Download as pdf or txt
You might also like
- When The World Goes Quiet - Gian SardarDocument283 pagesWhen The World Goes Quiet - Gian Sardarmengchhoungleang.cbvhNo ratings yet
- Prevalence of Eating Disorders Over The 2000-2018 Period: A Systematic Literature ReviewDocument12 pagesPrevalence of Eating Disorders Over The 2000-2018 Period: A Systematic Literature ReviewRahman FirmansyahNo ratings yet
- Galmiche 2019 Prevalence EDDocument12 pagesGalmiche 2019 Prevalence EDCésar BlancoNo ratings yet
- Prevalence of Eating Disorders Over The 2000-2018 PeriodDocument12 pagesPrevalence of Eating Disorders Over The 2000-2018 PeriodloloasbNo ratings yet
- (ARTIGO) ARCELUS, Et Al. - Prevalence of Eating Disorders Amongst Dancers. A Systemic Review and Meta-Analysis (2013) - PUBMEDDocument28 pages(ARTIGO) ARCELUS, Et Al. - Prevalence of Eating Disorders Amongst Dancers. A Systemic Review and Meta-Analysis (2013) - PUBMEDGuido BrustNo ratings yet
- Development of The Pica, ARFID, and Rumination Disorder Interview, A Multi-Informant, Semi-Structured Interview of Feeding Disorders Across The Lifespan: A Pilot Study For Ages 10 - 22Document10 pagesDevelopment of The Pica, ARFID, and Rumination Disorder Interview, A Multi-Informant, Semi-Structured Interview of Feeding Disorders Across The Lifespan: A Pilot Study For Ages 10 - 22LAURA CRISTINA TORRES CATANONo ratings yet
- The Follow-Up of Eating Disorders From Adolescence To Early Adulthood: A Systematic ReviewDocument19 pagesThe Follow-Up of Eating Disorders From Adolescence To Early Adulthood: A Systematic ReviewAnahi MaciasNo ratings yet
- 10 1002@eat 23236Document12 pages10 1002@eat 23236LucíaNo ratings yet
- 1983 Garner EDIDocument22 pages1983 Garner EDIAzyan ShahiraNo ratings yet
- Garner 1983Document20 pagesGarner 1983Putri Aurora AngelinaNo ratings yet
- Psy Project 2nd SemDocument28 pagesPsy Project 2nd SemShashwat SinghNo ratings yet
- Binge Eating y DepressionDocument10 pagesBinge Eating y DepressionGemma Ortiz100% (1)
- Hilbert 2012Document7 pagesHilbert 2012pentrucanva1No ratings yet
- Geriatric Malnutrition and DepressionDocument5 pagesGeriatric Malnutrition and DepressionCamila VasquesNo ratings yet
- Prevalence of Orthorexia Nervosa in University Students and Its Relationship With Psychopathological Aspects of Eating Behaviour DisordersDocument8 pagesPrevalence of Orthorexia Nervosa in University Students and Its Relationship With Psychopathological Aspects of Eating Behaviour DisordersSAMARPITANo ratings yet
- Dietary Patterns and Depression Risk A Meta AnalysisDocument10 pagesDietary Patterns and Depression Risk A Meta AnalysisGrasiela JunqueiraNo ratings yet
- May-Article OlfactionDocument16 pagesMay-Article Olfactionlammarisoumayya1No ratings yet
- Hoek 2003Document14 pagesHoek 2003Kariena PermanasariNo ratings yet
- Epidemiology of Eating Disorders: Incidence, Prevalence and Mortality RatesDocument9 pagesEpidemiology of Eating Disorders: Incidence, Prevalence and Mortality RatesVictória NamurNo ratings yet
- Vegetarianism and Eating Disorders The Subjective Experience ofDocument8 pagesVegetarianism and Eating Disorders The Subjective Experience ofnawaf14asNo ratings yet
- REDALYGDocument8 pagesREDALYGjoel cedeño SánchezNo ratings yet
- Eating Disorders CPGDocument62 pagesEating Disorders CPGLuis Pablo HsNo ratings yet
