
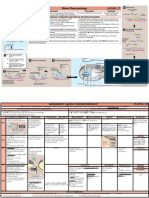
Arrhythmias (II) : Treatment: 1-Nonpharmacologic Therapy of Bradyarrhythmias: Cardiac Pacemakers
Arrhythmias (II) : Treatment: 1-Nonpharmacologic Therapy of Bradyarrhythmias: Cardiac Pacemakers
You might also like
- Dick Quinn - Left For Dead - Cayenne Pepper-R F Quinn Pub Co (1991)Document212 pagesDick Quinn - Left For Dead - Cayenne Pepper-R F Quinn Pub Co (1991)Gleb Pogaday100% (1)
- NP 3Document20 pagesNP 3MENARDNo ratings yet
- Handbook of AnesthesiologyDocument176 pagesHandbook of AnesthesiologyarmelzahfauziNo ratings yet
- WarfarinDocument23 pagesWarfarinminaNo ratings yet
- PALS Pamphlet Edited PDFDocument4 pagesPALS Pamphlet Edited PDFsaleem50% (4)
- Guidelines: Peri-Arrest Arrhythmias: Guidelines Development Process ManualDocument15 pagesGuidelines: Peri-Arrest Arrhythmias: Guidelines Development Process ManualParvathy R NairNo ratings yet
- Peri-Arrest Arrhythmias: AuthorsDocument11 pagesPeri-Arrest Arrhythmias: AuthorsMohammadAbdurRahmanNo ratings yet
- PPP305 LA10 08052024 ArrhythmiaDocument37 pagesPPP305 LA10 08052024 Arrhythmiagadk555No ratings yet
- Prehospital Care: Immediate Interventions - AbcsDocument8 pagesPrehospital Care: Immediate Interventions - AbcsindahkurNo ratings yet
- Nhip Tim NhanhDocument3 pagesNhip Tim NhanhHiếu KiềuNo ratings yet
- Atrial Fibrillation 2022Document29 pagesAtrial Fibrillation 2022daniel mitikuNo ratings yet
- Cardioversion For Atrial Fibrillation - ClinicalKeyDocument27 pagesCardioversion For Atrial Fibrillation - ClinicalKeyAnthony Martin Corrales ParedesNo ratings yet
- Af NoteDocument6 pagesAf NoteMohammed SadoonNo ratings yet
- Arrhythimas 6Document38 pagesArrhythimas 6غفران هيثم خليلNo ratings yet
- Advanced Cardiovascular Life Support in Adults (ACLS) : SubtitleDocument30 pagesAdvanced Cardiovascular Life Support in Adults (ACLS) : SubtitleMohamad El SharNo ratings yet
- Intensive Care Unit Arrhythmias: S.M. HollenbergDocument13 pagesIntensive Care Unit Arrhythmias: S.M. HollenbergEvita FebriyantiNo ratings yet
- Current Clinical Strategies: Handbook of AnesthesiologyDocument180 pagesCurrent Clinical Strategies: Handbook of AnesthesiologydramaganaNo ratings yet
- Ischemic Stroke ManagementDocument8 pagesIschemic Stroke ManagementBa LitNo ratings yet
- Atrial FibrillationDocument2 pagesAtrial Fibrillationrxmskdkd33No ratings yet
- Management of Symptomatic Bradycardia and TachycardiaDocument55 pagesManagement of Symptomatic Bradycardia and TachycardiaDewintha Airene NoviantiNo ratings yet
- Managing Atrial Fibrillation 2015Document8 pagesManaging Atrial Fibrillation 2015Mayra Alejandra Prada SerranoNo ratings yet
- Acute Heart FailureDocument24 pagesAcute Heart FailureTeddy MauriceNo ratings yet
- Summary of 2016 Esc Guidelines On Heart Failure, Atrial Fibrillation, Dyslipidaemia and Cardiovascular PreventionDocument11 pagesSummary of 2016 Esc Guidelines On Heart Failure, Atrial Fibrillation, Dyslipidaemia and Cardiovascular PreventionNick StamatiadisNo ratings yet
- Guidelines For The Management of Atrial Fibrillation Part-IIDocument66 pagesGuidelines For The Management of Atrial Fibrillation Part-IIJamil Muqtadir BhattiNo ratings yet
- Supraventricular Tachycardia (SVT)Document2 pagesSupraventricular Tachycardia (SVT)Balayet HossenNo ratings yet
