
All Slides-1-67-2
All Slides-1-67-2
You might also like
- Stress Management 101 BookDocument335 pagesStress Management 101 BookAnisa Strachan100% (9)
- Dermatology Mini-OSCEDocument322 pagesDermatology Mini-OSCEMarrkNo ratings yet
- Surgery Clerkship Oral Exam ReviewDocument18 pagesSurgery Clerkship Oral Exam Reviewpanther795100% (1)
- Sarcoidosis Remission Aden ProtocolDocument127 pagesSarcoidosis Remission Aden Protocoljodywhitaker100% (6)
- OphthalmologyDocument144 pagesOphthalmologyrosaririsNo ratings yet
- Fungal Infection Part 2Document39 pagesFungal Infection Part 2Abaan QaisNo ratings yet
- Lecture 5 - PseudopyodermasDocument47 pagesLecture 5 - Pseudopyodermasceleste omegaNo ratings yet
- Race Dermatology 2024 by DR AshishDocument29 pagesRace Dermatology 2024 by DR AshishdrshekarforyouNo ratings yet
- Dermatology WorkbookDocument162 pagesDermatology Workbookwisegot586No ratings yet
- Microbial Diseases of The SkinDocument4 pagesMicrobial Diseases of The Skinjana.alngNo ratings yet
- 2 DermatomikosisDocument47 pages2 DermatomikosisLintang WahyuNo ratings yet
- Reviewer: Ramona Flordeliza Fabie DimaanoDocument41 pagesReviewer: Ramona Flordeliza Fabie DimaanoKevin Michael Fabie BautistaNo ratings yet
- Uveal TractDocument4 pagesUveal TractMohamed GhanemNo ratings yet
- Endotoxin: Watery Diarrhea in Aids PatientDocument13 pagesEndotoxin: Watery Diarrhea in Aids PatientRyan TurnerNo ratings yet
- How To Manage Vector-Borne Viral Disease As General Practitioner in Primary Health Care? (Dengue-Chikungunya-Zika Infection)Document83 pagesHow To Manage Vector-Borne Viral Disease As General Practitioner in Primary Health Care? (Dengue-Chikungunya-Zika Infection)fida amalinaNo ratings yet
- Male Genital DermDocument112 pagesMale Genital DermVũ CaoNo ratings yet
- 膚科Document191 pages膚科Sai TaiNo ratings yet
- Prezentare TEN EnglezaDocument27 pagesPrezentare TEN EnglezaAlinaNo ratings yet
- Skinl3 WEB09Document50 pagesSkinl3 WEB09Gwyneth Koleen LopezNo ratings yet
- CCF - Derm Rahul damnyaPDFDocument101 pagesCCF - Derm Rahul damnyaPDFRajul Patel100% (1)
- Community OmaraDocument33 pagesCommunity Omarasayf ahmedNo ratings yet
- MergedDocument17 pagesMergedJack Ortega PuruggananNo ratings yet
- (Mantap) Slide Materi Mata Batch 3 2018Document164 pages(Mantap) Slide Materi Mata Batch 3 2018fifinnurfina50% (2)
- The Cornea PPT EditDocument38 pagesThe Cornea PPT EditRahman Setiawan100% (1)
- EedDocument70 pagesEedzihniyya471No ratings yet
- Bacte MidtermDocument40 pagesBacte MidtermTrangia, SharmaineNo ratings yet
- Emed - Pedia 1Document7 pagesEmed - Pedia 1Princess Cate MercadoNo ratings yet
- LEPTOSPIRADocument31 pagesLEPTOSPIRADinar NastitiNo ratings yet
- Derm Blue BookDocument48 pagesDerm Blue BookQaphela MinenhleNo ratings yet
- Kul Mata Merah PDFDocument56 pagesKul Mata Merah PDFMuhammad HasanNo ratings yet
- 10a Dermatitis AtopikDocument27 pages10a Dermatitis Atopikwuryan dewiNo ratings yet
- Outline: Common Dermatologic Disorders: Tips For Diagnosis and ManagementDocument41 pagesOutline: Common Dermatologic Disorders: Tips For Diagnosis and ManagementJobelle Fernandez-SantosNo ratings yet
- Step 2 Paeds NuggetsDocument31 pagesStep 2 Paeds NuggetsNoor JehanNo ratings yet
- Oral Pathology ChaptersDocument8 pagesOral Pathology ChaptersHazem MouradNo ratings yet
