
Idpccm Examination Form
Idpccm Examination Form
You might also like
- Ebook Hazzards Geriatric Medicine and Gerontology 8Th Ed PDF Full Chapter PDFDocument67 pagesEbook Hazzards Geriatric Medicine and Gerontology 8Th Ed PDF Full Chapter PDFnancy.stice552100% (36)
- Investor Deck - Doctor Insta PDFDocument28 pagesInvestor Deck - Doctor Insta PDFSamarjit Samanta100% (3)
- Shnider and Levinsons Anesthesia For Obstetrics, 5th EdDocument879 pagesShnider and Levinsons Anesthesia For Obstetrics, 5th EdSri Hari50% (2)
- Textbook of Reumathology-Kelley's PDFDocument1,909 pagesTextbook of Reumathology-Kelley's PDFFlorentina Sterghiu100% (4)
- 2.Crcp Application Form 20210114Document2 pages2.Crcp Application Form 20210114Neha GulfamNo ratings yet
- M.e.ph.d Form 2011-12Document9 pagesM.e.ph.d Form 2011-12prakashsahu_84No ratings yet
- E1 E2 E3 E4 FormsDocument8 pagesE1 E2 E3 E4 FormsAbeel IrshadNo ratings yet
- Admission Form BDS 2017-18Document2 pagesAdmission Form BDS 2017-18Shoaib JadoonNo ratings yet
- UTU MTech Application FormDocument6 pagesUTU MTech Application FormAnweshaBoseNo ratings yet
- Adevrtisement Application FormDocument4 pagesAdevrtisement Application FormMùzÃmîl SåMbøråNo ratings yet
- Admission Application Form: Section 1: Personal DataDocument5 pagesAdmission Application Form: Section 1: Personal DatamahmadwasiNo ratings yet
- Indian Maritime University: SL - No.Document4 pagesIndian Maritime University: SL - No.Nivedhitha VivekanandhanNo ratings yet
- Application Form May 2023Document4 pagesApplication Form May 2023derrick andivaNo ratings yet
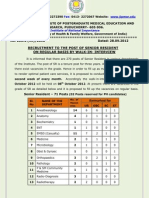
- Dermatology 1 Pathology, 1 Ophthalmology 1: No of VacancyDocument3 pagesDermatology 1 Pathology, 1 Ophthalmology 1: No of VacancyKirankumar MutnaliNo ratings yet
- Application Form-2019 PDFDocument2 pagesApplication Form-2019 PDFNazneen ShaikNo ratings yet
- O o o o o o o o o o o O: Khyber Medical UniversityDocument3 pagesO o o o o o o o o o o O: Khyber Medical UniversitySobar KhanNo ratings yet
- AdmissionDocument8 pagesAdmissionQuestion BankNo ratings yet
- UERM ApplicationDocument5 pagesUERM ApplicationJasper Benjamin JuradoNo ratings yet
- Bs Medical Technology FormDocument2 pagesBs Medical Technology FormAnonymous CWdCHHSX9qNo ratings yet
- Application For Admission Into APGDEC 2010 - 23.03Document2 pagesApplication For Admission Into APGDEC 2010 - 23.03Sumedh BeleNo ratings yet
- Registration Form: - Fellow - Junior Fellow - Medical Student MemberDocument4 pagesRegistration Form: - Fellow - Junior Fellow - Medical Student MemberWahyu SutrisnaNo ratings yet
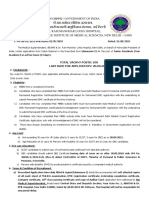
- Total Vacant Posts: 100 Last Date For Application: 20.09.2021Document4 pagesTotal Vacant Posts: 100 Last Date For Application: 20.09.2021hardik dabasNo ratings yet
- BP Haram Cy CourseDocument2 pagesBP Haram Cy CourseSushmi AsNo ratings yet
- Mohi-ud-Din Islamic Medical College Sector D-4, Mirpur (AJ&K) Application FormDocument2 pagesMohi-ud-Din Islamic Medical College Sector D-4, Mirpur (AJ&K) Application FormUsama TariqNo ratings yet
- Application Form 2020-21 Part-A: Fellowship in General Infectious DiseasesDocument7 pagesApplication Form 2020-21 Part-A: Fellowship in General Infectious DiseasesPrashant PalNo ratings yet