- Ventricular TachycardiaDocument17 pagesVentricular TachycardiaAyu Rezki FadliyaNo ratings yet
- Life Threatening Arrhythmia and ManagementDocument40 pagesLife Threatening Arrhythmia and ManagementRuki Hartawan100% (1)
- Emergency Drug Therapy 1ceuDocument7 pagesEmergency Drug Therapy 1ceuRN333No ratings yet
- Guidelines For The Management of Acute Stroke: Emergency DepartmentDocument10 pagesGuidelines For The Management of Acute Stroke: Emergency DepartmentUhuebor DavidNo ratings yet
- Anaesthesia For TURPDocument6 pagesAnaesthesia For TURPMutia FarinaNo ratings yet
- Atrial FibrillationDocument8 pagesAtrial FibrillationduhsknwsNo ratings yet
- FA Rate ControlDocument29 pagesFA Rate Controlchecos.boy88No ratings yet
- Acs 11 190524110746Document46 pagesAcs 11 190524110746Obakeng MandaNo ratings yet
- The Emergency ManagementDocument12 pagesThe Emergency ManagementWidya Surya AvantiNo ratings yet
- Management of Atrial Fibrillation CNA 2015Document14 pagesManagement of Atrial Fibrillation CNA 2015isaNo ratings yet
- Treatment of FLASH Pulm Edema & ADHF in ACS - UpToDateDocument10 pagesTreatment of FLASH Pulm Edema & ADHF in ACS - UpToDateansylaeNo ratings yet
- Cardio BBDocument73 pagesCardio BBايات عبدالرحمنNo ratings yet
- Guideline 11 9 Managing Acute Dysrhythmias 307Document10 pagesGuideline 11 9 Managing Acute Dysrhythmias 307gregraynerNo ratings yet
- Farmakologi Anti AritmiaDocument26 pagesFarmakologi Anti AritmiaAzzam nur TaufikurrahmanNo ratings yet
- 3390-Article Text-1555-3802-10-20200606Document12 pages3390-Article Text-1555-3802-10-20200606Mayara Bongestab ParteliNo ratings yet
- PerfusionDocument10 pagesPerfusionHaja Sherief100% (1)
- AF KardiomiopatiDocument5 pagesAF KardiomiopatiannisNo ratings yet
- Acute Heart Failure Diagnosing and Managing Acute Heart Failure in Adults.Document21 pagesAcute Heart Failure Diagnosing and Managing Acute Heart Failure in Adults.Madalina TalpauNo ratings yet
- AVJ Ablation Vs CardioversionDocument6 pagesAVJ Ablation Vs CardioversionAndy CordekNo ratings yet
- Aha Guidelines StemiDocument94 pagesAha Guidelines StemiDika DekokNo ratings yet
- Arrhythmia Management For The Primary Care Clinician - UpToDateDocument33 pagesArrhythmia Management For The Primary Care Clinician - UpToDateMelanny Perez GonzalesNo ratings yet
- QRG AntithromboticDocument6 pagesQRG AntithromboticthapanNo ratings yet
- Stroke Anti CoagulationDocument26 pagesStroke Anti CoagulationdoctormussieaberraNo ratings yet
- Treatment Approach Considerations: Pericardial SclerosisDocument7 pagesTreatment Approach Considerations: Pericardial SclerosisDikie MustofadijayaNo ratings yet
- CCS - Handbook of Anesthesiology (2005)Document180 pagesCCS - Handbook of Anesthesiology (2005)Rojelle LezamaNo ratings yet
- ACLS Advanced Cardiovascular Life Support Provider Manual 2023From EverandACLS Advanced Cardiovascular Life Support Provider Manual 2023No ratings yet
- Critical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsNo ratings yet
- Critical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsNo ratings yet
- Pacemaker Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPacemaker Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Antiarrhythmic DrugsFrom EverandAntiarrhythmic DrugsAntoni Martínez-RubioNo ratings yet
- Arrhythmia Induction in the EP LabFrom EverandArrhythmia Induction in the EP LabGabriel CismaruNo ratings yet
