Download as pdf or txt
You might also like
- James Gurney - Dinotopia - A Land Apart From Time (SiPDF)Document168 pagesJames Gurney - Dinotopia - A Land Apart From Time (SiPDF)Sergio Mercado Gil98% (54)
- Chess Lesson Plan NewDocument3 pagesChess Lesson Plan NewJhen Mendoza100% (3)
- Sas 12 Den 032Document15 pagesSas 12 Den 032Alexa De GuzmanNo ratings yet
- Sas 15 Den 032Document19 pagesSas 15 Den 032Alexa De GuzmanNo ratings yet
- Sas 13 Den 032Document21 pagesSas 13 Den 032Alexa De GuzmanNo ratings yet
- Tutorial 6 SK 4 Blok 13Document19 pagesTutorial 6 SK 4 Blok 13Mutiah Dwi ariniNo ratings yet
- CA LS Bướu Nhiều Hốc - Multilocular Radiolucency in the Body of MandibleDocument4 pagesCA LS Bướu Nhiều Hốc - Multilocular Radiolucency in the Body of MandibleThành Luân NguyễnNo ratings yet
- Elizan, Trixia Mae A. SAS 2Document13 pagesElizan, Trixia Mae A. SAS 22rvbz4xmmqNo ratings yet
- Periodontics 1 Laboratory 2Document8 pagesPeriodontics 1 Laboratory 2Klariz Ira Abaniel SolmayorNo ratings yet
- Perio 1 DEN 039 SAS Module 2 Gingiva (Investing Tissue)Document12 pagesPerio 1 DEN 039 SAS Module 2 Gingiva (Investing Tissue)2rvbz4xmmqNo ratings yet
- Sas 14 Den 032Document17 pagesSas 14 Den 032Alexa De GuzmanNo ratings yet
- Cystic Lesions of MandibleDocument18 pagesCystic Lesions of MandibleRahul ShindeNo ratings yet
- Flint Cumming Otolaryngology CHAPTER 93 - Odontogenesis Odontogenic Cysts and Odontogenic TumorsDocument20 pagesFlint Cumming Otolaryngology CHAPTER 93 - Odontogenesis Odontogenic Cysts and Odontogenic TumorsNicco Jake AlegroNo ratings yet
- Ameloblastic Fibro-Odontoma: A Case ReportDocument4 pagesAmeloblastic Fibro-Odontoma: A Case Reportoral pathNo ratings yet
- Review Article: Pathogenesis OF Odontogenic Tumors OF Epithelial Origin-A ReviewDocument10 pagesReview Article: Pathogenesis OF Odontogenic Tumors OF Epithelial Origin-A ReviewIzzati Aqmar DarayaniNo ratings yet
- Mixed Tumors of Odontogenic Origin WordDocument31 pagesMixed Tumors of Odontogenic Origin WordAshimNo ratings yet
- 10 1016@j MPDHP 2020 01 004Document7 pages10 1016@j MPDHP 2020 01 004mohamaed abbasNo ratings yet
- Odonto Genic TumorsDocument7 pagesOdonto Genic TumorsMcmac YangoNo ratings yet
- Unicystic Ameloblastoma - Investigation Into An Enigma: IOSR Journal of Dental and Medical Sciences February 2020Document5 pagesUnicystic Ameloblastoma - Investigation Into An Enigma: IOSR Journal of Dental and Medical Sciences February 2020dr.filipcristian87No ratings yet
- Role of Bite Mark in Forensic Odontology - A Review: Dr. Shiva Kumar B, Dr. Deepthi. B. CDocument5 pagesRole of Bite Mark in Forensic Odontology - A Review: Dr. Shiva Kumar B, Dr. Deepthi. B. CRicka Widya RosalinaNo ratings yet
- Review Article: Bone Diseases of The JawsDocument7 pagesReview Article: Bone Diseases of The Jawsh20pologtNo ratings yet
- Clinical and Histopathological Investigation of Odontomas - Review of The Literature and Presentation of 160 CasesDocument4 pagesClinical and Histopathological Investigation of Odontomas - Review of The Literature and Presentation of 160 CasesdeathdesantosNo ratings yet
