver BlogDocument7 pagesBasic Summary of X-Ray Equipment - Naver BlogMalikAlrahabiNo ratings yet
- GALLO-SCYTHIANS - Celtic Ukraine (By Mac Congail)Document22 pagesGALLO-SCYTHIANS - Celtic Ukraine (By Mac Congail)Toma100% (1)
- Therblig Color Symbol/Icon Therblig Color Symbol/Icon: Search Black Use PurpleDocument10 pagesTherblig Color Symbol/Icon Therblig Color Symbol/Icon: Search Black Use Purplechad macatangayNo ratings yet
- IUPAC & Nomenclature PDFDocument6 pagesIUPAC & Nomenclature PDFjaspreet singh100% (1)
- Gamesa G90 2mwDocument6 pagesGamesa G90 2mwNemanja KomatinovicNo ratings yet
- Kepco KpsDocument27 pagesKepco Kps허준No ratings yet
- Procedure For Equipment Calibration and MaintenanceDocument9 pagesProcedure For Equipment Calibration and MaintenanceAli HadiNo ratings yet
- Compilations of Board Exam Problem1 PDFDocument65 pagesCompilations of Board Exam Problem1 PDFJevan Calaque100% (1)
- Bonn & Gaston 2005 Richness Ecosystem Conserv SAfDocument18 pagesBonn & Gaston 2005 Richness Ecosystem Conserv SAfKellyta RodriguezNo ratings yet
- Datasheet VisiTouch-Pac V1.3 ENDocument8 pagesDatasheet VisiTouch-Pac V1.3 ENDavid CalderonNo ratings yet
- University of Cambridge International Examinations International General Certificate of Secondary EducationDocument20 pagesUniversity of Cambridge International Examinations International General Certificate of Secondary Educationluines78No ratings yet
- Worked Example To Eurocode 2 Vol 1Document228 pagesWorked Example To Eurocode 2 Vol 1Mohd RafiqNo ratings yet
- Planning and Designing of Bridge Over Solani RiverDocument5 pagesPlanning and Designing of Bridge Over Solani RiverCurious RajNo ratings yet
- Precision t7810 Workstation - Owners Manual - en UsDocument58 pagesPrecision t7810 Workstation - Owners Manual - en Usfotograf nuntaNo ratings yet
- Arsenic Presentation 11111Document19 pagesArsenic Presentation 11111Namrata PalNo ratings yet
- IHKS Summit ProgramDocument35 pagesIHKS Summit ProgramDiah Rahayu SetiawatiNo ratings yet
- PhET Simulation - Determination of Planck's ConstantDocument3 pagesPhET Simulation - Determination of Planck's ConstantDaniel CruzNo ratings yet
























































































Download as pdf or txt
You might also like
- Diagnosis and Treatment of Pulmonary Arterial Hypertension A ReviewDocument13 pagesDiagnosis and Treatment of Pulmonary Arterial Hypertension A ReviewLuis Enrique Giraldo PenicheNo ratings yet
- Update Dec 06Document18 pagesUpdate Dec 06api-27370939No ratings yet
- Metabolic Dysfunction in Pulmonary Hypertension FR PDFDocument11 pagesMetabolic Dysfunction in Pulmonary Hypertension FR PDFWayan GunawanNo ratings yet
- 449 FullDocument6 pages449 Fullwael aboelmagdNo ratings yet
- RCCM 202012-4317soDocument16 pagesRCCM 202012-4317soRhahahaNo ratings yet
- Pulmonary HypertensionDocument25 pagesPulmonary Hypertensionavinashvyas2007No ratings yet
- Jim 2020 001291.fullDocument7 pagesJim 2020 001291.fullAlessioNavarraNo ratings yet
- New Progress in Diagnosis and Treatment of Pulmonary Arterial HypertensionDocument9 pagesNew Progress in Diagnosis and Treatment of Pulmonary Arterial HypertensionRhahahaNo ratings yet
- Pulmonary Hipertension PDFDocument481 pagesPulmonary Hipertension PDFRadhiatul AdillahNo ratings yet
- Diagnosis of Pulmonary HypertensionDocument12 pagesDiagnosis of Pulmonary HypertensionFaridaFaradillaPutryCherewetNo ratings yet
