Download as pdf or txt
You might also like
- ACLS Pocket CardDocument6 pagesACLS Pocket Cardno_spam_mang83% (6)
- Precision Nutrition Coaching WorkbookDocument165 pagesPrecision Nutrition Coaching WorkbookJože Majcen86% (7)
- Pediatric Mock Resuscitation ScenariosDocument6 pagesPediatric Mock Resuscitation ScenariosdinkytinkNo ratings yet
- Acls Cheat Sheet PDFDocument3 pagesAcls Cheat Sheet PDFDarren Dawkins100% (4)
- CPR PPT FinalDocument83 pagesCPR PPT FinalSimran Josan100% (3)
- 23 Mock CodesDocument56 pages23 Mock Codesmaguisssa100% (4)
- BloApCo Fan Model 40-2, Serial Number 150089B Fan ManualDocument25 pagesBloApCo Fan Model 40-2, Serial Number 150089B Fan ManualAnderson AlmeidaNo ratings yet
- AlgorithmACLS CA COVID LNGDSCRP 220203Document3 pagesAlgorithmACLS CA COVID LNGDSCRP 220203AndhikaNo ratings yet
- Paediatric Advanced Life Support: Resuscitation Council (UK)Document12 pagesPaediatric Advanced Life Support: Resuscitation Council (UK)zacklim_2000100% (1)
- ECSI CAAlgorithm PDFDocument2 pagesECSI CAAlgorithm PDFCarlos ChiNo ratings yet
- A (ACLS) - 2015: Dvanced Cardiac Life SupportDocument52 pagesA (ACLS) - 2015: Dvanced Cardiac Life SupportNajmussaqibNo ratings yet
- Saudi CPR Guidlines in EnglishDocument16 pagesSaudi CPR Guidlines in EnglishpiyushbamsNo ratings yet
- AlgorithmBLS Ped Single Rescuer LNGDSCRP 200831 EdDocument2 pagesAlgorithmBLS Ped Single Rescuer LNGDSCRP 200831 EdmangoolegooshNo ratings yet
- Paediatric Clinical GuidelinesDocument7 pagesPaediatric Clinical GuidelinesAndriNo ratings yet
- CPR Class QuestionnaireDocument4 pagesCPR Class QuestionnaireParikshit PekhaleNo ratings yet
- Basic Life Support (BLS) and Advanced Cardiovascular Life Support (ACLS)Document35 pagesBasic Life Support (BLS) and Advanced Cardiovascular Life Support (ACLS)rajNo ratings yet
- ACLS - Guidelines From 2005USADocument62 pagesACLS - Guidelines From 2005USAsbontchevNo ratings yet
- AlgorithmBLS Adult LNGDSCRP 200702 EdDocument1 pageAlgorithmBLS Adult LNGDSCRP 200702 EdAnshika yadavNo ratings yet
- Advanced Cardiac Life SupportDocument42 pagesAdvanced Cardiac Life SupportDennis MiritiNo ratings yet
- Adult Advanced Life Support2Document34 pagesAdult Advanced Life Support2drDilanNo ratings yet
- ACLS Algorithms (2011)Document6 pagesACLS Algorithms (2011)senbonsakuraNo ratings yet
- AlgorithmDocument25 pagesAlgorithmQayNo ratings yet
- Cardiopulmonary ResuscitationDocument29 pagesCardiopulmonary ResuscitationSarahNo ratings yet
- Advanced Cardiac Life Support Information From American Heart Association, Advanced Cardiac Life Support, 2006Document25 pagesAdvanced Cardiac Life Support Information From American Heart Association, Advanced Cardiac Life Support, 2006karento1No ratings yet
- Basic Life SupportDocument6 pagesBasic Life SupportbhongskirnNo ratings yet
- Advanced Cardiac Life Support (ACLS)Document17 pagesAdvanced Cardiac Life Support (ACLS)Siti Rahima HarahapNo ratings yet
- 3 Combined AHA BLS ACLS Updates CombinedDocument5 pages3 Combined AHA BLS ACLS Updates Combinedamanrup randhawa100% (1)
- Dvanced Ardiovascular Ife Upport: A C L SDocument10 pagesDvanced Ardiovascular Ife Upport: A C L SErica Jane100% (1)
- Cesarean SectionDocument34 pagesCesarean SectionAboubakar Moalim Mahad moh'dNo ratings yet