- Bacteriology Edited 1Document65 pagesBacteriology Edited 1Ali AhmedNo ratings yet
- Dermatology Revision E6.5 @theboggusdocDocument36 pagesDermatology Revision E6.5 @theboggusdockhushi koliNo ratings yet
- (Download PDF) Fitzpatricks Color Atlas and Synopsis of Clinical Dermatology Eighth Edition 8Th Edition PDF Full Chapter PDFDocument53 pages(Download PDF) Fitzpatricks Color Atlas and Synopsis of Clinical Dermatology Eighth Edition 8Th Edition PDF Full Chapter PDFolintoecrin100% (7)
- Morbus HansenDocument37 pagesMorbus HansenYolanda Agnesia Purba100% (1)
- Deputy Provost MCHDocument250 pagesDeputy Provost MCHrahmatullahqueenmercyNo ratings yet
- Oftalmologi Batch November 2017 - UnlockedDocument153 pagesOftalmologi Batch November 2017 - Unlockeddzulkifli sukriNo ratings yet
- Dermatology - Essays - Sun 2016Document6 pagesDermatology - Essays - Sun 2016rabeca johnsonNo ratings yet
- Leprosy (Morbus Hansen) : Dr. Uun Khusnul Khotimah, SPKKDocument38 pagesLeprosy (Morbus Hansen) : Dr. Uun Khusnul Khotimah, SPKKagilNo ratings yet
- Bacterial Skin InfectionDocument4 pagesBacterial Skin InfectionAngeline TaghapNo ratings yet
- Boards II Pages 1 121Document120 pagesBoards II Pages 1 121karate.b97No ratings yet
- Top Up Training Center and Research Consultancy Communicable Disease NursingDocument3 pagesTop Up Training Center and Research Consultancy Communicable Disease NursingSTEFFI GABRIELLE GOLEZNo ratings yet
- Gram Positive BacteriaDocument88 pagesGram Positive BacteriaRonelene GatoNo ratings yet
- 150 - Mycobacterium LepraeDocument83 pages150 - Mycobacterium LepraeNirav PatelNo ratings yet
- Bahan Pemicu 5 Penginderaan: Ivan Buntara 405120049Document62 pagesBahan Pemicu 5 Penginderaan: Ivan Buntara 405120049AdamNo ratings yet
- Corneea EnglishDocument57 pagesCorneea EnglishGermanyNo ratings yet
- ConjungtivitisDocument86 pagesConjungtivitisIvo AfianiNo ratings yet
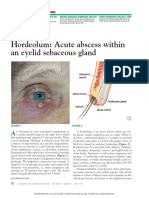
- Hordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureDocument3 pagesHordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureCamNo ratings yet
- Keratoconjunctivitis Sicca: in DogsDocument8 pagesKeratoconjunctivitis Sicca: in DogsGABRIELA VERGARA PEREZNo ratings yet
- Stevens-Johnson Syndrome Diagnosis: Sofya Sugi Setyawati Sembiring (1801000016)Document19 pagesStevens-Johnson Syndrome Diagnosis: Sofya Sugi Setyawati Sembiring (1801000016)Wer TeumeNo ratings yet
- 744 Mycobacterium LepraeDocument83 pages744 Mycobacterium Lepraeabhiaishu.kanna26No ratings yet
- Dermatology BookDocument13 pagesDermatology BookYezenashNo ratings yet
- StaphDocument6 pagesStaphpekibelssNo ratings yet
- EkcemiDocument35 pagesEkcemiSnj SnjNo ratings yet
- Necrotizing Fasciitis: BY Hosam Mohammad Hamza, MSCDocument24 pagesNecrotizing Fasciitis: BY Hosam Mohammad Hamza, MSCKana FajarNo ratings yet
- Part 1Document15 pagesPart 1solimanmahmoudaNo ratings yet
- DERM NotesDocument19 pagesDERM NoteszakyNo ratings yet
- Ipm Dan Diagnoosis Banding IntegumenDocument13 pagesIpm Dan Diagnoosis Banding IntegumenAbrorMuhammadNo ratings yet
- Evidence-Based OphthalmologyFrom EverandEvidence-Based OphthalmologyRichard WormaldNo ratings yet
- Citrus Tristeza by Cvag Path 372Document14 pagesCitrus Tristeza by Cvag Path 372Shivaji Eesam (Ragnar)No ratings yet