- B.SC., (Nursing) - Original Degree & Migration Application FormDocument3 pagesB.SC., (Nursing) - Original Degree & Migration Application FormGCON KURNOOLNo ratings yet
- Biasiswa 1 PDFDocument6 pagesBiasiswa 1 PDFMOHD. AIDIL FIKRIE BIN AZMIE -No ratings yet
- 2019 PUS Generic Application FormDocument26 pages2019 PUS Generic Application FormGospol MikoziNo ratings yet
- National Institute of Public Health Training & ResearchDocument2 pagesNational Institute of Public Health Training & ResearchQueen1982 KNo ratings yet
- Notification Vizag Steel Plant Medical Horticulture PostsDocument4 pagesNotification Vizag Steel Plant Medical Horticulture PostsRuthvik ReddyNo ratings yet
- GDG Grade IX Registration FormDocument2 pagesGDG Grade IX Registration FormLaksh KalraNo ratings yet
- IITRPhD Application FormDocument4 pagesIITRPhD Application FormVineet SinghNo ratings yet
- (Walk-In-Interview) SR-Website & Advt Copy (Regular) 08.10.2012Document8 pages(Walk-In-Interview) SR-Website & Advt Copy (Regular) 08.10.2012Yogesh DagarNo ratings yet
- PG Diploma ApplicationDocument2 pagesPG Diploma Applicationratna606No ratings yet
- Job DicriptionDocument2 pagesJob DicriptionPranav BhattNo ratings yet
- Application Cum Data SheetDocument2 pagesApplication Cum Data SheetAbhishek FrederickNo ratings yet
- Annexure - For - PGDIE NITIEDocument5 pagesAnnexure - For - PGDIE NITIEIshika PadhyNo ratings yet
- Admission Form July 2010Document4 pagesAdmission Form July 2010haikal1995No ratings yet
- Kishore Vaigyanik Protsahan Yojana - 2011: Application Fo M For Stream SP (Medicine) RDocument6 pagesKishore Vaigyanik Protsahan Yojana - 2011: Application Fo M For Stream SP (Medicine) RAvinash TiwariNo ratings yet
- Indian Institute of Management Sambalpur: June 2020. (Mention: Application For Application FormDocument10 pagesIndian Institute of Management Sambalpur: June 2020. (Mention: Application For Application FormUjjwal MarahattaNo ratings yet
- Centre Fixation Proforma JEE 2016Document4 pagesCentre Fixation Proforma JEE 2016Srini RaoNo ratings yet
- Quality, Technology, InnovationDocument6 pagesQuality, Technology, InnovationRio RioNo ratings yet
- Application Form-IPMI - FinlDocument4 pagesApplication Form-IPMI - FinlRithu SoumyajNo ratings yet
- Medical StudentDocument2 pagesMedical StudentZeeshan HussainNo ratings yet
- 2 Application Form Study in SathyabamaDocument2 pages2 Application Form Study in SathyabamaVENKATESH ALISHAMNo ratings yet
- MINORITIES SEATS For Upload LatestDocument6 pagesMINORITIES SEATS For Upload LatestSikandar ZahoorNo ratings yet
- Brihanmumbai Municipal Corporation: T. N. Medical College & B. Y. L. Nair Ch. Hospital Early Intervention CenterDocument9 pagesBrihanmumbai Municipal Corporation: T. N. Medical College & B. Y. L. Nair Ch. Hospital Early Intervention CenterTushar MeshramNo ratings yet
- Adpcn Membership Form 2018Document2 pagesAdpcn Membership Form 2018Vivi rikka100% (3)
- Indian Institute of Materials ManagementDocument3 pagesIndian Institute of Materials ManagementfaisaldorpNo ratings yet
- Government College of Engineering Kalahandi, BhawanipatnaDocument5 pagesGovernment College of Engineering Kalahandi, BhawanipatnaAditya SinghNo ratings yet
- Vector Control Research Centre: Application For The Post ofDocument3 pagesVector Control Research Centre: Application For The Post ofRamesh AnanthanarayananNo ratings yet