- Case-Based Device Therapy for Heart FailureFrom EverandCase-Based Device Therapy for Heart FailureUlrika Birgersdotter-GreenNo ratings yet
- Atrial Fibrillation A Simple Guide to The Condition, Treatment And Related DiseasesFrom EverandAtrial Fibrillation A Simple Guide to The Condition, Treatment And Related DiseasesRating: 4 out of 5 stars4/5 (1)
- Alcain CPRDocument6 pagesAlcain CPRErika Trina AlcainNo ratings yet
- A Drug Study On: Furosemide TabletDocument7 pagesA Drug Study On: Furosemide TabletRaijenne VersolaNo ratings yet
- Cardiac ArrhythmiasDocument9 pagesCardiac ArrhythmiasRemelou Garchitorena AlfelorNo ratings yet
- NCP Impaired Gas Exchange STROKEDocument2 pagesNCP Impaired Gas Exchange STROKEMa. Elaine Carla TatingNo ratings yet
- Necrotizing Enterocolitis (Sultn Aiman NeazyDocument59 pagesNecrotizing Enterocolitis (Sultn Aiman NeazyMohammed ElhashimiNo ratings yet
- Perspective in Centre For Pharmaceutical Sciences (CPS), Institute of Science and Technology (IST)Document3 pagesPerspective in Centre For Pharmaceutical Sciences (CPS), Institute of Science and Technology (IST)Ardiene Shallouvette GamosoNo ratings yet
- Comparative Rates of Conduction System FiringDocument3 pagesComparative Rates of Conduction System FiringSulochana ChanNo ratings yet
- Internal Medicine Case Studies BMHDocument4 pagesInternal Medicine Case Studies BMHParsaant SinghNo ratings yet
- 7 The Meninges, CSFDocument22 pages7 The Meninges, CSFDavid KleinNo ratings yet
- DefibrillatorDocument85 pagesDefibrillatorDhruv DesaiNo ratings yet
- Assessing Vital Signs HandoutsDocument9 pagesAssessing Vital Signs Handoutsyhudz100% (3)
- Drug-StudyDocument1 pageDrug-StudyMhica PrestozaNo ratings yet
- Stress-Induced (Takotsubo) CardiomyopathyDocument13 pagesStress-Induced (Takotsubo) CardiomyopathyAdrian GeambasuNo ratings yet
- March 2023 Recalls Solved by Nazia RafiqueDocument18 pagesMarch 2023 Recalls Solved by Nazia RafiqueelgafarypharmacyNo ratings yet
- Hema Poikilocytosis StatPearls NCBI BookshelfDocument10 pagesHema Poikilocytosis StatPearls NCBI BookshelfVincent ReyesNo ratings yet
- Aortic RegurgitationDocument7 pagesAortic RegurgitationazaliavirsaNo ratings yet
- Zoology II (Em) BLM 21-22Document99 pagesZoology II (Em) BLM 21-22GANESH KANDAGATLANo ratings yet
- CTA CoronaryDocument39 pagesCTA CoronaryConsita VictoriaNo ratings yet
- Kaya ChikitsaDocument37 pagesKaya ChikitsaGAURAV100% (1)
- How To Take HistoryDocument59 pagesHow To Take HistoryBelalNo ratings yet
- Purpose of Emergency DrugsDocument8 pagesPurpose of Emergency DrugsShehnaz SheikhNo ratings yet
- HeartIndia54157-4958724 134627 PDFDocument3 pagesHeartIndia54157-4958724 134627 PDFGagandeep Singh ShergillNo ratings yet
- Health Assessment Lecture: - Review About THE Respiratory SystemDocument8 pagesHealth Assessment Lecture: - Review About THE Respiratory SystemHNo ratings yet
- AtherosclerosisDocument7 pagesAtherosclerosisFaris Mufid Madyaputra100% (1)
- Haversian System (Osteon) : Basic Structural UnitDocument7 pagesHaversian System (Osteon) : Basic Structural UnitJulius Matthew MarananNo ratings yet
- S-Bridging The Gap in Asthma Management (In-11244)Document34 pagesS-Bridging The Gap in Asthma Management (In-11244)w5bwmbfrtwNo ratings yet
