Download as pdf or txt
You might also like
- Wongs Essentials of Pediatric Nursing 9th Edition Hockenberry Test BankDocument3 pagesWongs Essentials of Pediatric Nursing 9th Edition Hockenberry Test Banka488625443100% (1)
- Hepatocellular Carcinoma: Hepatocellular Carcinoma (HCC, Also Called Malignant Hepatoma) Is The MostDocument10 pagesHepatocellular Carcinoma: Hepatocellular Carcinoma (HCC, Also Called Malignant Hepatoma) Is The MostNurul An NisaNo ratings yet
- Hepatocellular Cancer: A Guide For The Internist: Review AJM Theme Issue: GastroenterologyDocument9 pagesHepatocellular Cancer: A Guide For The Internist: Review AJM Theme Issue: GastroenterologyCaerulus Fuad Abdul BaqiNo ratings yet
- HepatocarcinomDocument6 pagesHepatocarcinomAndreeaGheorgheNo ratings yet
- Diabetes and CancerDocument15 pagesDiabetes and CancerAriHendraWijayanti100% (1)
- Clinics in Liver Disease, Vol 12 PDFDocument229 pagesClinics in Liver Disease, Vol 12 PDFSrikanth YadavNo ratings yet
- Grundy 2008Document10 pagesGrundy 2008adipspain981No ratings yet
- (14796821 - Endocrine-Related Cancer) Diabetes and CancerDocument21 pages(14796821 - Endocrine-Related Cancer) Diabetes and CancerKami KamiNo ratings yet
- Cause, Pathogenesis, and Treatment of Nonalcoholic SteatohepatitisDocument10 pagesCause, Pathogenesis, and Treatment of Nonalcoholic SteatohepatitisGabriel VargasNo ratings yet
- hepatoCA 2Document9 pageshepatoCA 2Al VlaovicNo ratings yet
- Vigneri 2009Document21 pagesVigneri 2009Didin Tisna SayektiNo ratings yet
- Metformin and Reduced Risk of Hepatocellular Carcinoma in Diabetes With CLDDocument9 pagesMetformin and Reduced Risk of Hepatocellular Carcinoma in Diabetes With CLDNararto PrijogoNo ratings yet
- Diabetes Mellitus and Obesity As Risk Factors For Pancreatic CancerDocument13 pagesDiabetes Mellitus and Obesity As Risk Factors For Pancreatic CancerAsunción AncoNo ratings yet
- HCC HarrisonDocument5 pagesHCC HarrisonJesly CharliesNo ratings yet
- Lipid Disturbances in Breast Cancer Patients During ChemotherapyDocument11 pagesLipid Disturbances in Breast Cancer Patients During ChemotherapySteve GannabanNo ratings yet
- Obesidad y CirrosisDocument14 pagesObesidad y CirrosisMarly Tatiana Oviedo CaliNo ratings yet
- Nej MR A 1503519Document10 pagesNej MR A 1503519Mohammed KedirNo ratings yet
- Metabolic Syndrome and StrokeDocument5 pagesMetabolic Syndrome and StrokeEmir SaricNo ratings yet
- Colorectal Cancer&DiabetesDocument13 pagesColorectal Cancer&Diabetesperisici4_535458722No ratings yet
- Primer: Hepatocellular CarcinomaDocument28 pagesPrimer: Hepatocellular CarcinomaAinun Aii NoorNo ratings yet
- Dietary Fat and Risk of Renal Cell Carcinoma in The Usa A Casecontrol StudyDocument11 pagesDietary Fat and Risk of Renal Cell Carcinoma in The Usa A Casecontrol StudyMarko Sanja StikovicNo ratings yet
- Diabetes and Cancer: Paolo Vigneri, Francesco Frasca, Laura Sciacca, Giuseppe Pandini and Riccardo VigneriDocument21 pagesDiabetes and Cancer: Paolo Vigneri, Francesco Frasca, Laura Sciacca, Giuseppe Pandini and Riccardo VigneribrijeshandfamilyNo ratings yet