- Trend of Nutrition Research in Endocrine Disorders, Gaps, and Future Plans A Collection of Experiences of An Endocrinology Research InstituteDocument8 pagesTrend of Nutrition Research in Endocrine Disorders, Gaps, and Future Plans A Collection of Experiences of An Endocrinology Research InstituteChawki MokademNo ratings yet
- Funcionalidad Familiar y Diabetes Mellitus Tipo 2Document4 pagesFuncionalidad Familiar y Diabetes Mellitus Tipo 2Jose Luis Bustamante CarrascoNo ratings yet
- Psychiatric and Medical Correlates of DSM-5 Eating Disorders in A Nationally Representative Sample of Adults in The United StatesDocument9 pagesPsychiatric and Medical Correlates of DSM-5 Eating Disorders in A Nationally Representative Sample of Adults in The United StatesManny RosengallegosNo ratings yet
- 10 1002@eat 23366Document11 pages10 1002@eat 23366LucíaNo ratings yet
- NPP 2015275Document10 pagesNPP 2015275Weverson LinharesNo ratings yet
- Nutritional TherapyDocument13 pagesNutritional TherapyAl VileoNo ratings yet
- Antidepresivos y PesoDocument11 pagesAntidepresivos y Pesogtellez25No ratings yet
- Intl J Eating Disorders - 2020 - Hilbert - Psychometric Evaluation of The Eating Disorders in Youth Questionnaire When UsedDocument10 pagesIntl J Eating Disorders - 2020 - Hilbert - Psychometric Evaluation of The Eating Disorders in Youth Questionnaire When UsedKariena PermanasariNo ratings yet
- Guia Practica DMI y DMIIDocument21 pagesGuia Practica DMI y DMIICamila Paz Colunche NuñezNo ratings yet
- BourneDocument21 pagesBourneNelson Syah HabibiNo ratings yet
- Mental Health Effet 1Document21 pagesMental Health Effet 1Mostafa McheikNo ratings yet
- Medical Management Restrictive EDs 2022Document7 pagesMedical Management Restrictive EDs 2022SaturniineNo ratings yet
- Castellini 2018Document13 pagesCastellini 2018Maria GemescuNo ratings yet
- The Hidden Burden of Eating Disorders An Extension of Estimates From The Global Burden of Disease StudyDocument9 pagesThe Hidden Burden of Eating Disorders An Extension of Estimates From The Global Burden of Disease StudyDannte GBNo ratings yet
- Family Functioning Is Related To Health Behaviors in Patients With Type 2 Diabetes MellitusDocument5 pagesFamily Functioning Is Related To Health Behaviors in Patients With Type 2 Diabetes MellitusEliseo Lopz HnandzNo ratings yet
- Prevalence of Metabolic Syndrome in Iran A Meta-Analysis of 69 StudiesDocument8 pagesPrevalence of Metabolic Syndrome in Iran A Meta-Analysis of 69 StudiesNancy Aidée Reyes MéndezNo ratings yet
- Childhood Maltreatment and Eating Disorder Pathology: A Systematic Review and Dose-Response Meta-AnalysisDocument15 pagesChildhood Maltreatment and Eating Disorder Pathology: A Systematic Review and Dose-Response Meta-AnalysisMaria GemescuNo ratings yet
- mYFAS2 ValidationpaperDocument7 pagesmYFAS2 Validationpaperzgcsj8ht5sNo ratings yet
- 2012 Article 282 PDFDocument9 pages2012 Article 282 PDFDrAnisha PatelNo ratings yet
- Intl J Eating Disorders - 2018 - Nazar - An Examination of The Clinical Outcomes of Adolescents and Young Adults With BroadDocument6 pagesIntl J Eating Disorders - 2018 - Nazar - An Examination of The Clinical Outcomes of Adolescents and Young Adults With BroadYamely CamachoNo ratings yet
- Udo Et Al-2019-International Journal of Eating DisordersDocument11 pagesUdo Et Al-2019-International Journal of Eating DisordersMonicaVCamarenaNo ratings yet