- Blood Pharmacology 27-34Document8 pagesBlood Pharmacology 27-34ahmedsalah565vvvNo ratings yet

























































































Download as pdf or txt
You might also like
- Dick Quinn - Left For Dead - Cayenne Pepper-R F Quinn Pub Co (1991)Document212 pagesDick Quinn - Left For Dead - Cayenne Pepper-R F Quinn Pub Co (1991)Gleb Pogaday100% (1)
- NP 3Document20 pagesNP 3MENARDNo ratings yet
- Handbook of AnesthesiologyDocument176 pagesHandbook of AnesthesiologyarmelzahfauziNo ratings yet
- WarfarinDocument23 pagesWarfarinminaNo ratings yet
- PALS Pamphlet Edited PDFDocument4 pagesPALS Pamphlet Edited PDFsaleem50% (4)
- Guidelines: Peri-Arrest Arrhythmias: Guidelines Development Process ManualDocument15 pagesGuidelines: Peri-Arrest Arrhythmias: Guidelines Development Process ManualParvathy R NairNo ratings yet
- Peri-Arrest Arrhythmias: AuthorsDocument11 pagesPeri-Arrest Arrhythmias: AuthorsMohammadAbdurRahmanNo ratings yet
- PPP305 LA10 08052024 ArrhythmiaDocument37 pagesPPP305 LA10 08052024 Arrhythmiagadk555No ratings yet
- Prehospital Care: Immediate Interventions - AbcsDocument8 pagesPrehospital Care: Immediate Interventions - AbcsindahkurNo ratings yet
- Nhip Tim NhanhDocument3 pagesNhip Tim NhanhHiếu KiềuNo ratings yet
- Atrial Fibrillation 2022Document29 pagesAtrial Fibrillation 2022daniel mitikuNo ratings yet
- Cardioversion For Atrial Fibrillation - ClinicalKeyDocument27 pagesCardioversion For Atrial Fibrillation - ClinicalKeyAnthony Martin Corrales ParedesNo ratings yet
- Af NoteDocument6 pagesAf NoteMohammed SadoonNo ratings yet
- Arrhythimas 6Document38 pagesArrhythimas 6غفران هيثم خليلNo ratings yet
- Advanced Cardiovascular Life Support in Adults (ACLS) : SubtitleDocument30 pagesAdvanced Cardiovascular Life Support in Adults (ACLS) : SubtitleMohamad El SharNo ratings yet
- Intensive Care Unit Arrhythmias: S.M. HollenbergDocument13 pagesIntensive Care Unit Arrhythmias: S.M. HollenbergEvita FebriyantiNo ratings yet
- Current Clinical Strategies: Handbook of AnesthesiologyDocument180 pagesCurrent Clinical Strategies: Handbook of AnesthesiologydramaganaNo ratings yet
- Ischemic Stroke ManagementDocument8 pagesIschemic Stroke ManagementBa LitNo ratings yet
- Atrial FibrillationDocument2 pagesAtrial Fibrillationrxmskdkd33No ratings yet
- Management of Symptomatic Bradycardia and TachycardiaDocument55 pagesManagement of Symptomatic Bradycardia and TachycardiaDewintha Airene NoviantiNo ratings yet
- Managing Atrial Fibrillation 2015Document8 pagesManaging Atrial Fibrillation 2015Mayra Alejandra Prada SerranoNo ratings yet
- Acute Heart FailureDocument24 pagesAcute Heart FailureTeddy MauriceNo ratings yet
- Summary of 2016 Esc Guidelines On Heart Failure, Atrial Fibrillation, Dyslipidaemia and Cardiovascular PreventionDocument11 pagesSummary of 2016 Esc Guidelines On Heart Failure, Atrial Fibrillation, Dyslipidaemia and Cardiovascular PreventionNick StamatiadisNo ratings yet
- Guidelines For The Management of Atrial Fibrillation Part-IIDocument66 pagesGuidelines For The Management of Atrial Fibrillation Part-IIJamil Muqtadir BhattiNo ratings yet
- Supraventricular Tachycardia (SVT)Document2 pagesSupraventricular Tachycardia (SVT)Balayet HossenNo ratings yet
- Ventricular TachycardiaDocument17 pagesVentricular TachycardiaAyu Rezki FadliyaNo ratings yet