- Pulmonary HipertensionDocument481 pagesPulmonary HipertensionFransiskus A Danu KrisbiantoroNo ratings yet
- WSPH 2019Document15 pagesWSPH 2019Faisol SiddiqNo ratings yet
- Jama 2022 327 1379Document13 pagesJama 2022 327 1379silviaNo ratings yet
- Revised Definition of Pulmonary Hypertension and Approach To Management: A Clinical PrimerDocument8 pagesRevised Definition of Pulmonary Hypertension and Approach To Management: A Clinical PrimerRhahahaNo ratings yet
- Vias Moleculares HapDocument24 pagesVias Moleculares Hapdayanachuquimia95No ratings yet
- Pharmaceuticals 15 01242Document29 pagesPharmaceuticals 15 01242gadangNo ratings yet
- Clinical Update On Pulmonary Hypertension: Salim Yaghi, Anastasia Novikov, Theo TrandafirescuDocument7 pagesClinical Update On Pulmonary Hypertension: Salim Yaghi, Anastasia Novikov, Theo TrandafirescuIs DGNo ratings yet
- 肺动脉高压诊治临床路径Document13 pages肺动脉高压诊治临床路径zjjszflNo ratings yet
- JR Hipertensi Pulmonal Rizki AmaliyahDocument11 pagesJR Hipertensi Pulmonal Rizki AmaliyahnengahdarmawanNo ratings yet
- Maron 2023 Revised Definition of Pulmonary Hypertension and Approach To Management A Clinical PrimerDocument8 pagesMaron 2023 Revised Definition of Pulmonary Hypertension and Approach To Management A Clinical PrimerDaniel ForeroNo ratings yet
- Guideline USA 2020Document16 pagesGuideline USA 2020Rodrigo Felipe Albuquerque Paiva de OliveiraNo ratings yet
- Circulationaha 114 006971Document11 pagesCirculationaha 114 006971RhahahaNo ratings yet
- Pulmonary Arterial Hypertension: The Burden of Disease and Impact On Quality of LifeDocument9 pagesPulmonary Arterial Hypertension: The Burden of Disease and Impact On Quality of LifeMeilani Azaria SNo ratings yet
- Ijms 24 08462Document4 pagesIjms 24 08462RhahahaNo ratings yet
- Err 0099 2020Document12 pagesErr 0099 2020Faradiba MaricarNo ratings yet
- Pulmon AlDocument1 pagePulmon AlBrisney AureliaNo ratings yet
- 1 s2.0 S1053077021005723 MainDocument13 pages1 s2.0 S1053077021005723 Main8mjy475v9mNo ratings yet
- Additional 3Document12 pagesAdditional 3Bagus Radityo AmienNo ratings yet
- Pulmonary HypertensionDocument8 pagesPulmonary HypertensionSebastian BarreraNo ratings yet
- Hipertensión PulmonarDocument13 pagesHipertensión PulmonarBrayam Emerson Calderón RecaldeNo ratings yet
- Approach To Pulmonary Hypertension From CT To Clinical DiagnosisDocument17 pagesApproach To Pulmonary Hypertension From CT To Clinical DiagnosisnancyNo ratings yet
- Epidemiology of Pulmonary HypertensionDocument19 pagesEpidemiology of Pulmonary HypertensionzulemerlanoNo ratings yet
- Jama Ruopp 2022 RV 220007 1662040577.72953Document13 pagesJama Ruopp 2022 RV 220007 1662040577.72953Yo MeNo ratings yet
- PAH Ann Intern Med 2013Document15 pagesPAH Ann Intern Med 2013waterprincess100% (1)
- Póster 1Document3 pagesPóster 1Dan Medina OrtizNo ratings yet
- Chest Julio 2022 Hipertension Pulm en ILDDocument11 pagesChest Julio 2022 Hipertension Pulm en ILDnoeliaNo ratings yet
- Updated 20 Classification 20 and 20 Management 20 of 20 Pulmonary 20 HypertensionDocument10 pagesUpdated 20 Classification 20 and 20 Management 20 of 20 Pulmonary 20 HypertensionAarlettejimenezNo ratings yet
- Pulmonary Veno-Occlusive Disease An Important Consideration in PatientsDocument7 pagesPulmonary Veno-Occlusive Disease An Important Consideration in PatientsأنيسNo ratings yet
- Hipertensi PulmonalDocument5 pagesHipertensi PulmonalSteven RichardNo ratings yet