- Contemporary Reviews in Cardiovascular Medicine: Shared Risk Factors in Cardiovascular Disease and CancerDocument14 pagesContemporary Reviews in Cardiovascular Medicine: Shared Risk Factors in Cardiovascular Disease and CancerMuhammad NasirNo ratings yet
- Seminar: Jonathan D Mizrahi, Rishi Surana, Juan W Valle, Rachna T ShroffDocument13 pagesSeminar: Jonathan D Mizrahi, Rishi Surana, Juan W Valle, Rachna T ShroffNoy FaridaNo ratings yet
- 6#cirrhosisDocument9 pages6#cirrhosishitashiNo ratings yet
- Human C-Reactive Protein and The Metabolic SyndromeDocument13 pagesHuman C-Reactive Protein and The Metabolic SyndromeEmir SaricNo ratings yet
- Diabetes y Relacion Entre Carcinoma HepatocelularDocument7 pagesDiabetes y Relacion Entre Carcinoma HepatocelularAnha Lagos ReyesNo ratings yet
- Diabetes and Cancer: A Consensus ReportDocument12 pagesDiabetes and Cancer: A Consensus ReportDeekay06No ratings yet
- Esophageal Malignancy: A Growing Concern: ISSN 1007-9327 (Print) ISSN 2219-2840 (Online) Doi:10.3748/wjg.v18.i45.6521Document6 pagesEsophageal Malignancy: A Growing Concern: ISSN 1007-9327 (Print) ISSN 2219-2840 (Online) Doi:10.3748/wjg.v18.i45.6521Agus KarsetiyonoNo ratings yet
- Cancer Gastrico Lancet 2020Document14 pagesCancer Gastrico Lancet 2020andreaNo ratings yet
- VITAMINA D y Riesgo CardiovascularDocument12 pagesVITAMINA D y Riesgo CardiovascularAngusNo ratings yet
- Review of Cancer CachexiaDocument46 pagesReview of Cancer CachexiahuwainannisaNo ratings yet
- Gut and Liver NASH Inflammatory DisorderDocument23 pagesGut and Liver NASH Inflammatory Disordershiv_chitturi1295No ratings yet
- Guggenheim 2012Document7 pagesGuggenheim 2012Andreea PodaruNo ratings yet
- Pathology of Fatty Liver DiseaseDocument9 pagesPathology of Fatty Liver DiseaseJeanny LadiNo ratings yet
- Metastasis Site Liver CancerDocument7 pagesMetastasis Site Liver CancerChristofel JomanNo ratings yet
- Incidence and Predictors of All-Cause and Site-Specific Cancer in Type 2 Diabetes: The Fremantle Diabetes StudyDocument11 pagesIncidence and Predictors of All-Cause and Site-Specific Cancer in Type 2 Diabetes: The Fremantle Diabetes StudyKami KamiNo ratings yet
- Histopathology of Hepatocellular CarcinomaDocument11 pagesHistopathology of Hepatocellular CarcinomaCindy Sabina FaleandraNo ratings yet
- Hepato CA 8Document15 pagesHepato CA 8Al VlaovicNo ratings yet
- Non-Alcoholic Fatty Liver Disease - Causes, Diagnosis, Cardiometabolic Consequences, and Treatment StrategiesDocument12 pagesNon-Alcoholic Fatty Liver Disease - Causes, Diagnosis, Cardiometabolic Consequences, and Treatment StrategiesntnquynhproNo ratings yet
- International Incidence and Mortality Trends of Liver Cancer: A Global ProfileDocument9 pagesInternational Incidence and Mortality Trends of Liver Cancer: A Global ProfileNovita ApramadhaNo ratings yet
- Diabetes, Pancreatogenic Diabetes, and Pancreatic CancerDocument8 pagesDiabetes, Pancreatogenic Diabetes, and Pancreatic CancerTeodoraManNo ratings yet
- DM Tipe 2Document5 pagesDM Tipe 2Septian PutraNo ratings yet