- Life Threatening Arrhythmia and ManagementDocument40 pagesLife Threatening Arrhythmia and ManagementRuki Hartawan100% (1)
- Emergency Drug Therapy 1ceuDocument7 pagesEmergency Drug Therapy 1ceuRN333No ratings yet
- Guidelines For The Management of Acute Stroke: Emergency DepartmentDocument10 pagesGuidelines For The Management of Acute Stroke: Emergency DepartmentUhuebor DavidNo ratings yet
- Anaesthesia For TURPDocument6 pagesAnaesthesia For TURPMutia FarinaNo ratings yet
- Atrial FibrillationDocument8 pagesAtrial FibrillationduhsknwsNo ratings yet
- FA Rate ControlDocument29 pagesFA Rate Controlchecos.boy88No ratings yet
- Acs 11 190524110746Document46 pagesAcs 11 190524110746Obakeng MandaNo ratings yet
- The Emergency ManagementDocument12 pagesThe Emergency ManagementWidya Surya AvantiNo ratings yet
- Management of Atrial Fibrillation CNA 2015Document14 pagesManagement of Atrial Fibrillation CNA 2015isaNo ratings yet
- Treatment of FLASH Pulm Edema & ADHF in ACS - UpToDateDocument10 pagesTreatment of FLASH Pulm Edema & ADHF in ACS - UpToDateansylaeNo ratings yet
- Cardio BBDocument73 pagesCardio BBايات عبدالرحمنNo ratings yet
- Guideline 11 9 Managing Acute Dysrhythmias 307Document10 pagesGuideline 11 9 Managing Acute Dysrhythmias 307gregraynerNo ratings yet
- Farmakologi Anti AritmiaDocument26 pagesFarmakologi Anti AritmiaAzzam nur TaufikurrahmanNo ratings yet
- 3390-Article Text-1555-3802-10-20200606Document12 pages3390-Article Text-1555-3802-10-20200606Mayara Bongestab ParteliNo ratings yet
- PerfusionDocument10 pagesPerfusionHaja Sherief100% (1)
- AF KardiomiopatiDocument5 pagesAF KardiomiopatiannisNo ratings yet
- Acute Heart Failure Diagnosing and Managing Acute Heart Failure in Adults.Document21 pagesAcute Heart Failure Diagnosing and Managing Acute Heart Failure in Adults.Madalina TalpauNo ratings yet
- AVJ Ablation Vs CardioversionDocument6 pagesAVJ Ablation Vs CardioversionAndy CordekNo ratings yet
- Aha Guidelines StemiDocument94 pagesAha Guidelines StemiDika DekokNo ratings yet
- Arrhythmia Management For The Primary Care Clinician - UpToDateDocument33 pagesArrhythmia Management For The Primary Care Clinician - UpToDateMelanny Perez GonzalesNo ratings yet
- QRG AntithromboticDocument6 pagesQRG AntithromboticthapanNo ratings yet
- Stroke Anti CoagulationDocument26 pagesStroke Anti CoagulationdoctormussieaberraNo ratings yet
- Treatment Approach Considerations: Pericardial SclerosisDocument7 pagesTreatment Approach Considerations: Pericardial SclerosisDikie MustofadijayaNo ratings yet
- CCS - Handbook of Anesthesiology (2005)Document180 pagesCCS - Handbook of Anesthesiology (2005)Rojelle LezamaNo ratings yet
- ACLS Advanced Cardiovascular Life Support Provider Manual 2023From EverandACLS Advanced Cardiovascular Life Support Provider Manual 2023No ratings yet
- Critical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsNo ratings yet
- Critical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsNo ratings yet
- Pacemaker Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPacemaker Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Antiarrhythmic DrugsFrom EverandAntiarrhythmic DrugsAntoni Martínez-RubioNo ratings yet
- Arrhythmia Induction in the EP LabFrom EverandArrhythmia Induction in the EP LabGabriel CismaruNo ratings yet