- Assg The NotebookDocument4 pagesAssg The NotebookNurul IzzatulNo ratings yet
- BSP1A - M1-Check-In Activity 4 - AldeDocument2 pagesBSP1A - M1-Check-In Activity 4 - AldeMarissa AldeNo ratings yet
- Neuro Week 13 AnswersDocument41 pagesNeuro Week 13 AnswersCJ RelleveNo ratings yet
- Mrcs UrologyDocument78 pagesMrcs UrologyAdebisiNo ratings yet
- CNS Infections: Rashmi KumarDocument32 pagesCNS Infections: Rashmi Kumarfasil tadesseNo ratings yet
- Hyperinflated LungsDocument10 pagesHyperinflated LungsGplsHub.comNo ratings yet
- Biographical DataDocument2 pagesBiographical DataKenzo WongNo ratings yet
- EMS Health Declaration Form For Applicant-V2Document1 pageEMS Health Declaration Form For Applicant-V2MettaNo ratings yet
- Flyer Symposium INOIIS X PERDAMI JabarDocument7 pagesFlyer Symposium INOIIS X PERDAMI JabarBonita AsyigahNo ratings yet
- Homeopathy in DentalDocument5 pagesHomeopathy in Dentaljd59hs82d6No ratings yet
- Conversion Disorder-1Document11 pagesConversion Disorder-1zainiNo ratings yet
- Postpartum Psychosis: Madness, Mania, and Melancholia in MotherhoodDocument10 pagesPostpartum Psychosis: Madness, Mania, and Melancholia in MotherhoodAndreeaNicoletaNo ratings yet
- A Study On Impact of Covid-19 in The Indian EconomyDocument62 pagesA Study On Impact of Covid-19 in The Indian Economyanam882001No ratings yet
- Effects of High Dose Vitamin C Supplementation On Severe Covid19 Patients in The ICU - A Retrospective AnalysisDocument1 pageEffects of High Dose Vitamin C Supplementation On Severe Covid19 Patients in The ICU - A Retrospective AnalysiszipzoinkNo ratings yet
- Noro Virus - Analytical MicrobiologyDocument12 pagesNoro Virus - Analytical Microbiologykolita kamal100% (1)
- Jawbone CavitationsDocument8 pagesJawbone CavitationsCAESA96No ratings yet
- St. Michael's College: Nursing Care Plan FormDocument3 pagesSt. Michael's College: Nursing Care Plan Formacademic purposesNo ratings yet
- Skin Scraping and A Potassium Hydroxide Mount, KOHDocument4 pagesSkin Scraping and A Potassium Hydroxide Mount, KOHKuldeepSinghBanaNo ratings yet
- Khin Khin Lay - 2007 - Prevalence of Cryptosporidium, Giardia and Other Gastrointestinal Parasites in Dairy Calves in Mandalay, MyanmarDocument98 pagesKhin Khin Lay - 2007 - Prevalence of Cryptosporidium, Giardia and Other Gastrointestinal Parasites in Dairy Calves in Mandalay, MyanmarwiwienNo ratings yet
- Reading Sub-Test - Question Paper: Part CDocument10 pagesReading Sub-Test - Question Paper: Part CSarah Jane PetalioNo ratings yet
- Paper 1Document27 pagesPaper 1christopher25No ratings yet
- Sickle Cell Anaemia and Malaria PDFDocument6 pagesSickle Cell Anaemia and Malaria PDFshjahsjanshaNo ratings yet
- General Surgery Lecture N: 1. Bone FractureDocument11 pagesGeneral Surgery Lecture N: 1. Bone FractureAmal ShereefNo ratings yet
- Cancer and Carcinogens: Consumer ChemistryDocument29 pagesCancer and Carcinogens: Consumer ChemistryAshlie AbalaNo ratings yet
- SCE Nephrology Sample Questions 51-70 PDFDocument18 pagesSCE Nephrology Sample Questions 51-70 PDFayo odeyemi100% (1)
- Congenital Anomalies Developmental Disorders DysplasiasDocument128 pagesCongenital Anomalies Developmental Disorders Dysplasiasalsead798No ratings yet





















































































