Download as pdf or txt
You might also like
- 2021 ACLS Study GuideDocument20 pages2021 ACLS Study GuideShane Brown86% (14)
- Nursing Care Plan 6 Impaired Gas ExchangeDocument9 pagesNursing Care Plan 6 Impaired Gas Exchangedbryant0101100% (12)
- Filing # 120208791 E-Filed 01/25/2021 07:26:55 PMDocument67 pagesFiling # 120208791 E-Filed 01/25/2021 07:26:55 PMthe next miami100% (1)
- Sample Scoping ReportDocument92 pagesSample Scoping ReportEm Mar0% (1)
- Project Proposal On Dairy FarmDocument26 pagesProject Proposal On Dairy Farmvector dairy88% (8)
- MD 11fgnDocument3 pagesMD 11fgnMcDonnell Douglas MD-110% (7)
- RFH COVID-19 ICU Resource Pack FULL PDFDocument15 pagesRFH COVID-19 ICU Resource Pack FULL PDFQuique GarciaNo ratings yet
- Vasopressors and InotropesDocument31 pagesVasopressors and InotropesReza Prakosa SedyatamaNo ratings yet
- Tesla Motors Expansion StrategyDocument26 pagesTesla Motors Expansion StrategyVu Nguyen75% (4)
- RSI & Status Asthmaticus: Drug Dose Onset/duration Cons ProsDocument2 pagesRSI & Status Asthmaticus: Drug Dose Onset/duration Cons ProsAfina Abdul AzizNo ratings yet
- High-Flow Nasal Cannula-Protocol For Initiation, Titration and WeaningDocument3 pagesHigh-Flow Nasal Cannula-Protocol For Initiation, Titration and WeaningMahmoud khedrNo ratings yet
- Management of Acute Exacerbation in Children: Dr. Raghvendra Singh Senior Resident K.S.C.HDocument18 pagesManagement of Acute Exacerbation in Children: Dr. Raghvendra Singh Senior Resident K.S.C.HDr Amit BishnoiNo ratings yet
- CC Final Study Guide 1Document21 pagesCC Final Study Guide 1api-402814755No ratings yet
- Rapid Sequence Intubation: Mask and MonitoringDocument6 pagesRapid Sequence Intubation: Mask and MonitoringHatim DziauddinNo ratings yet
- Airway ManagementDocument4 pagesAirway ManagementEllamae DerupeNo ratings yet
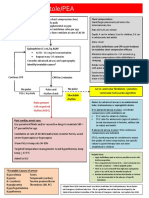
- Asystole/PEA: Epinephrine 0.1 ML/KG ASAPDocument1 pageAsystole/PEA: Epinephrine 0.1 ML/KG ASAPAlejandro MusaNo ratings yet
- Comprehensive Life Support Tutorial Case 1: Question/Action Information Note/Reference TipsDocument3 pagesComprehensive Life Support Tutorial Case 1: Question/Action Information Note/Reference Tipshyukkie minnieNo ratings yet
- DR Lily - Resp Distress in Newborn Infants PDFDocument45 pagesDR Lily - Resp Distress in Newborn Infants PDFM Ilham MNo ratings yet
- Increasing and Decreasing Repspiratory Support PDFDocument1 pageIncreasing and Decreasing Repspiratory Support PDFÖzgür Barışcan KayaNo ratings yet
- Postanesthesia Care: Dhany BudipratamaDocument36 pagesPostanesthesia Care: Dhany BudipratamaAbu Bakr Ar RaziNo ratings yet
- WB COVID19 Latest Treatment ProtocolDocument1 pageWB COVID19 Latest Treatment ProtocolRahul AwasthiNo ratings yet
- Bronchiolitis: See AlsoDocument6 pagesBronchiolitis: See AlsoJuleides De LeonNo ratings yet
- Status Asthmaticus: Triwahju AstutiDocument41 pagesStatus Asthmaticus: Triwahju AstutirianiNo ratings yet
- NIV and HFNCDocument16 pagesNIV and HFNCMarceline GarciaNo ratings yet
- Asma 1Document8 pagesAsma 1punkgatitNo ratings yet
- Chapter 36V3Document25 pagesChapter 36V3عباس أحمد الشيخ جعفرNo ratings yet
- Case 4Document11 pagesCase 4Shakshi RainaNo ratings yet
- Post Arrest CareDocument23 pagesPost Arrest CareMohamed RasoolNo ratings yet
- NPPVDocument29 pagesNPPVStephanie SusavageNo ratings yet
- 01 - Bronchial AsthmaDocument6 pages01 - Bronchial AsthmaFrank VaronaNo ratings yet
- GINA AlgorithmDocument6 pagesGINA AlgorithmMarcela YolinaNo ratings yet
- Emergencies-Pulmonary OedemaDocument1 pageEmergencies-Pulmonary OedemaMaimoona AimanNo ratings yet