- National Institute of Construction Management and Research: Instructions To CandidateDocument5 pagesNational Institute of Construction Management and Research: Instructions To CandidateUmesh AgrawalNo ratings yet
- MBA MPhil MSC PGD Application FormDocument3 pagesMBA MPhil MSC PGD Application FormKaranGargNo ratings yet
- M.E. Applicatino FormDocument2 pagesM.E. Applicatino FormOmkar SheteNo ratings yet
- Tertiary Education: University Bursary Application FormDocument4 pagesTertiary Education: University Bursary Application Formrcf9658No ratings yet
- Indian Dairy Association: IDA House, Sector IV, R.K. Puram, N. Delhi-22Document2 pagesIndian Dairy Association: IDA House, Sector IV, R.K. Puram, N. Delhi-22Amit Kr GodaraNo ratings yet
- MRCP PacesDocument12 pagesMRCP PacesBilal Khan MarwatNo ratings yet
- Iiae Application FormDocument11 pagesIiae Application FormPalash SwarnakarNo ratings yet
- 2023 Degree Regestration Format-1Document3 pages2023 Degree Regestration Format-1Kiya AbdiNo ratings yet
- Institute of Medical Sciences: Banaras Hindu University VARANASI - 221 005Document4 pagesInstitute of Medical Sciences: Banaras Hindu University VARANASI - 221 005foru007No ratings yet
- FormsMDMS 2010Document12 pagesFormsMDMS 2010Anant BrarNo ratings yet
- All Answers Must Be Given in Words and Not by Dashes and Dots. No Column Should Be Left BlankDocument3 pagesAll Answers Must Be Given in Words and Not by Dashes and Dots. No Column Should Be Left Blankmeripe sureshNo ratings yet
- Resume: Name Permanent Address Phone Numbers E-Mails Web Site Personal Information Objective EducationDocument4 pagesResume: Name Permanent Address Phone Numbers E-Mails Web Site Personal Information Objective EducationPutul MahantaNo ratings yet
- Mmu Solan Prospectus 2018 PDFDocument30 pagesMmu Solan Prospectus 2018 PDFAmrit SainiNo ratings yet
- History of Legal MedicineDocument10 pagesHistory of Legal MedicineLarrymagananNo ratings yet
- Current Residents Faculty 2018Document5 pagesCurrent Residents Faculty 2018Abhishek ChandaNo ratings yet
- Clinical Ophthalmic Oncology Eyelid and Conjunctival Tumors - Jacob Pe'Er Arun D. Singh 3ed 2019Document314 pagesClinical Ophthalmic Oncology Eyelid and Conjunctival Tumors - Jacob Pe'Er Arun D. Singh 3ed 2019Barbara MarcussoNo ratings yet
- CV DR AkpathakDocument3 pagesCV DR AkpathakArupkumar PathakNo ratings yet
- 5 6124922555812807018Document1,044 pages5 6124922555812807018Jennifer Mrj100% (1)
- Insights Into One'S Personal DevelopmentDocument5 pagesInsights Into One'S Personal DevelopmentKristine Angelie Acuña VidadNo ratings yet
- Practical Management of Pediatric Ocular Disorders and Strabismu 2016Document784 pagesPractical Management of Pediatric Ocular Disorders and Strabismu 2016ismkipendprowil2No ratings yet
- Sec. 5, Rule 138, Rules of Court. Sec. 6, RA 2382. 2 Sec. 21, RA 2382. 4Document2 pagesSec. 5, Rule 138, Rules of Court. Sec. 6, RA 2382. 2 Sec. 21, RA 2382. 4Cinja ShidoujiNo ratings yet
- Final PH D Ordinance 2019Document19 pagesFinal PH D Ordinance 2019BKNo ratings yet
- CUVASLARDocument21 pagesCUVASLARKristal MartinezNo ratings yet
- Kle 2008Document43 pagesKle 2008mahesh96% (26)
- 31412Document369 pages31412aptureinc100% (5)
- Program Faculty - Sports MedicineDocument17 pagesProgram Faculty - Sports MedicineKavirNivNo ratings yet