- Case-Based Device Therapy for Heart FailureFrom EverandCase-Based Device Therapy for Heart FailureUlrika Birgersdotter-GreenNo ratings yet
- Atrial Fibrillation A Simple Guide to The Condition, Treatment And Related DiseasesFrom EverandAtrial Fibrillation A Simple Guide to The Condition, Treatment And Related DiseasesRating: 4 out of 5 stars4/5 (1)
- Alcain CPRDocument6 pagesAlcain CPRErika Trina AlcainNo ratings yet
- A Drug Study On: Furosemide TabletDocument7 pagesA Drug Study On: Furosemide TabletRaijenne VersolaNo ratings yet
- Cardiac ArrhythmiasDocument9 pagesCardiac ArrhythmiasRemelou Garchitorena AlfelorNo ratings yet
- NCP Impaired Gas Exchange STROKEDocument2 pagesNCP Impaired Gas Exchange STROKEMa. Elaine Carla TatingNo ratings yet
- Necrotizing Enterocolitis (Sultn Aiman NeazyDocument59 pagesNecrotizing Enterocolitis (Sultn Aiman NeazyMohammed ElhashimiNo ratings yet
- Perspective in Centre For Pharmaceutical Sciences (CPS), Institute of Science and Technology (IST)Document3 pagesPerspective in Centre For Pharmaceutical Sciences (CPS), Institute of Science and Technology (IST)Ardiene Shallouvette GamosoNo ratings yet
- Comparative Rates of Conduction System FiringDocument3 pagesComparative Rates of Conduction System FiringSulochana ChanNo ratings yet
- Internal Medicine Case Studies BMHDocument4 pagesInternal Medicine Case Studies BMHParsaant SinghNo ratings yet
- 7 The Meninges, CSFDocument22 pages7 The Meninges, CSFDavid KleinNo ratings yet
- DefibrillatorDocument85 pagesDefibrillatorDhruv DesaiNo ratings yet
- Assessing Vital Signs HandoutsDocument9 pagesAssessing Vital Signs Handoutsyhudz100% (3)
- Drug-StudyDocument1 pageDrug-StudyMhica PrestozaNo ratings yet
- Stress-Induced (Takotsubo) CardiomyopathyDocument13 pagesStress-Induced (Takotsubo) CardiomyopathyAdrian GeambasuNo ratings yet
- March 2023 Recalls Solved by Nazia RafiqueDocument18 pagesMarch 2023 Recalls Solved by Nazia RafiqueelgafarypharmacyNo ratings yet
- Hema Poikilocytosis StatPearls NCBI BookshelfDocument10 pagesHema Poikilocytosis StatPearls NCBI BookshelfVincent ReyesNo ratings yet
- Aortic RegurgitationDocument7 pagesAortic RegurgitationazaliavirsaNo ratings yet
- Zoology II (Em) BLM 21-22Document99 pagesZoology II (Em) BLM 21-22GANESH KANDAGATLANo ratings yet
- CTA CoronaryDocument39 pagesCTA CoronaryConsita VictoriaNo ratings yet
- Kaya ChikitsaDocument37 pagesKaya ChikitsaGAURAV100% (1)
- How To Take HistoryDocument59 pagesHow To Take HistoryBelalNo ratings yet
- Purpose of Emergency DrugsDocument8 pagesPurpose of Emergency DrugsShehnaz SheikhNo ratings yet
- HeartIndia54157-4958724 134627 PDFDocument3 pagesHeartIndia54157-4958724 134627 PDFGagandeep Singh ShergillNo ratings yet
- Health Assessment Lecture: - Review About THE Respiratory SystemDocument8 pagesHealth Assessment Lecture: - Review About THE Respiratory SystemHNo ratings yet
- AtherosclerosisDocument7 pagesAtherosclerosisFaris Mufid Madyaputra100% (1)
- Haversian System (Osteon) : Basic Structural UnitDocument7 pagesHaversian System (Osteon) : Basic Structural UnitJulius Matthew MarananNo ratings yet
- S-Bridging The Gap in Asthma Management (In-11244)Document34 pagesS-Bridging The Gap in Asthma Management (In-11244)w5bwmbfrtwNo ratings yet
- Blood Pharmacology 27-34Document8 pagesBlood Pharmacology 27-34ahmedsalah565vvvNo ratings yet