- Advanced Cardiac Life SupportDocument8 pagesAdvanced Cardiac Life Supportcool kipsNo ratings yet
- NEONNATALDocument15 pagesNEONNATALOsama HussainNo ratings yet
- Neonatal ResuscitationDocument5 pagesNeonatal Resuscitationapi-3712326No ratings yet
- Algoritm Trat Algoritm Tratament Astm Bronsic - Pdfament Astm BronsicDocument1 pageAlgoritm Trat Algoritm Tratament Astm Bronsic - Pdfament Astm BronsicSbarcea AurelNo ratings yet
- American Heart Association: Precourse Written Examination May 2001Document10 pagesAmerican Heart Association: Precourse Written Examination May 2001Ericka SwordNo ratings yet
- Pediatric Life Support SHGDocument32 pagesPediatric Life Support SHGIwan SinagaNo ratings yet
- Pediatric Emergency Summary For Osce ExamDocument84 pagesPediatric Emergency Summary For Osce ExamAlwaallh Mohammed100% (1)
- ATLSDocument34 pagesATLSalice DillerudNo ratings yet
- Pediatric Protokol EmergencyDocument19 pagesPediatric Protokol EmergencyChristian RobbyNo ratings yet
- Pediatric Notes 2Document25 pagesPediatric Notes 2luke markNo ratings yet
- Should Be Available at All Sites If Feasible, Include at Sites (Not Required)Document5 pagesShould Be Available at All Sites If Feasible, Include at Sites (Not Required)Ahmed QlhamdNo ratings yet
- PALS Pre StudyDocument28 pagesPALS Pre Studynursesed100% (7)
- Neonatal ResuscitationDocument17 pagesNeonatal ResuscitationKookia BatoromaioNo ratings yet
- BLS and ACLS SurveysDocument29 pagesBLS and ACLS SurveysMosab AfanahNo ratings yet
- Pulseless Arrest Algorithm For Managing VF and Pulseless VTDocument3 pagesPulseless Arrest Algorithm For Managing VF and Pulseless VTLaili CinthiaNo ratings yet
- VF PediDocument6 pagesVF PedixiphoideusNo ratings yet
- ASCIA Guidelines Acute Management Anaphylaxis 2017 Updated PDFDocument8 pagesASCIA Guidelines Acute Management Anaphylaxis 2017 Updated PDFAyu WahyuniNo ratings yet
- Advanced Life SupportDocument65 pagesAdvanced Life SupportPrasad Narangoda100% (1)
- Code Blue PolicyDocument3 pagesCode Blue Policydr.eyad.m.m.mNo ratings yet
- Intubation ChecklistDocument2 pagesIntubation ChecklistDaniel CrookNo ratings yet
- Acls Study GuideDocument3 pagesAcls Study Guideemacc250No ratings yet
- ACLS PEA Asystole AlgorithmDocument3 pagesACLS PEA Asystole AlgorithmSafira RNo ratings yet
- Bls - Fbao - First AidDocument172 pagesBls - Fbao - First AidMaria Regina Castro Gabriel100% (1)
- Hersheychapter 1Document17 pagesHersheychapter 1poddata100% (1)
- NRP - Lesson 7 MedicationsDocument31 pagesNRP - Lesson 7 MedicationsShariti DeviNo ratings yet
- Ped - ER Lec 2 Ver1Document18 pagesPed - ER Lec 2 Ver1Priyadharsini RajNo ratings yet
- Induced HPDocument4 pagesInduced HPmaddythedocNo ratings yet
- Pediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandPediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesRating: 5 out of 5 stars5/5 (2)
- Advanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandAdvanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesRating: 4 out of 5 stars4/5 (6)
- First Aid & Emergency Companions: First Aid & Emergencies at SeaFrom EverandFirst Aid & Emergency Companions: First Aid & Emergencies at SeaNo ratings yet
- Dimensional Analysis For Nursing StudentsFrom EverandDimensional Analysis For Nursing StudentsNo ratings yet