- SICAT - E5-Faculty - FormDocument18 pagesSICAT - E5-Faculty - FormNereo ReoliquioNo ratings yet
- Union Public Service Commission (UPSC) Recruitment 2014 - 159 VacanciesDocument13 pagesUnion Public Service Commission (UPSC) Recruitment 2014 - 159 Vacanciessureshreddy1234No ratings yet
- Clinical Tuberculosis 4th Ed PDFDocument574 pagesClinical Tuberculosis 4th Ed PDFRamonataleNo ratings yet
- BS MD ProgramsDocument1 pageBS MD ProgramsFuego McFuegoNo ratings yet
- National Institute of Health and Family Welfare List of Shortlisted Candidates For Various Post in Nrhm/Rch-IiDocument38 pagesNational Institute of Health and Family Welfare List of Shortlisted Candidates For Various Post in Nrhm/Rch-IiRohit JainNo ratings yet
- The Grants Register 2023 The Complete Guide To Postgraduate Funding Worldwide Palgrave Macmillan Full ChapterDocument67 pagesThe Grants Register 2023 The Complete Guide To Postgraduate Funding Worldwide Palgrave Macmillan Full Chapterheather.shull896100% (6)
- Wilms' Tumor Front MatterDocument14 pagesWilms' Tumor Front MatterAlonso Rodriguez EscobedoNo ratings yet
- Full Download PDF of Comprehensive Review of Infectious Diseases 1st Edition Andrej Spec - Ebook PDF All ChapterDocument69 pagesFull Download PDF of Comprehensive Review of Infectious Diseases 1st Edition Andrej Spec - Ebook PDF All Chapteralasodyeiris100% (4)
- Appendix E - Sponsorship Certificate INI CET PG July 2021 SessionDocument1 pageAppendix E - Sponsorship Certificate INI CET PG July 2021 Sessionudham sudanNo ratings yet
- Letter From Healthcare CommunityDocument4 pagesLetter From Healthcare Community...No ratings yet






















































































Download as pdf or txt
You might also like
- Ebook Hazzards Geriatric Medicine and Gerontology 8Th Ed PDF Full Chapter PDFDocument67 pagesEbook Hazzards Geriatric Medicine and Gerontology 8Th Ed PDF Full Chapter PDFnancy.stice552100% (36)
- Investor Deck - Doctor Insta PDFDocument28 pagesInvestor Deck - Doctor Insta PDFSamarjit Samanta100% (3)
- Shnider and Levinsons Anesthesia For Obstetrics, 5th EdDocument879 pagesShnider and Levinsons Anesthesia For Obstetrics, 5th EdSri Hari50% (2)
- Textbook of Reumathology-Kelley's PDFDocument1,909 pagesTextbook of Reumathology-Kelley's PDFFlorentina Sterghiu100% (4)
- 2.Crcp Application Form 20210114Document2 pages2.Crcp Application Form 20210114Neha GulfamNo ratings yet
- M.e.ph.d Form 2011-12Document9 pagesM.e.ph.d Form 2011-12prakashsahu_84No ratings yet
- E1 E2 E3 E4 FormsDocument8 pagesE1 E2 E3 E4 FormsAbeel IrshadNo ratings yet
- Admission Form BDS 2017-18Document2 pagesAdmission Form BDS 2017-18Shoaib JadoonNo ratings yet
- UTU MTech Application FormDocument6 pagesUTU MTech Application FormAnweshaBoseNo ratings yet
- Adevrtisement Application FormDocument4 pagesAdevrtisement Application FormMùzÃmîl SåMbøråNo ratings yet
- Admission Application Form: Section 1: Personal DataDocument5 pagesAdmission Application Form: Section 1: Personal DatamahmadwasiNo ratings yet
- Indian Maritime University: SL - No.Document4 pagesIndian Maritime University: SL - No.Nivedhitha VivekanandhanNo ratings yet
- Application Form May 2023Document4 pagesApplication Form May 2023derrick andivaNo ratings yet