- No.24, II Eng.Document12 pagesNo.24, II Eng.Noli Sous NilNo ratings yet
- Ameloblastic Fibroma: Report of A Case: Su-Gwan Kim, DDS, PHD, and Hyun-Seon Jang, DDS, PHDDocument3 pagesAmeloblastic Fibroma: Report of A Case: Su-Gwan Kim, DDS, PHD, and Hyun-Seon Jang, DDS, PHDdoktergigikoeNo ratings yet
- Relative Prevalence of Odontogenic Cysts and Tumours in Kano Northern NigeriaDocument4 pagesRelative Prevalence of Odontogenic Cysts and Tumours in Kano Northern Nigeriablack_eagelNo ratings yet
- Oral Path Case Study PaperDocument4 pagesOral Path Case Study PaperSukirti MisraNo ratings yet
- A Complex Odontoma of The Anterior Maxilla AssociaDocument5 pagesA Complex Odontoma of The Anterior Maxilla AssociaJulka MadejNo ratings yet
- 6 Pediatric Odontogenic Tumors. Oral and Maxillofacial Surgery Clinics of North AmericaDocument14 pages6 Pediatric Odontogenic Tumors. Oral and Maxillofacial Surgery Clinics of North AmericaalexandreNo ratings yet
- Dental CariesDocument5 pagesDental CariesTwinamasiko DanielNo ratings yet
- OdontomasDocument4 pagesOdontomasArafat Masud Niloy100% (1)
- SAS - DEN041 - Lesson19 Orofacial CystsDocument13 pagesSAS - DEN041 - Lesson19 Orofacial Cysts2rvbz4xmmqNo ratings yet
- Tumores Odontogenicos Patología PDFDocument17 pagesTumores Odontogenicos Patología PDFDayanara Medina AldazNo ratings yet
- Jurnal Asli JR Radiologi - Unusual Giant Complex Odontoma A Case ReportDocument4 pagesJurnal Asli JR Radiologi - Unusual Giant Complex Odontoma A Case ReportAliaNo ratings yet
- Odontoma Compound 1Document4 pagesOdontoma Compound 1ashariNo ratings yet
- Odontogenic Tumors and Related Jaw Lesions: A) Benign Epithelial TumorsDocument19 pagesOdontogenic Tumors and Related Jaw Lesions: A) Benign Epithelial Tumorsluna zeidNo ratings yet
- Benign and MalignantDocument16 pagesBenign and MalignantRSU DUTA MULYANo ratings yet
- 3.podoplanin Antibody MainDocument6 pages3.podoplanin Antibody MainNitin KhanduriNo ratings yet
- Odontogenic Tumor Ameloblastoma: Presented By: Ankita Singh Bds Final Year Roll No 37Document73 pagesOdontogenic Tumor Ameloblastoma: Presented By: Ankita Singh Bds Final Year Roll No 37ankita sethiNo ratings yet
- Jurnal 20 PDFDocument10 pagesJurnal 20 PDFsriwahyuutamiNo ratings yet
- Classification of Periradicular Pathosis:: 4-Acute Apical AbscessDocument7 pagesClassification of Periradicular Pathosis:: 4-Acute Apical AbscessOmar MohamedNo ratings yet
- Session 8 Odontogenic and Non Odontogenic TumorsDocument74 pagesSession 8 Odontogenic and Non Odontogenic TumorsZNo ratings yet
- Odontogenic Tumor PDFDocument93 pagesOdontogenic Tumor PDFEmad Alriashy100% (1)
- Mds Oral Pathology Thesis TopicsDocument7 pagesMds Oral Pathology Thesis Topicsafkodkedr100% (2)
- Odontogenic Cysts and Tumors What Radiologists Need To Know 2019Document22 pagesOdontogenic Cysts and Tumors What Radiologists Need To Know 2019Fadly RasyidNo ratings yet