- 1 s2.0 S0012369219300029 MainDocument22 pages1 s2.0 S0012369219300029 MainbrandusaNo ratings yet
- Hipertension Pulmonar Tto Lancet 2023Document16 pagesHipertension Pulmonar Tto Lancet 2023alejandro RodriguezNo ratings yet
- HTPAnnals 2005Document12 pagesHTPAnnals 2005api-3703544No ratings yet
- Tratment Oh HIV-PAHDocument34 pagesTratment Oh HIV-PAHFelisa Nur KhayanaNo ratings yet
- Recent Advances in Pulmonary HypertensionDocument12 pagesRecent Advances in Pulmonary Hypertensionflying highNo ratings yet
- Psychosocial Aspects of Pulmonary Hypertension: A Review: J M. W, P .D., G L, M.D. V M L, M.D., M R, M.D. M R, M.DDocument9 pagesPsychosocial Aspects of Pulmonary Hypertension: A Review: J M. W, P .D., G L, M.D. V M L, M.D., M R, M.D. M R, M.DNedelcuCMNo ratings yet
- Pulmonary HTN. ESC POCKET GLS 2022. Larger Font. For PrintingDocument79 pagesPulmonary HTN. ESC POCKET GLS 2022. Larger Font. For PrintingGeoNo ratings yet
- Prognostic Factors in Pulmonary Arterial Hypertension: Literature ReviewDocument5 pagesPrognostic Factors in Pulmonary Arterial Hypertension: Literature Reviewhuda riyambodoNo ratings yet
- South Africa A Global View of Pulmonary HypertensionDocument17 pagesSouth Africa A Global View of Pulmonary HypertensionDhan RamadhanNo ratings yet
- Hoeper 2016Document14 pagesHoeper 2016riyad saksakNo ratings yet
- Medicina: Pulmonary Hypertension in COPD: A Case Study and Review of The LiteratureDocument8 pagesMedicina: Pulmonary Hypertension in COPD: A Case Study and Review of The Literatureguhan taraNo ratings yet
- Modern Invasive Hemodynamic Assessment of Pulmonary HypertensionDocument11 pagesModern Invasive Hemodynamic Assessment of Pulmonary HypertensionfabiolaNo ratings yet
- British J Pharmacology - 2021 - DignamDocument27 pagesBritish J Pharmacology - 2021 - DignamLinda Silvana SariNo ratings yet
- HT PedDocument18 pagesHT PedLina María CañónNo ratings yet
- Pulmonary HypertensionDocument20 pagesPulmonary Hypertensionyelsinosmin romeroalvaradoNo ratings yet
- Hemodynamic Indices in Pulmonary Hypertension: A Narrative ReviewDocument15 pagesHemodynamic Indices in Pulmonary Hypertension: A Narrative ReviewfabiolaNo ratings yet
- Pulmonary Hypertension: Annals of Internal MedicinetDocument16 pagesPulmonary Hypertension: Annals of Internal MedicinetAlicia TGNo ratings yet
- 2022 PH Guidelines - Essential MessagesDocument10 pages2022 PH Guidelines - Essential MessagesRoyNo ratings yet
- Management Strategies For Patients With Pulmonary Hypertension in The Intensive Care UnitDocument14 pagesManagement Strategies For Patients With Pulmonary Hypertension in The Intensive Care Unitanon-374465No ratings yet
- Pulmonary Hypertension Mediastinal FibrosisDocument10 pagesPulmonary Hypertension Mediastinal FibrosisAndreiSefNo ratings yet
- PAH Lessons From A Cancer Final VersionDocument11 pagesPAH Lessons From A Cancer Final VersionAndreiSefNo ratings yet
- COPD: A Guide to Diagnosis and Clinical ManagementFrom EverandCOPD: A Guide to Diagnosis and Clinical ManagementNicola A. HananiaNo ratings yet
- Potential of Non-Conventional Source of Energy and Associated Environmental Issue: An Indian ScenarioDocument6 pagesPotential of Non-Conventional Source of Energy and Associated Environmental Issue: An Indian ScenarioSanchit PatilNo ratings yet
- A Review On Tecoma StansDocument3 pagesA Review On Tecoma StansBaru Chandrasekhar RaoNo ratings yet
- 5085DL / 5055DL SeriesDocument2 pages5085DL / 5055DL SeriesMinh TranNo ratings yet