- Dermatology 1 Pathology, 1 Ophthalmology 1: No of VacancyDocument3 pagesDermatology 1 Pathology, 1 Ophthalmology 1: No of VacancyKirankumar MutnaliNo ratings yet
- Application Form-2019 PDFDocument2 pagesApplication Form-2019 PDFNazneen ShaikNo ratings yet
- O o o o o o o o o o o O: Khyber Medical UniversityDocument3 pagesO o o o o o o o o o o O: Khyber Medical UniversitySobar KhanNo ratings yet
- AdmissionDocument8 pagesAdmissionQuestion BankNo ratings yet
- UERM ApplicationDocument5 pagesUERM ApplicationJasper Benjamin JuradoNo ratings yet
- Bs Medical Technology FormDocument2 pagesBs Medical Technology FormAnonymous CWdCHHSX9qNo ratings yet
- Application For Admission Into APGDEC 2010 - 23.03Document2 pagesApplication For Admission Into APGDEC 2010 - 23.03Sumedh BeleNo ratings yet
- Registration Form: - Fellow - Junior Fellow - Medical Student MemberDocument4 pagesRegistration Form: - Fellow - Junior Fellow - Medical Student MemberWahyu SutrisnaNo ratings yet
- Total Vacant Posts: 100 Last Date For Application: 20.09.2021Document4 pagesTotal Vacant Posts: 100 Last Date For Application: 20.09.2021hardik dabasNo ratings yet
- BP Haram Cy CourseDocument2 pagesBP Haram Cy CourseSushmi AsNo ratings yet
- Mohi-ud-Din Islamic Medical College Sector D-4, Mirpur (AJ&K) Application FormDocument2 pagesMohi-ud-Din Islamic Medical College Sector D-4, Mirpur (AJ&K) Application FormUsama TariqNo ratings yet
- Application Form 2020-21 Part-A: Fellowship in General Infectious DiseasesDocument7 pagesApplication Form 2020-21 Part-A: Fellowship in General Infectious DiseasesPrashant PalNo ratings yet
- B.SC., (Nursing) - Original Degree & Migration Application FormDocument3 pagesB.SC., (Nursing) - Original Degree & Migration Application FormGCON KURNOOLNo ratings yet
- Biasiswa 1 PDFDocument6 pagesBiasiswa 1 PDFMOHD. AIDIL FIKRIE BIN AZMIE -No ratings yet
- 2019 PUS Generic Application FormDocument26 pages2019 PUS Generic Application FormGospol MikoziNo ratings yet
- National Institute of Public Health Training & ResearchDocument2 pagesNational Institute of Public Health Training & ResearchQueen1982 KNo ratings yet
- Notification Vizag Steel Plant Medical Horticulture PostsDocument4 pagesNotification Vizag Steel Plant Medical Horticulture PostsRuthvik ReddyNo ratings yet
- GDG Grade IX Registration FormDocument2 pagesGDG Grade IX Registration FormLaksh KalraNo ratings yet
- IITRPhD Application FormDocument4 pagesIITRPhD Application FormVineet SinghNo ratings yet
- (Walk-In-Interview) SR-Website & Advt Copy (Regular) 08.10.2012Document8 pages(Walk-In-Interview) SR-Website & Advt Copy (Regular) 08.10.2012Yogesh DagarNo ratings yet
- PG Diploma ApplicationDocument2 pagesPG Diploma Applicationratna606No ratings yet
- Job DicriptionDocument2 pagesJob DicriptionPranav BhattNo ratings yet
- Application Cum Data SheetDocument2 pagesApplication Cum Data SheetAbhishek FrederickNo ratings yet
- Annexure - For - PGDIE NITIEDocument5 pagesAnnexure - For - PGDIE NITIEIshika PadhyNo ratings yet
- Admission Form July 2010Document4 pagesAdmission Form July 2010haikal1995No ratings yet
- Kishore Vaigyanik Protsahan Yojana - 2011: Application Fo M For Stream SP (Medicine) RDocument6 pagesKishore Vaigyanik Protsahan Yojana - 2011: Application Fo M For Stream SP (Medicine) RAvinash TiwariNo ratings yet