- Differential Diagnosis of Tongue LesionsDocument12 pagesDifferential Diagnosis of Tongue LesionsKartikakhairaniNo ratings yet
- Delayed Tooth EmergenceDocument16 pagesDelayed Tooth EmergenceValeria CernegaNo ratings yet
- 1365-Article Text-6854-1-10-20220126Document4 pages1365-Article Text-6854-1-10-20220126brendaNo ratings yet
- Session 6 TeethDocument11 pagesSession 6 TeethTobio KageyamaNo ratings yet
- Oral Pathology - Case Study 1 - FinalDocument5 pagesOral Pathology - Case Study 1 - Finalapi-262534732No ratings yet
- Multilocular Radiolucencies of The JawsDocument4 pagesMultilocular Radiolucencies of The Jawsdr.sonalNo ratings yet
- JPNR - S04 - 233Document6 pagesJPNR - S04 - 233Ferisa paraswatiNo ratings yet
- 2013 Article 501Document3 pages2013 Article 501oral pathNo ratings yet
- Molar Impactions: Etiology, Implications and Treatment Modalities With Presentation of An Unusual CaseDocument3 pagesMolar Impactions: Etiology, Implications and Treatment Modalities With Presentation of An Unusual Casemagus davilaNo ratings yet
- Introduction Cysts of JawsDocument62 pagesIntroduction Cysts of JawsFatima Siddiqui100% (1)
- Case Report Ameloblastic Fibroma: Report of 3 Cases and Literature ReviewDocument5 pagesCase Report Ameloblastic Fibroma: Report of 3 Cases and Literature ReviewcareNo ratings yet
- Radicular Cyst With Primary Mandibular Molar A RarDocument5 pagesRadicular Cyst With Primary Mandibular Molar A RargarciadeluisaNo ratings yet
- Compound Odontoma Associated With Impacted Maxillary Anterior Teeth A Case ReportDocument4 pagesCompound Odontoma Associated With Impacted Maxillary Anterior Teeth A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Management of Unicystic Ameloblastoma Crossing Midline in Mandible in Geriatric Patient - July - 2020 - 9370586511 - 3513376Document3 pagesManagement of Unicystic Ameloblastoma Crossing Midline in Mandible in Geriatric Patient - July - 2020 - 9370586511 - 3513376Sowmya ManthaNo ratings yet
- Odonto MaDocument5 pagesOdonto MaashariNo ratings yet
- Bds Oral Patholgy MicrobiologyDocument9 pagesBds Oral Patholgy MicrobiologyVegda PoojaNo ratings yet
- The Periodontal Pocket PDFDocument9 pagesThe Periodontal Pocket PDFIgnacio PulleyNo ratings yet
- The Dental Pulp: Biology, Pathology, and Regenerative TherapiesFrom EverandThe Dental Pulp: Biology, Pathology, and Regenerative TherapiesNo ratings yet
- UNFCU Foundation Grant Application 2019Document4 pagesUNFCU Foundation Grant Application 2019Anonymous PbCsXeZNo ratings yet
- Joinery FlowchartDocument1 pageJoinery FlowchartrjNo ratings yet
- IJTK SupplementaryDocument9 pagesIJTK SupplementaryNastySon FootNimbusNo ratings yet
- Partograph 3Document49 pagesPartograph 3Geeta BhardwajNo ratings yet
- Schematic Diagram of Relay & Tcms Panel T: REV Revised by Checked by Approved byDocument1 pageSchematic Diagram of Relay & Tcms Panel T: REV Revised by Checked by Approved byTaufiq HidayatNo ratings yet
- Nurses Bill of RightsDocument1 pageNurses Bill of RightsFlauros Ryu Jabien100% (1)