- Nursing Intervention Respiratory Status: Ventilation Respiratory Status: Airway Patency Vital Sign StatusDocument12 pagesNursing Intervention Respiratory Status: Ventilation Respiratory Status: Airway Patency Vital Sign StatusSepti MemorisaNo ratings yet
- Respiratory Rules 2013Document20 pagesRespiratory Rules 2013kawaiiriceNo ratings yet
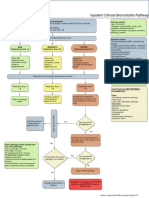
- Bronchiolitis Pathway InpatientDocument1 pageBronchiolitis Pathway Inpatientd'Agung NugrohoNo ratings yet
- Supplementary Material 1a Acute AsthmaDocument3 pagesSupplementary Material 1a Acute AsthmaJanela Chriselle B. TICARNo ratings yet
- Asthma: Treatment and ManagementDocument54 pagesAsthma: Treatment and ManagementEndah susantiNo ratings yet
- 3 Combined AHA BLS ACLS Updates CombinedDocument5 pages3 Combined AHA BLS ACLS Updates Combinedamanrup randhawa100% (1)
- Overview of Respiratory Failure & Use of Mechanical VentilationDocument89 pagesOverview of Respiratory Failure & Use of Mechanical VentilationsheharyarNo ratings yet
- Nueva Ecija University of Science and Technology: Case 7Document7 pagesNueva Ecija University of Science and Technology: Case 7jomariNo ratings yet
- Niv HFNCDocument15 pagesNiv HFNCFrank VaronaNo ratings yet
- Seven Ps For RSI BOARDDocument2 pagesSeven Ps For RSI BOARDJames BrownNo ratings yet
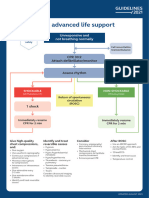
- 8-Adult Advanced Life Support Algorithm 2021Document1 page8-Adult Advanced Life Support Algorithm 2021khaledNo ratings yet
- Aclspediatric BradycardiaDocument2 pagesAclspediatric BradycardiasalamredNo ratings yet
- Adult Advanced Life Support Algorithm 2021 Aug 2023Document1 pageAdult Advanced Life Support Algorithm 2021 Aug 2023cknihilnewNo ratings yet
- NCP - Or-Rotation 2Document12 pagesNCP - Or-Rotation 2Vian RiveraNo ratings yet
- DR Sujata: Professor Dept - of Anaesthesiology &critical Care Ucms & GTB HospitalDocument53 pagesDR Sujata: Professor Dept - of Anaesthesiology &critical Care Ucms & GTB HospitalMiniNo ratings yet
- RahpoDocument3 pagesRahpoassouma16052002No ratings yet
- A (ACLS) - 2015: Dvanced Cardiac Life SupportDocument52 pagesA (ACLS) - 2015: Dvanced Cardiac Life SupportNajmussaqibNo ratings yet
- AIIMS COVID Doc 1.6.1-1Document1 pageAIIMS COVID Doc 1.6.1-1mbhangaleNo ratings yet
- HFOV High-Frequency-Oscillatory-VentilationDocument22 pagesHFOV High-Frequency-Oscillatory-VentilationJZNo ratings yet
- PRIORITY 2: Impaired Gas Exchange Related To Excessive or Thick Secretions Tree Secondary To PneumoniaDocument4 pagesPRIORITY 2: Impaired Gas Exchange Related To Excessive or Thick Secretions Tree Secondary To PneumoniaElay Pedroso100% (1)
- Tutorial 6 - SedationDocument4 pagesTutorial 6 - SedationSNo ratings yet
- Pediatrics-Respiratory Disorders of The Newborn: Diseases Clinical Manifestations Diagnosis & Prognosis ManagementDocument9 pagesPediatrics-Respiratory Disorders of The Newborn: Diseases Clinical Manifestations Diagnosis & Prognosis ManagementJonathan ZumakpehNo ratings yet
- ICU One Pager ARDS v1.1Document1 pageICU One Pager ARDS v1.1Michael LevitNo ratings yet
- Oxygen TherapyDocument2 pagesOxygen TherapyPhilip MusonyeNo ratings yet
- Adult ALS-A3Document1 pageAdult ALS-A3jbruunsNo ratings yet
- BipapDocument26 pagesBipapالغائب الحاضرNo ratings yet
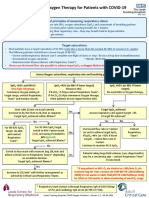
- Guidance On Oxygen Therapy For Patients With COVID-19: General Principles of Assessing Respiratory StatusDocument1 pageGuidance On Oxygen Therapy For Patients With COVID-19: General Principles of Assessing Respiratory StatusAsh mohamedNo ratings yet