- Indian Institute of Management Sambalpur: June 2020. (Mention: Application For Application FormDocument10 pagesIndian Institute of Management Sambalpur: June 2020. (Mention: Application For Application FormUjjwal MarahattaNo ratings yet
- Centre Fixation Proforma JEE 2016Document4 pagesCentre Fixation Proforma JEE 2016Srini RaoNo ratings yet
- Quality, Technology, InnovationDocument6 pagesQuality, Technology, InnovationRio RioNo ratings yet
- Application Form-IPMI - FinlDocument4 pagesApplication Form-IPMI - FinlRithu SoumyajNo ratings yet
- Medical StudentDocument2 pagesMedical StudentZeeshan HussainNo ratings yet
- 2 Application Form Study in SathyabamaDocument2 pages2 Application Form Study in SathyabamaVENKATESH ALISHAMNo ratings yet
- MINORITIES SEATS For Upload LatestDocument6 pagesMINORITIES SEATS For Upload LatestSikandar ZahoorNo ratings yet
- Brihanmumbai Municipal Corporation: T. N. Medical College & B. Y. L. Nair Ch. Hospital Early Intervention CenterDocument9 pagesBrihanmumbai Municipal Corporation: T. N. Medical College & B. Y. L. Nair Ch. Hospital Early Intervention CenterTushar MeshramNo ratings yet
- Adpcn Membership Form 2018Document2 pagesAdpcn Membership Form 2018Vivi rikka100% (3)
- Indian Institute of Materials ManagementDocument3 pagesIndian Institute of Materials ManagementfaisaldorpNo ratings yet
- Government College of Engineering Kalahandi, BhawanipatnaDocument5 pagesGovernment College of Engineering Kalahandi, BhawanipatnaAditya SinghNo ratings yet
- Vector Control Research Centre: Application For The Post ofDocument3 pagesVector Control Research Centre: Application For The Post ofRamesh AnanthanarayananNo ratings yet
- National Institute of Construction Management and Research: Instructions To CandidateDocument5 pagesNational Institute of Construction Management and Research: Instructions To CandidateUmesh AgrawalNo ratings yet
- MBA MPhil MSC PGD Application FormDocument3 pagesMBA MPhil MSC PGD Application FormKaranGargNo ratings yet
- M.E. Applicatino FormDocument2 pagesM.E. Applicatino FormOmkar SheteNo ratings yet
- Tertiary Education: University Bursary Application FormDocument4 pagesTertiary Education: University Bursary Application Formrcf9658No ratings yet
- Indian Dairy Association: IDA House, Sector IV, R.K. Puram, N. Delhi-22Document2 pagesIndian Dairy Association: IDA House, Sector IV, R.K. Puram, N. Delhi-22Amit Kr GodaraNo ratings yet
- MRCP PacesDocument12 pagesMRCP PacesBilal Khan MarwatNo ratings yet
- Iiae Application FormDocument11 pagesIiae Application FormPalash SwarnakarNo ratings yet
- 2023 Degree Regestration Format-1Document3 pages2023 Degree Regestration Format-1Kiya AbdiNo ratings yet
- Institute of Medical Sciences: Banaras Hindu University VARANASI - 221 005Document4 pagesInstitute of Medical Sciences: Banaras Hindu University VARANASI - 221 005foru007No ratings yet
- FormsMDMS 2010Document12 pagesFormsMDMS 2010Anant BrarNo ratings yet
- All Answers Must Be Given in Words and Not by Dashes and Dots. No Column Should Be Left BlankDocument3 pagesAll Answers Must Be Given in Words and Not by Dashes and Dots. No Column Should Be Left Blankmeripe sureshNo ratings yet
- Resume: Name Permanent Address Phone Numbers E-Mails Web Site Personal Information Objective EducationDocument4 pagesResume: Name Permanent Address Phone Numbers E-Mails Web Site Personal Information Objective EducationPutul MahantaNo ratings yet
