Download as pdf or txt
You might also like
- Diagnostic Exam Nov 24Document25 pagesDiagnostic Exam Nov 24genita.keziahandrea100% (1)
- Chapter 1 - Bess GaskellDocument8 pagesChapter 1 - Bess GaskellEunice CortésNo ratings yet
- Argumentative Essay About Anti-VaxxersShould A COVID-19 Vaccine Be MandatoryDocument1 pageArgumentative Essay About Anti-VaxxersShould A COVID-19 Vaccine Be MandatoryAzril owayetNo ratings yet
- Infection Control Competency QuizDocument7 pagesInfection Control Competency QuizLoo DrBrad100% (1)
- Report of Medical Examination and Vaccination RecordDocument14 pagesReport of Medical Examination and Vaccination RecordHrishi WaghNo ratings yet
- LG-14 Important Health Programs CDDDocument20 pagesLG-14 Important Health Programs CDDMazinNo ratings yet
- Summary of IMCI Case ManagementDocument2 pagesSummary of IMCI Case Managementjanesky09100% (1)
- Appendix 11. Flow Chart For Cholera Case ManagementDocument1 pageAppendix 11. Flow Chart For Cholera Case ManagementGerard Pio Wee100% (2)
- Pediatric em 2Document28 pagesPediatric em 2bhupeshwariNo ratings yet
- TRANS - Dehydration & RehydrationDocument3 pagesTRANS - Dehydration & RehydrationRencel Hope BañezNo ratings yet
- Sudan IMCI 2.pptx CCDocument55 pagesSudan IMCI 2.pptx CCabdiqadir ali adanNo ratings yet
- World Health Organization: WHO/CDD/SER/91.15 REV.1Document10 pagesWorld Health Organization: WHO/CDD/SER/91.15 REV.1IjafiyaNo ratings yet
- Diarrhea Is Derived From Greek Word, Meaning 'Flowing Through'. It Is The Second Leading Cause of Death in Children Under 5 Years of AgeDocument12 pagesDiarrhea Is Derived From Greek Word, Meaning 'Flowing Through'. It Is The Second Leading Cause of Death in Children Under 5 Years of AgefitahsinghNo ratings yet
- Case Report Diarrhea: Adviser By: Dr. Alfred, Sp. A Writen By: Meylinda (1261050133)Document18 pagesCase Report Diarrhea: Adviser By: Dr. Alfred, Sp. A Writen By: Meylinda (1261050133)Norma Diona PurbaNo ratings yet
- Conditions of The GITTDocument4 pagesConditions of The GITTPGDME 20192020No ratings yet
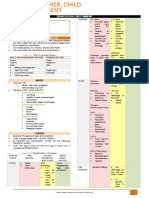
- Integrated Management of Childhood Illness: Chart BookletDocument81 pagesIntegrated Management of Childhood Illness: Chart BookletReadcast EFNo ratings yet
- Integrated Management of Childhood IllnessesDocument65 pagesIntegrated Management of Childhood IllnessesJocel LañasNo ratings yet
- Integrated Management of Childhood IllnessesDocument11 pagesIntegrated Management of Childhood IllnessesSophia BarnesNo ratings yet
- CPG Acute Infectious Diarrhea Pocket Guide v2Document21 pagesCPG Acute Infectious Diarrhea Pocket Guide v2Moonyeen Jann Casera BalicNo ratings yet
- د. علي الزيدي Diarrhea-1 (Muhadharaty)Document47 pagesد. علي الزيدي Diarrhea-1 (Muhadharaty)aaaNo ratings yet
- Diarrhea 180822082356Document12 pagesDiarrhea 180822082356Prateek Singh100% (1)
- Dehydration in Peads: Nora Edora Francis PPW 23, Etd Hqe 2Document16 pagesDehydration in Peads: Nora Edora Francis PPW 23, Etd Hqe 2Maman GundohingNo ratings yet
- MalnutritionDocument7 pagesMalnutritionKookia BatoromaioNo ratings yet
- Diarrhea PediaDocument10 pagesDiarrhea PediaSuneeth Kumar MohantyNo ratings yet
- AGE MarchDocument46 pagesAGE MarchJefelson Eu Palaña NahidNo ratings yet