- Epidemiology of Eating Disorders, Eating Disordered Behaviour, and Body Image Disturbance in MalesDocument9 pagesEpidemiology of Eating Disorders, Eating Disordered Behaviour, and Body Image Disturbance in Malesgim absalNo ratings yet
- 1 s2.0 S030645222100573X MainDocument16 pages1 s2.0 S030645222100573X Mainmostafa dawoudNo ratings yet
- Prevalence of Depression Symptoms in Diabetes Mellitus: Salih EkerDocument4 pagesPrevalence of Depression Symptoms in Diabetes Mellitus: Salih EkerNathayaNeilaVarneliaNo ratings yet
- Hubungan Gerd Dengan DepresiDocument8 pagesHubungan Gerd Dengan DepresiDella Elvina RoeslandNo ratings yet
- Adherence of Psychopharmacological Prescriptions To Clinical PDFDocument9 pagesAdherence of Psychopharmacological Prescriptions To Clinical PDFGaby ZavalaNo ratings yet
- Characteristics of Avoidant-Restrictive Food Intake Disorder in A General Pediatric Inpatient SampleDocument49 pagesCharacteristics of Avoidant-Restrictive Food Intake Disorder in A General Pediatric Inpatient SampleAmiLia CandrasariNo ratings yet
- Original Papers: The Lifetime Prevalence of Anxiety Disorders Among Patients With Irritable Bowel SyndromeDocument6 pagesOriginal Papers: The Lifetime Prevalence of Anxiety Disorders Among Patients With Irritable Bowel Syndromeapi-193771047No ratings yet
- Diet Quality in Persons With and Without Depressiv 2018 Journal of PsychiatrDocument7 pagesDiet Quality in Persons With and Without Depressiv 2018 Journal of Psychiatrgiulia.santinNo ratings yet
- Eating Disorders - Overview of Epidemiology, Clinical Features, and Diagnosis - UpToDateDocument39 pagesEating Disorders - Overview of Epidemiology, Clinical Features, and Diagnosis - UpToDateDylanNo ratings yet
- 3 - Higher Prevalence of Irritable Bowel Syndrome and Greater Gastrointestinal Symptoms in Obsessive-Compulsive DisorderDocument6 pages3 - Higher Prevalence of Irritable Bowel Syndrome and Greater Gastrointestinal Symptoms in Obsessive-Compulsive DisorderPaula CantalapiedraNo ratings yet
- 1 s2.0 S0165032718328222 MainDocument7 pages1 s2.0 S0165032718328222 MainTulaNo ratings yet
- Epidemiologia TCADocument4 pagesEpidemiologia TCAmaitte orellanaNo ratings yet
- 449041-Texto Del Artículo-1709821-1-10-20210804Document7 pages449041-Texto Del Artículo-1709821-1-10-20210804María José Coronado VillarrealNo ratings yet
- The Difficulties in Emotional Regulation Among A Cohort of Females With LipedemaDocument9 pagesThe Difficulties in Emotional Regulation Among A Cohort of Females With Lipedemar.barca98No ratings yet
- Articles Summary Health PsyDocument5 pagesArticles Summary Health Psyhadiqaasif01No ratings yet
- Nuac 058Document14 pagesNuac 058rghvakumarNo ratings yet
- Ageing Research Reviews: Annabel P. Matison, Karen A. Mather, Victoria M. Flood, Simone ReppermundDocument18 pagesAgeing Research Reviews: Annabel P. Matison, Karen A. Mather, Victoria M. Flood, Simone ReppermundMasithaNo ratings yet
- The Prevention and Treatment of Disease with a Plant-Based Diet Volume 2: Evidence-based articles to guide the physicianFrom EverandThe Prevention and Treatment of Disease with a Plant-Based Diet Volume 2: Evidence-based articles to guide the physicianNo ratings yet
- Zaharizan Binti Mat ZinDocument189 pagesZaharizan Binti Mat Zinbluebell31088No ratings yet
- 1.the Cold War and VietnamDocument5 pages1.the Cold War and VietnamMateo HenaoNo ratings yet
- Case Study Talent ManagementDocument2 pagesCase Study Talent ManagementaparnashastriNo ratings yet