- Cakes and IcingsDocument2 pagesCakes and Icingsgian jorgioNo ratings yet
- Summer Training Report On: "Consumer Perception Towards Online Shopping"Document83 pagesSummer Training Report On: "Consumer Perception Towards Online Shopping"Swati TanwarNo ratings yet
- Full Text 01Document113 pagesFull Text 01Anonymous GUitcVONo ratings yet
- Long-Term Effects Fertilizers Yield Soil Fertility Winter Wheat-Maize System in Jiangsu, China 'Document8 pagesLong-Term Effects Fertilizers Yield Soil Fertility Winter Wheat-Maize System in Jiangsu, China 'wisnuaji wibowoNo ratings yet
- Mark Scheme (Results) November 2009: IGCSE Biology (4325) Paper 2HDocument16 pagesMark Scheme (Results) November 2009: IGCSE Biology (4325) Paper 2HmuhajireenNo ratings yet
- ΕΓΧΕΙΡΙΔΙΟ ΠΛΥΝΤΗΡΙΟΥ ΠΙΑΤΩΝ - ΑΝΤΑΛΛΑΚΤΙΚΑDocument16 pagesΕΓΧΕΙΡΙΔΙΟ ΠΛΥΝΤΗΡΙΟΥ ΠΙΑΤΩΝ - ΑΝΤΑΛΛΑΚΤΙΚΑΤΣΙΜΠΙΔΗΣ ΠΑΝΑΓΙΩΤΗΣNo ratings yet
- Added Scenes For - Tattered FatesDocument19 pagesAdded Scenes For - Tattered FatesRadosław KwiecińskiNo ratings yet
- GRI 180-12-B-W1K Data SheetDocument3 pagesGRI 180-12-B-W1K Data SheetJMAC SupplyNo ratings yet
- One Dimensional Heat EquationDocument30 pagesOne Dimensional Heat Equation20-317 RithvikNo ratings yet
- Basic Summary of X-Ray Equipment - Naver BlogDocument7 pagesBasic Summary of X-Ray Equipment - Naver BlogMalikAlrahabiNo ratings yet
- GALLO-SCYTHIANS - Celtic Ukraine (By Mac Congail)Document22 pagesGALLO-SCYTHIANS - Celtic Ukraine (By Mac Congail)Toma100% (1)
- Therblig Color Symbol/Icon Therblig Color Symbol/Icon: Search Black Use PurpleDocument10 pagesTherblig Color Symbol/Icon Therblig Color Symbol/Icon: Search Black Use Purplechad macatangayNo ratings yet
- IUPAC & Nomenclature PDFDocument6 pagesIUPAC & Nomenclature PDFjaspreet singh100% (1)
- Gamesa G90 2mwDocument6 pagesGamesa G90 2mwNemanja KomatinovicNo ratings yet
- Kepco KpsDocument27 pagesKepco Kps허준No ratings yet
- Procedure For Equipment Calibration and MaintenanceDocument9 pagesProcedure For Equipment Calibration and MaintenanceAli HadiNo ratings yet
- Compilations of Board Exam Problem1 PDFDocument65 pagesCompilations of Board Exam Problem1 PDFJevan Calaque100% (1)
- Bonn & Gaston 2005 Richness Ecosystem Conserv SAfDocument18 pagesBonn & Gaston 2005 Richness Ecosystem Conserv SAfKellyta RodriguezNo ratings yet
- Datasheet VisiTouch-Pac V1.3 ENDocument8 pagesDatasheet VisiTouch-Pac V1.3 ENDavid CalderonNo ratings yet
- University of Cambridge International Examinations International General Certificate of Secondary EducationDocument20 pagesUniversity of Cambridge International Examinations International General Certificate of Secondary Educationluines78No ratings yet
- Worked Example To Eurocode 2 Vol 1Document228 pagesWorked Example To Eurocode 2 Vol 1Mohd RafiqNo ratings yet
- Planning and Designing of Bridge Over Solani RiverDocument5 pagesPlanning and Designing of Bridge Over Solani RiverCurious RajNo ratings yet
- Precision t7810 Workstation - Owners Manual - en UsDocument58 pagesPrecision t7810 Workstation - Owners Manual - en Usfotograf nuntaNo ratings yet
- Arsenic Presentation 11111Document19 pagesArsenic Presentation 11111Namrata PalNo ratings yet
- IHKS Summit ProgramDocument35 pagesIHKS Summit ProgramDiah Rahayu SetiawatiNo ratings yet
- PhET Simulation - Determination of Planck's ConstantDocument3 pagesPhET Simulation - Determination of Planck's ConstantDaniel CruzNo ratings yet