Download as pdf or txt
You might also like
- Stress Management 101 BookDocument335 pagesStress Management 101 BookAnisa Strachan100% (9)
- Dermatology Mini-OSCEDocument322 pagesDermatology Mini-OSCEMarrkNo ratings yet
- Surgery Clerkship Oral Exam ReviewDocument18 pagesSurgery Clerkship Oral Exam Reviewpanther795100% (1)
- Sarcoidosis Remission Aden ProtocolDocument127 pagesSarcoidosis Remission Aden Protocoljodywhitaker100% (6)
- OphthalmologyDocument144 pagesOphthalmologyrosaririsNo ratings yet
- Fungal Infection Part 2Document39 pagesFungal Infection Part 2Abaan QaisNo ratings yet
- Lecture 5 - PseudopyodermasDocument47 pagesLecture 5 - Pseudopyodermasceleste omegaNo ratings yet
- Race Dermatology 2024 by DR AshishDocument29 pagesRace Dermatology 2024 by DR AshishdrshekarforyouNo ratings yet
- Dermatology WorkbookDocument162 pagesDermatology Workbookwisegot586No ratings yet
- Microbial Diseases of The SkinDocument4 pagesMicrobial Diseases of The Skinjana.alngNo ratings yet
- 2 DermatomikosisDocument47 pages2 DermatomikosisLintang WahyuNo ratings yet
- Reviewer: Ramona Flordeliza Fabie DimaanoDocument41 pagesReviewer: Ramona Flordeliza Fabie DimaanoKevin Michael Fabie BautistaNo ratings yet
- Uveal TractDocument4 pagesUveal TractMohamed GhanemNo ratings yet
- Endotoxin: Watery Diarrhea in Aids PatientDocument13 pagesEndotoxin: Watery Diarrhea in Aids PatientRyan TurnerNo ratings yet
- How To Manage Vector-Borne Viral Disease As General Practitioner in Primary Health Care? (Dengue-Chikungunya-Zika Infection)Document83 pagesHow To Manage Vector-Borne Viral Disease As General Practitioner in Primary Health Care? (Dengue-Chikungunya-Zika Infection)fida amalinaNo ratings yet
- Male Genital DermDocument112 pagesMale Genital DermVũ CaoNo ratings yet
- 膚科Document191 pages膚科Sai TaiNo ratings yet
- Prezentare TEN EnglezaDocument27 pagesPrezentare TEN EnglezaAlinaNo ratings yet
- Skinl3 WEB09Document50 pagesSkinl3 WEB09Gwyneth Koleen LopezNo ratings yet
- CCF - Derm Rahul damnyaPDFDocument101 pagesCCF - Derm Rahul damnyaPDFRajul Patel100% (1)
- Community OmaraDocument33 pagesCommunity Omarasayf ahmedNo ratings yet
- MergedDocument17 pagesMergedJack Ortega PuruggananNo ratings yet
- (Mantap) Slide Materi Mata Batch 3 2018Document164 pages(Mantap) Slide Materi Mata Batch 3 2018fifinnurfina50% (2)
- The Cornea PPT EditDocument38 pagesThe Cornea PPT EditRahman Setiawan100% (1)
- EedDocument70 pagesEedzihniyya471No ratings yet
- Bacte MidtermDocument40 pagesBacte MidtermTrangia, SharmaineNo ratings yet
- Emed - Pedia 1Document7 pagesEmed - Pedia 1Princess Cate MercadoNo ratings yet
- LEPTOSPIRADocument31 pagesLEPTOSPIRADinar NastitiNo ratings yet
- Derm Blue BookDocument48 pagesDerm Blue BookQaphela MinenhleNo ratings yet
- Kul Mata Merah PDFDocument56 pagesKul Mata Merah PDFMuhammad HasanNo ratings yet
- 10a Dermatitis AtopikDocument27 pages10a Dermatitis Atopikwuryan dewiNo ratings yet
- Outline: Common Dermatologic Disorders: Tips For Diagnosis and ManagementDocument41 pagesOutline: Common Dermatologic Disorders: Tips For Diagnosis and ManagementJobelle Fernandez-SantosNo ratings yet
- Step 2 Paeds NuggetsDocument31 pagesStep 2 Paeds NuggetsNoor JehanNo ratings yet