- Hepatocellular Carcinoma: The Need For Progress: Ournal of Linical NcologyDocument8 pagesHepatocellular Carcinoma: The Need For Progress: Ournal of Linical NcologyGetty InasNo ratings yet
- NIH Public Access: Epidemiology of HCC: Consider The PopulationDocument10 pagesNIH Public Access: Epidemiology of HCC: Consider The PopulationKe XuNo ratings yet
- Unidad Educativa Bilingüe Steiner Internacional MonographDocument18 pagesUnidad Educativa Bilingüe Steiner Internacional MonographAndre KangNo ratings yet
- Vitamin DDocument12 pagesVitamin DLia NadaNo ratings yet
- Hepatocellular CarcinomaDocument2 pagesHepatocellular CarcinomaDaniel Moreira CarreiraNo ratings yet
- Cancers 07 00883Document22 pagesCancers 07 00883julia.linsNo ratings yet
- The Gastroenterologist's Guide To Preventive Management of Compensated CirrhosisDocument8 pagesThe Gastroenterologist's Guide To Preventive Management of Compensated CirrhosisjihanvrpNo ratings yet
- Journal IJC STLH EditDocument6 pagesJournal IJC STLH EditTuti WardaniNo ratings yet
- 3 Lastra Et Al., 2014 Review - Type 2 Diabetes Mellitus and Hypertension An UpdateDocument20 pages3 Lastra Et Al., 2014 Review - Type 2 Diabetes Mellitus and Hypertension An Updatebangd1f4nNo ratings yet
- Jounal Gizi2 AJCNDocument8 pagesJounal Gizi2 AJCNperiNo ratings yet
- Biomolecules 11 01022Document25 pagesBiomolecules 11 01022meliaaammeNo ratings yet
- Etiology of Pancreatic CancerDocument3 pagesEtiology of Pancreatic CancerHananya ManroeNo ratings yet
- The Effect of Ketogenic Diet On Shared Risk Factors of Cardiovascular Disease and CancerDocument22 pagesThe Effect of Ketogenic Diet On Shared Risk Factors of Cardiovascular Disease and CancerCierra NolenNo ratings yet
- Published PaperDocument10 pagesPublished Papermohd aftab siddiquiNo ratings yet
- Prevalence and Associated Risk Factors of Dyslipidemia Among Type Two Diabetic Patients Attending Tiko Cottage HospitalDocument12 pagesPrevalence and Associated Risk Factors of Dyslipidemia Among Type Two Diabetic Patients Attending Tiko Cottage HospitalEditor IJTSRDNo ratings yet
- Gastric CancerDocument100 pagesGastric CancerJunior Más FlowNo ratings yet
- Diabetes, Glucose Level, and Risk of Sudden Cardiac DeathDocument6 pagesDiabetes, Glucose Level, and Risk of Sudden Cardiac DeathDino DanielNo ratings yet
- Dental Hygiene Resume - No ReferencesDocument2 pagesDental Hygiene Resume - No Referencesapi-313829416No ratings yet
- Endorsement FormDocument12 pagesEndorsement Formferraterkimdaniel25No ratings yet
- Protocolo de EscritaDocument5 pagesProtocolo de EscritaGabriela Ruggiero NorNo ratings yet
- Helloyubo Com Chatbot Benefits of Using A Whatsapp Healthcare ChatbotDocument4 pagesHelloyubo Com Chatbot Benefits of Using A Whatsapp Healthcare ChatbotSubrahmanyeswari DeviNo ratings yet
- Electronic Health (E-Health) : Emerging Role in Asthma: ReviewDocument6 pagesElectronic Health (E-Health) : Emerging Role in Asthma: ReviewVirgo WNo ratings yet
- Nursing Care Plan: Cues Nursing Diagnosis Objective Intervention Rationale EvaluationDocument2 pagesNursing Care Plan: Cues Nursing Diagnosis Objective Intervention Rationale Evaluationmyer pasandalanNo ratings yet