- Tor Ic Adri - 2Document7 pagesTor Ic Adri - 2herri susantoNo ratings yet
- Basics of Aircraft Market Analysis v1Document30 pagesBasics of Aircraft Market Analysis v1avianovaNo ratings yet
- Hawaii HB1116 - Legislation To Release Birth Records of "Person of Civic Prominence" AKA Obama For $100.00 Fee - 2011Document9 pagesHawaii HB1116 - Legislation To Release Birth Records of "Person of Civic Prominence" AKA Obama For $100.00 Fee - 2011ObamaRelease YourRecordsNo ratings yet
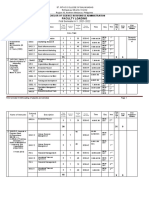
- BSBA FINAL LOADING For BOT 2021-2022 1st SEMESTERDocument5 pagesBSBA FINAL LOADING For BOT 2021-2022 1st SEMESTERMaureen GalendezNo ratings yet
- Featured Chaim BloomDocument2 pagesFeatured Chaim Bloomapi-583037485No ratings yet
- Monitoring and Evaluation Assistant Cover LetterDocument6 pagesMonitoring and Evaluation Assistant Cover Letteremlwymjbf100% (2)
- In The Matter of The Disbarment of DominadorDocument2 pagesIn The Matter of The Disbarment of DominadorRen ConchaNo ratings yet
- Financial Management Notes - Dividend Decision - Dynamic Tutorials and ServicesDocument10 pagesFinancial Management Notes - Dividend Decision - Dynamic Tutorials and Servicessimranarora2007No ratings yet
- Quiz - Which Christlike Attribute Should You Work OnDocument4 pagesQuiz - Which Christlike Attribute Should You Work Ondiego.almeidNo ratings yet
- LGBT FactsDocument43 pagesLGBT Factsjohn kaneNo ratings yet
- The History of The Popes From The Close of The Middle Ages 1891 Vol 37Document480 pagesThe History of The Popes From The Close of The Middle Ages 1891 Vol 37ammgmNo ratings yet
- Follow Up LessonsDocument11 pagesFollow Up LessonsFrancisco NiegasNo ratings yet
- United States Court of Appeals: For The First CircuitDocument34 pagesUnited States Court of Appeals: For The First CircuitScribd Government DocsNo ratings yet
- MA Thesis Proposal - Arnab Dutta GoeGroDocument7 pagesMA Thesis Proposal - Arnab Dutta GoeGroArnab DuttaNo ratings yet
- Flight Ops - Cost Index Database PDFDocument15 pagesFlight Ops - Cost Index Database PDFDiego RangelNo ratings yet
- Examine Any 5 Determinants of Social Policy in Developing CountriesDocument8 pagesExamine Any 5 Determinants of Social Policy in Developing Countriestendai precious nyamadzaoNo ratings yet
- LS 101 Daylighting Controller Cut SheetDocument6 pagesLS 101 Daylighting Controller Cut SheetIgor NiculovicNo ratings yet
- Daftar Siswa Melanjutkan (AL ISLAM & MANDALA)Document4 pagesDaftar Siswa Melanjutkan (AL ISLAM & MANDALA)Agus furnamaNo ratings yet
- Labor Review Digest On LabstandDocument300 pagesLabor Review Digest On LabstandAudreyNo ratings yet
- 2022 JOAP Remedial Law Mock Bar ExaminationDocument14 pages2022 JOAP Remedial Law Mock Bar ExaminationVincent Jave GutierrezNo ratings yet
- Daftar Isi Speaker Murottal Al Qur'an - 16gbDocument29 pagesDaftar Isi Speaker Murottal Al Qur'an - 16gbrahmat fajar94% (31)
- Corey and Oats inDocument3 pagesCorey and Oats inrealnatahanfNo ratings yet
- Isoiec11801-Cor3 (Ed2 0) en PDFDocument2 pagesIsoiec11801-Cor3 (Ed2 0) en PDFShubham KaklijNo ratings yet
- Magna Carta of PWDDocument56 pagesMagna Carta of PWDPatrice De CastroNo ratings yet
- History of Ord SchoolDocument6 pagesHistory of Ord SchoolCOLONEL ZIKRIANo ratings yet
- Aadhar Update CertificateDocument1 pageAadhar Update CertificateMAMATHA XEROX AND RECHARGES 2No ratings yet