- Raguindin, Maricel B. (S.W 103 Assignment)Document10 pagesRaguindin, Maricel B. (S.W 103 Assignment)Maricel RaguindinNo ratings yet
- Keeping Food Safe PresentationDocument13 pagesKeeping Food Safe Presentationapi-515993598No ratings yet
- AHA Vs ERC GuidelinesDocument39 pagesAHA Vs ERC GuidelinesYoel Harianto100% (2)
- Esmeril de Banco Metabo DS-200Document24 pagesEsmeril de Banco Metabo DS-200rctallerelectricoNo ratings yet
- Fixed ProsthodonticsDocument21 pagesFixed ProsthodonticsnseraldenNo ratings yet
- My Learning Experience at Lung Center of The: PhilippinesDocument3 pagesMy Learning Experience at Lung Center of The: PhilippinesMarie Aurora Gielbert MarianoNo ratings yet
- Justice and Solicitor General Letter To Edmonton Mayor Public Safety 2022-05-26Document3 pagesJustice and Solicitor General Letter To Edmonton Mayor Public Safety 2022-05-26edmontonjournalNo ratings yet
- Dr. Djohan Ardiansyah, SP.S (K)Document60 pagesDr. Djohan Ardiansyah, SP.S (K)satyagraha84No ratings yet
- 025c082733ea2-CLAT POST AprilDocument47 pages025c082733ea2-CLAT POST AprilHarsh SrivastavaNo ratings yet
- Drugs Used in The Treatment of CoughDocument12 pagesDrugs Used in The Treatment of CoughMaryam NisaNo ratings yet
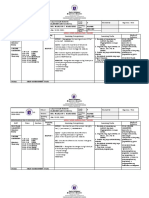
- Whlp-Mapeh (2ND Quarter)Document10 pagesWhlp-Mapeh (2ND Quarter)MARLON MARTINEZNo ratings yet
- Full Mouth Rehabilitation of A Patient With Ra PDFDocument3 pagesFull Mouth Rehabilitation of A Patient With Ra PDFdehaaNo ratings yet
- Radial Nerve InjuryDocument5 pagesRadial Nerve InjuryMuhammad RezaNo ratings yet
- Health DaysDocument2 pagesHealth DaysAkshata GojeNo ratings yet
- Mind, Character and Personality Volume 2Document353 pagesMind, Character and Personality Volume 23angelsminconcepts100% (2)
- Research Paper On Dengue Fever in PakistanDocument6 pagesResearch Paper On Dengue Fever in Pakistangvzz4v44100% (1)
- Case Control Study DesignDocument15 pagesCase Control Study Designgeorgeloto12No ratings yet
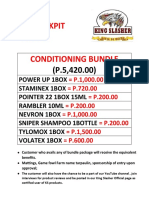
- Texas Cockpit Arena Conditioning BundleDocument4 pagesTexas Cockpit Arena Conditioning BundleHanna Sobreviñas AmanteNo ratings yet
- Asian Medical SystemsDocument12 pagesAsian Medical SystemsReggie ThorpeNo ratings yet
- Practical Application of CPAP: Dr. Srinivas MurkiDocument8 pagesPractical Application of CPAP: Dr. Srinivas MurkiRaji MohanNo ratings yet
- Change The Story SummaryDocument2 pagesChange The Story SummaryEmmaNo ratings yet
- Motor Development in Children With Autism SpectrumDocument7 pagesMotor Development in Children With Autism SpectrumFlávia AquinoNo ratings yet
- MEDICAL IMAGING Updated 2022Document25 pagesMEDICAL IMAGING Updated 2022Mengot Ashu RoseNo ratings yet
- Health Buddy: Our VisionDocument7 pagesHealth Buddy: Our VisionMoidin AfsanNo ratings yet
- English ProjectDocument17 pagesEnglish ProjectPreeti TiwariNo ratings yet
- Establish Quality StandardsTTLMDocument15 pagesEstablish Quality StandardsTTLMwendi mesele100% (3)
- Q1 Tle 9 Eim TosDocument2 pagesQ1 Tle 9 Eim TosjuzielouNo ratings yet
- Project Feasibility Study and Evaluation 2011 Sports ComplexDocument264 pagesProject Feasibility Study and Evaluation 2011 Sports ComplexFongbeerNo ratings yet