- PGH 101 v2018Document10 pagesPGH 101 v2018Ian Phillip PaclibareNo ratings yet
- Family Nursing Care PlanDocument4 pagesFamily Nursing Care PlanSyvNo ratings yet
- Sharpening The Equity Focus: Selected Innovations and Lessons Learned From UNICEF-assisted Programmes 2009-2010Document80 pagesSharpening The Equity Focus: Selected Innovations and Lessons Learned From UNICEF-assisted Programmes 2009-2010UNICEFNo ratings yet
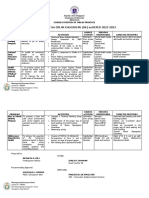
- Action Plan For Oplan Kalusugan Ok Sa Deped 2022Document2 pagesAction Plan For Oplan Kalusugan Ok Sa Deped 2022Emily Patìo100% (1)
- Apa AjaDocument129 pagesApa AjaRoyNo ratings yet
- OSHA Recordkeeping - Comprehensive PresentationDocument73 pagesOSHA Recordkeeping - Comprehensive Presentationjcs223No ratings yet
- Introduction To Hospital Pharmacy: OutlineDocument12 pagesIntroduction To Hospital Pharmacy: OutlinePrincess TiongsonNo ratings yet
- Gensco Pharma's Transdermal Colchicine, ColciGel®, For Treatment of Acute Gout Flares With Negligible Systemic Absorption Improving Tolerability With Less Side EffectsDocument3 pagesGensco Pharma's Transdermal Colchicine, ColciGel®, For Treatment of Acute Gout Flares With Negligible Systemic Absorption Improving Tolerability With Less Side EffectsPR.comNo ratings yet
- Diabetic 1Document1 pageDiabetic 1Vamsee KrishnaNo ratings yet
- Biostatistics For CK Step 2 6.16.2019Document37 pagesBiostatistics For CK Step 2 6.16.2019karan kauraNo ratings yet
- Protected Health InformationDocument4 pagesProtected Health Informationpurity NgasiNo ratings yet
- Ageing Population Geography Case StudyDocument3 pagesAgeing Population Geography Case StudynosheenNo ratings yet
- Ourse Yllabus Section I - College and University Catalog DataDocument5 pagesOurse Yllabus Section I - College and University Catalog DatabagusNo ratings yet
- An Historical Perspective On Principles of Osteopathy - Jane Eliza Stark. 2013Document8 pagesAn Historical Perspective On Principles of Osteopathy - Jane Eliza Stark. 2013Adolfo Esteban Soto MartinezNo ratings yet
- Topcom Vi Tentative ProgramDocument6 pagesTopcom Vi Tentative ProgramLim Jun BinNo ratings yet
- Sonnykalangi,+13 +ok+ (13) +sudarman+68-80Document21 pagesSonnykalangi,+13 +ok+ (13) +sudarman+68-80Nandini Permata SariNo ratings yet
- JKCD 6Document5 pagesJKCD 6sulistyowati_rnNo ratings yet
- Hydrotherapy NotesDocument15 pagesHydrotherapy NotesKeerthana RaviNo ratings yet
- Hydro DemolitionDocument1 pageHydro DemolitionAgnes BNo ratings yet
- Video-Lesson-Script - Q4M4Document7 pagesVideo-Lesson-Script - Q4M4Rona RuizNo ratings yet
- Rle - NCM 109 Sample OnlyDocument3 pagesRle - NCM 109 Sample OnlyFaine Angela CaonesNo ratings yet
- Exam Semi23423123132Document2 pagesExam Semi23423123132gwapoNo ratings yet
- Past, Present, and Future of Antibacterial Economics: Increasing Bacterial Resistance, Limited Antibiotic Pipeline, and Societal ImplicationsDocument14 pagesPast, Present, and Future of Antibacterial Economics: Increasing Bacterial Resistance, Limited Antibiotic Pipeline, and Societal ImplicationsLeonardo SimonciniNo ratings yet