- Oral Pathology ChaptersDocument8 pagesOral Pathology ChaptersHazem MouradNo ratings yet
- Bacteriology Edited 1Document65 pagesBacteriology Edited 1Ali AhmedNo ratings yet
- Dermatology Revision E6.5 @theboggusdocDocument36 pagesDermatology Revision E6.5 @theboggusdockhushi koliNo ratings yet
- (Download PDF) Fitzpatricks Color Atlas and Synopsis of Clinical Dermatology Eighth Edition 8Th Edition PDF Full Chapter PDFDocument53 pages(Download PDF) Fitzpatricks Color Atlas and Synopsis of Clinical Dermatology Eighth Edition 8Th Edition PDF Full Chapter PDFolintoecrin100% (7)
- Morbus HansenDocument37 pagesMorbus HansenYolanda Agnesia Purba100% (1)
- Deputy Provost MCHDocument250 pagesDeputy Provost MCHrahmatullahqueenmercyNo ratings yet
- Oftalmologi Batch November 2017 - UnlockedDocument153 pagesOftalmologi Batch November 2017 - Unlockeddzulkifli sukriNo ratings yet
- Dermatology - Essays - Sun 2016Document6 pagesDermatology - Essays - Sun 2016rabeca johnsonNo ratings yet
- Leprosy (Morbus Hansen) : Dr. Uun Khusnul Khotimah, SPKKDocument38 pagesLeprosy (Morbus Hansen) : Dr. Uun Khusnul Khotimah, SPKKagilNo ratings yet
- Bacterial Skin InfectionDocument4 pagesBacterial Skin InfectionAngeline TaghapNo ratings yet
- Boards II Pages 1 121Document120 pagesBoards II Pages 1 121karate.b97No ratings yet
- Top Up Training Center and Research Consultancy Communicable Disease NursingDocument3 pagesTop Up Training Center and Research Consultancy Communicable Disease NursingSTEFFI GABRIELLE GOLEZNo ratings yet
- Gram Positive BacteriaDocument88 pagesGram Positive BacteriaRonelene GatoNo ratings yet
- 150 - Mycobacterium LepraeDocument83 pages150 - Mycobacterium LepraeNirav PatelNo ratings yet
- Bahan Pemicu 5 Penginderaan: Ivan Buntara 405120049Document62 pagesBahan Pemicu 5 Penginderaan: Ivan Buntara 405120049AdamNo ratings yet
- Corneea EnglishDocument57 pagesCorneea EnglishGermanyNo ratings yet
- ConjungtivitisDocument86 pagesConjungtivitisIvo AfianiNo ratings yet
- Hordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureDocument3 pagesHordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureCamNo ratings yet
- Keratoconjunctivitis Sicca: in DogsDocument8 pagesKeratoconjunctivitis Sicca: in DogsGABRIELA VERGARA PEREZNo ratings yet
- Stevens-Johnson Syndrome Diagnosis: Sofya Sugi Setyawati Sembiring (1801000016)Document19 pagesStevens-Johnson Syndrome Diagnosis: Sofya Sugi Setyawati Sembiring (1801000016)Wer TeumeNo ratings yet
- 744 Mycobacterium LepraeDocument83 pages744 Mycobacterium Lepraeabhiaishu.kanna26No ratings yet
- Dermatology BookDocument13 pagesDermatology BookYezenashNo ratings yet
- StaphDocument6 pagesStaphpekibelssNo ratings yet
- EkcemiDocument35 pagesEkcemiSnj SnjNo ratings yet
- Necrotizing Fasciitis: BY Hosam Mohammad Hamza, MSCDocument24 pagesNecrotizing Fasciitis: BY Hosam Mohammad Hamza, MSCKana FajarNo ratings yet
- Part 1Document15 pagesPart 1solimanmahmoudaNo ratings yet
- DERM NotesDocument19 pagesDERM NoteszakyNo ratings yet
- Ipm Dan Diagnoosis Banding IntegumenDocument13 pagesIpm Dan Diagnoosis Banding IntegumenAbrorMuhammadNo ratings yet
- Evidence-Based OphthalmologyFrom EverandEvidence-Based OphthalmologyRichard WormaldNo ratings yet
- Citrus Tristeza by Cvag Path 372Document14 pagesCitrus Tristeza by Cvag Path 372Shivaji Eesam (Ragnar)No ratings yet