- ICU One Pager Intubation ChecklistDocument4 pagesICU One Pager Intubation ChecklistCarlos Hernandez CamposNo ratings yet
- Drug-Assisted Intubation (Dai) : Expanded Scope Practice (NR)Document1 pageDrug-Assisted Intubation (Dai) : Expanded Scope Practice (NR)MEKSELINA KALENDERNo ratings yet
- Scenario Title: Community Acquired Pneumonia Learning Outcomes: 1. Assessment and Recognition of The Signs and Symptoms of PneumoniaDocument6 pagesScenario Title: Community Acquired Pneumonia Learning Outcomes: 1. Assessment and Recognition of The Signs and Symptoms of PneumoniaDud AccNo ratings yet
- Respiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsFrom EverandRespiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsJian-Xin ZhouNo ratings yet
- WWTP (Grit Chamber) - TDocument22 pagesWWTP (Grit Chamber) - TsarfaNo ratings yet
- OtooDocument11 pagesOtooStefania DavidNo ratings yet
- Shadow Presentation Photography IdeasDocument28 pagesShadow Presentation Photography IdeasagharizwanaliNo ratings yet
- CMA Pre Exam Test PDFDocument28 pagesCMA Pre Exam Test PDFVinay YerubandiNo ratings yet
- Nile International Freight ServicesDocument19 pagesNile International Freight ServicessameerhamadNo ratings yet
- Practical File AI - Class 10Document3 pagesPractical File AI - Class 10pawankvs2008No ratings yet
- Bluetooth 4.2 SpecificationDocument2,772 pagesBluetooth 4.2 SpecificationScott PooleNo ratings yet
- Free Iptv Ex - Yu Streams 11.07.14Document51 pagesFree Iptv Ex - Yu Streams 11.07.14bajra123No ratings yet
- Instructional Methods For Teaching Social Studies: A Survey of What Middle School Students Like and Dislike About Social Studies InstructionDocument4 pagesInstructional Methods For Teaching Social Studies: A Survey of What Middle School Students Like and Dislike About Social Studies InstructionShally GuptaNo ratings yet
- NLC English 7 Enhancement LP v.1Document85 pagesNLC English 7 Enhancement LP v.1patric maturan100% (1)
- Class 12 CS ProjectDocument27 pagesClass 12 CS ProjectKs100% (3)
- Tce Exam SNV S3Document9 pagesTce Exam SNV S3koubi enactaNo ratings yet
- Fruit Processing: Ömer Utku Çopur and Canan Ece TamerDocument28 pagesFruit Processing: Ömer Utku Çopur and Canan Ece TamerTan Hau VoNo ratings yet
- Structural Analysis of Complex Networks 2011Document501 pagesStructural Analysis of Complex Networks 2011kemalihsan_17959No ratings yet
- Engleza Maritima 4: 2a-SMCP External ROUTINE Communication - READING Comprehension-Book1Document5 pagesEngleza Maritima 4: 2a-SMCP External ROUTINE Communication - READING Comprehension-Book1dark959595No ratings yet
- Rapidraw Honey AnalysisDocument5 pagesRapidraw Honey AnalysistaufiqridzNo ratings yet
- National Security Act of 1947 PDFDocument142 pagesNational Security Act of 1947 PDFMax TaylorNo ratings yet
- Digital NativesDocument10 pagesDigital NativesJonathan Blanco Sa RiyadhNo ratings yet
- Anderson Distribution of The Correlation CoefficientDocument14 pagesAnderson Distribution of The Correlation Coefficientdauren_pcNo ratings yet
- First AId Notes - UpdatedDocument54 pagesFirst AId Notes - UpdatedewawireNo ratings yet
- How To Calculate Quantity of Bricks in WallDocument5 pagesHow To Calculate Quantity of Bricks in Wallواثق كريم نعيمNo ratings yet
- 3.3.2.3 Lab - Configuring Rapid PVST, PortFast, and BPDU GuardDocument9 pages3.3.2.3 Lab - Configuring Rapid PVST, PortFast, and BPDU Guardsebastian ruiz100% (1)
- Ge 4.500HP PDFDocument3 pagesGe 4.500HP PDFCarlos FiorilloNo ratings yet
- Color Powder Color ChartDocument4 pagesColor Powder Color ChartArif RusyanaNo ratings yet
- Ict Dos and DontsDocument5 pagesIct Dos and DontsLouwellaEredianoIbabaoNo ratings yet