- Mmu Solan Prospectus 2018 PDFDocument30 pagesMmu Solan Prospectus 2018 PDFAmrit SainiNo ratings yet
- History of Legal MedicineDocument10 pagesHistory of Legal MedicineLarrymagananNo ratings yet
- Current Residents Faculty 2018Document5 pagesCurrent Residents Faculty 2018Abhishek ChandaNo ratings yet
- Clinical Ophthalmic Oncology Eyelid and Conjunctival Tumors - Jacob Pe'Er Arun D. Singh 3ed 2019Document314 pagesClinical Ophthalmic Oncology Eyelid and Conjunctival Tumors - Jacob Pe'Er Arun D. Singh 3ed 2019Barbara MarcussoNo ratings yet
- CV DR AkpathakDocument3 pagesCV DR AkpathakArupkumar PathakNo ratings yet
- 5 6124922555812807018Document1,044 pages5 6124922555812807018Jennifer Mrj100% (1)
- Insights Into One'S Personal DevelopmentDocument5 pagesInsights Into One'S Personal DevelopmentKristine Angelie Acuña VidadNo ratings yet
- Practical Management of Pediatric Ocular Disorders and Strabismu 2016Document784 pagesPractical Management of Pediatric Ocular Disorders and Strabismu 2016ismkipendprowil2No ratings yet
- Sec. 5, Rule 138, Rules of Court. Sec. 6, RA 2382. 2 Sec. 21, RA 2382. 4Document2 pagesSec. 5, Rule 138, Rules of Court. Sec. 6, RA 2382. 2 Sec. 21, RA 2382. 4Cinja ShidoujiNo ratings yet
- Final PH D Ordinance 2019Document19 pagesFinal PH D Ordinance 2019BKNo ratings yet
- CUVASLARDocument21 pagesCUVASLARKristal MartinezNo ratings yet
- Kle 2008Document43 pagesKle 2008mahesh96% (26)
- 31412Document369 pages31412aptureinc100% (5)
- Program Faculty - Sports MedicineDocument17 pagesProgram Faculty - Sports MedicineKavirNivNo ratings yet
- SICAT - E5-Faculty - FormDocument18 pagesSICAT - E5-Faculty - FormNereo ReoliquioNo ratings yet
- Union Public Service Commission (UPSC) Recruitment 2014 - 159 VacanciesDocument13 pagesUnion Public Service Commission (UPSC) Recruitment 2014 - 159 Vacanciessureshreddy1234No ratings yet
- Clinical Tuberculosis 4th Ed PDFDocument574 pagesClinical Tuberculosis 4th Ed PDFRamonataleNo ratings yet
- BS MD ProgramsDocument1 pageBS MD ProgramsFuego McFuegoNo ratings yet
- National Institute of Health and Family Welfare List of Shortlisted Candidates For Various Post in Nrhm/Rch-IiDocument38 pagesNational Institute of Health and Family Welfare List of Shortlisted Candidates For Various Post in Nrhm/Rch-IiRohit JainNo ratings yet
- The Grants Register 2023 The Complete Guide To Postgraduate Funding Worldwide Palgrave Macmillan Full ChapterDocument67 pagesThe Grants Register 2023 The Complete Guide To Postgraduate Funding Worldwide Palgrave Macmillan Full Chapterheather.shull896100% (6)
- Wilms' Tumor Front MatterDocument14 pagesWilms' Tumor Front MatterAlonso Rodriguez EscobedoNo ratings yet
- Full Download PDF of Comprehensive Review of Infectious Diseases 1st Edition Andrej Spec - Ebook PDF All ChapterDocument69 pagesFull Download PDF of Comprehensive Review of Infectious Diseases 1st Edition Andrej Spec - Ebook PDF All Chapteralasodyeiris100% (4)
- Appendix E - Sponsorship Certificate INI CET PG July 2021 SessionDocument1 pageAppendix E - Sponsorship Certificate INI CET PG July 2021 Sessionudham sudanNo ratings yet
- Letter From Healthcare CommunityDocument4 pagesLetter From Healthcare Community...No ratings yet