- Assg The NotebookDocument4 pagesAssg The NotebookNurul IzzatulNo ratings yet
- BSP1A - M1-Check-In Activity 4 - AldeDocument2 pagesBSP1A - M1-Check-In Activity 4 - AldeMarissa AldeNo ratings yet
- Neuro Week 13 AnswersDocument41 pagesNeuro Week 13 AnswersCJ RelleveNo ratings yet
- Mrcs UrologyDocument78 pagesMrcs UrologyAdebisiNo ratings yet
- CNS Infections: Rashmi KumarDocument32 pagesCNS Infections: Rashmi Kumarfasil tadesseNo ratings yet
- Hyperinflated LungsDocument10 pagesHyperinflated LungsGplsHub.comNo ratings yet
- Biographical DataDocument2 pagesBiographical DataKenzo WongNo ratings yet
- EMS Health Declaration Form For Applicant-V2Document1 pageEMS Health Declaration Form For Applicant-V2MettaNo ratings yet
- Flyer Symposium INOIIS X PERDAMI JabarDocument7 pagesFlyer Symposium INOIIS X PERDAMI JabarBonita AsyigahNo ratings yet
- Homeopathy in DentalDocument5 pagesHomeopathy in Dentaljd59hs82d6No ratings yet
- Conversion Disorder-1Document11 pagesConversion Disorder-1zainiNo ratings yet
- Postpartum Psychosis: Madness, Mania, and Melancholia in MotherhoodDocument10 pagesPostpartum Psychosis: Madness, Mania, and Melancholia in MotherhoodAndreeaNicoletaNo ratings yet
- A Study On Impact of Covid-19 in The Indian EconomyDocument62 pagesA Study On Impact of Covid-19 in The Indian Economyanam882001No ratings yet
- Effects of High Dose Vitamin C Supplementation On Severe Covid19 Patients in The ICU - A Retrospective AnalysisDocument1 pageEffects of High Dose Vitamin C Supplementation On Severe Covid19 Patients in The ICU - A Retrospective AnalysiszipzoinkNo ratings yet
- Noro Virus - Analytical MicrobiologyDocument12 pagesNoro Virus - Analytical Microbiologykolita kamal100% (1)
- Jawbone CavitationsDocument8 pagesJawbone CavitationsCAESA96No ratings yet
- St. Michael's College: Nursing Care Plan FormDocument3 pagesSt. Michael's College: Nursing Care Plan Formacademic purposesNo ratings yet
- Skin Scraping and A Potassium Hydroxide Mount, KOHDocument4 pagesSkin Scraping and A Potassium Hydroxide Mount, KOHKuldeepSinghBanaNo ratings yet
- Khin Khin Lay - 2007 - Prevalence of Cryptosporidium, Giardia and Other Gastrointestinal Parasites in Dairy Calves in Mandalay, MyanmarDocument98 pagesKhin Khin Lay - 2007 - Prevalence of Cryptosporidium, Giardia and Other Gastrointestinal Parasites in Dairy Calves in Mandalay, MyanmarwiwienNo ratings yet
- Reading Sub-Test - Question Paper: Part CDocument10 pagesReading Sub-Test - Question Paper: Part CSarah Jane PetalioNo ratings yet
- Paper 1Document27 pagesPaper 1christopher25No ratings yet
- Sickle Cell Anaemia and Malaria PDFDocument6 pagesSickle Cell Anaemia and Malaria PDFshjahsjanshaNo ratings yet
- General Surgery Lecture N: 1. Bone FractureDocument11 pagesGeneral Surgery Lecture N: 1. Bone FractureAmal ShereefNo ratings yet
- Cancer and Carcinogens: Consumer ChemistryDocument29 pagesCancer and Carcinogens: Consumer ChemistryAshlie AbalaNo ratings yet
- SCE Nephrology Sample Questions 51-70 PDFDocument18 pagesSCE Nephrology Sample Questions 51-70 PDFayo odeyemi100% (1)
- Congenital Anomalies Developmental Disorders DysplasiasDocument128 pagesCongenital Anomalies Developmental Disorders Dysplasiasalsead798No ratings yet