- Autodesk Navisworks Installation GuideDocument120 pagesAutodesk Navisworks Installation GuidemindwriterNo ratings yet
- Test Bank For Child Development A Thematic Approach 6th EditionDocument6 pagesTest Bank For Child Development A Thematic Approach 6th EditionCharles Pando100% (44)
- SS2 Chemistry 3rd Term Lesson Note PDFDocument97 pagesSS2 Chemistry 3rd Term Lesson Note PDFkhaleedoshodi7No ratings yet
- Damped HoDocument3 pagesDamped Homani kandanNo ratings yet
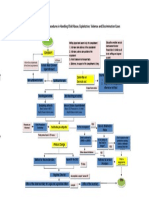
- Rules and Procedures in Handling Child Abuse CasesDocument1 pageRules and Procedures in Handling Child Abuse CasesJoyce Carreon50% (2)
- Stop Using Pandas To Read - Write Data - This Alternative Is 7 Times Faster - by Dario Radečić - Oct, 2021 - Towards Data ScienceDocument10 pagesStop Using Pandas To Read - Write Data - This Alternative Is 7 Times Faster - by Dario Radečić - Oct, 2021 - Towards Data ScienceVítor Luís Pauda da SilvaNo ratings yet
- DANCE PPT For RizalDocument40 pagesDANCE PPT For RizalAngelica perezNo ratings yet
- A Flangeless Complete Denture Prosthesis A Case Report April 2017 7862206681 3603082Document2 pagesA Flangeless Complete Denture Prosthesis A Case Report April 2017 7862206681 3603082wdyNo ratings yet
- GT Gold Corp.: Release Date: 25 June 2020Document12 pagesGT Gold Corp.: Release Date: 25 June 2020anon analyticsNo ratings yet
- Admin Law DigestDocument49 pagesAdmin Law DigestMichelle Muhrie TablizoNo ratings yet
- Slide 1Document4 pagesSlide 1Monika JosephNo ratings yet
- At Professional Responsibilities and Other Topics With AnswersDocument27 pagesAt Professional Responsibilities and Other Topics With AnswersShielle AzonNo ratings yet
- Accessibility of Urban Green Infrastructure in Addis-Ababa City, Ethiopia: Current Status and Future ChallengeDocument20 pagesAccessibility of Urban Green Infrastructure in Addis-Ababa City, Ethiopia: Current Status and Future ChallengeShemeles MitkieNo ratings yet
- Ajit ResumeDocument3 pagesAjit ResumeSreeluNo ratings yet
- Use of Almond Our and Stevia in Rice-Based Gluten-Free Cookie ProductionDocument13 pagesUse of Almond Our and Stevia in Rice-Based Gluten-Free Cookie ProductionLoredana Veronica ZalischiNo ratings yet
- BioclimaticDocument9 pagesBioclimaticHaber HaberNo ratings yet
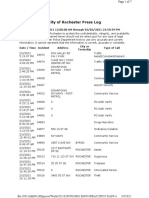
- RPD Daily Incident Report 2/3/21Document7 pagesRPD Daily Incident Report 2/3/21inforumdocsNo ratings yet
- 10 Acts of KindnessDocument1 page10 Acts of KindnessKim Penaflorida100% (1)
- Powerful Phrases For Customer ServiceDocument16 pagesPowerful Phrases For Customer ServiceArturo GallardoNo ratings yet
- MicroChannel HeatExchangersDocument16 pagesMicroChannel HeatExchangerskhushal bhanderiNo ratings yet
- Anuj Nijhon - The Toyota WayDocument35 pagesAnuj Nijhon - The Toyota WayAnuj NijhonNo ratings yet
- E-Auctions - MSTC Limited-TATA POWER HALDIADocument7 pagesE-Auctions - MSTC Limited-TATA POWER HALDIAmannakauNo ratings yet