- Case ManagementDocument78 pagesCase ManagementSeyfNo ratings yet
- Diarrheal Diseases in ChildrenDocument16 pagesDiarrheal Diseases in ChildrenNupur SharmaNo ratings yet
- CEM7213 Bronchiolitis Pathway Acute Care West Sussex Oct 2011Document2 pagesCEM7213 Bronchiolitis Pathway Acute Care West Sussex Oct 2011drgrizahNo ratings yet
- Outline: (Trans) Lesson 4: Imci SummaryDocument2 pagesOutline: (Trans) Lesson 4: Imci SummaryAbish Julienne PecundoNo ratings yet
- Sick Young Infants (Referral, Treatment, Oral Drugs) : ImnciDocument46 pagesSick Young Infants (Referral, Treatment, Oral Drugs) : ImnciTanviNo ratings yet
- Care of The Child With Gastrointestinal Dysfunction: Betsy Johnson, MSN, CPNP-PCDocument66 pagesCare of The Child With Gastrointestinal Dysfunction: Betsy Johnson, MSN, CPNP-PCGelsey Gelsinator JianNo ratings yet
- Literature ReviewDocument23 pagesLiterature ReviewSyMaryamHaninaNo ratings yet
- GE in ChildrenDocument23 pagesGE in ChildrensamiNo ratings yet
- DehydrationDocument23 pagesDehydrationEusebius01No ratings yet
- Epidemiology and Control of Acute Diarrheal Diseases: Dr. Anish KhannaDocument21 pagesEpidemiology and Control of Acute Diarrheal Diseases: Dr. Anish KhannaHans Chester Rirao CapindingNo ratings yet
- National Control of Dirrheal Diseases (CDD) Program ObjectivesDocument6 pagesNational Control of Dirrheal Diseases (CDD) Program ObjectivesJoy FucananNo ratings yet
- NCP Leptospirosis - NewDocument5 pagesNCP Leptospirosis - Newglaiza_requintoNo ratings yet
- Nursing Care Plan Cues Diagnosis Justification: Sodium-132 Mmol/l (Low)Document3 pagesNursing Care Plan Cues Diagnosis Justification: Sodium-132 Mmol/l (Low)rei_alina75% (4)
- NCP For Deficient Fluid VolumeDocument2 pagesNCP For Deficient Fluid VolumeRedwing_Dc_854758% (12)
- Acute Diarrheal Diseases: Dr. Priyanka SachdevaDocument45 pagesAcute Diarrheal Diseases: Dr. Priyanka SachdevapriyankaNo ratings yet
- Care of The Child Applying Integrated Management of Childhood Illnesses (Imci)Document22 pagesCare of The Child Applying Integrated Management of Childhood Illnesses (Imci)Jesena SalveNo ratings yet
- CPG On AID PPT PresentationDocument83 pagesCPG On AID PPT Presentationsharmaine peroNo ratings yet
- Diarrhea in ChildrenDocument69 pagesDiarrhea in ChildrenNishita True SpiritNo ratings yet
- MaxineDocument19 pagesMaxinefaithdejamo2No ratings yet
- The Mcmaster Pediatric Curriculum: at NightDocument29 pagesThe Mcmaster Pediatric Curriculum: at NightFrancia ToledanoNo ratings yet
- 104 Theorle Finals PointersDocument7 pages104 Theorle Finals PointersSudaea AgacerNo ratings yet
- DR Mwanzas Pediatric Protocols 2017Document143 pagesDR Mwanzas Pediatric Protocols 2017Mwambazi MathewsNo ratings yet
- Imci Summary Toprank by JadeDocument13 pagesImci Summary Toprank by JadeJade SorongonNo ratings yet
- IMCI SumDocument6 pagesIMCI SumLazo JuleeNo ratings yet
- Approach To A Child With DiarrheaDocument28 pagesApproach To A Child With DiarrheaUmair QasimNo ratings yet
- Nursing Care Plan 1 - DiarrheaDocument7 pagesNursing Care Plan 1 - DiarrheakirbyroohNo ratings yet
- IMCI Management 2m-5yearsDocument35 pagesIMCI Management 2m-5yearsRachanaNo ratings yet
- Diarrhea in ChildrenDocument42 pagesDiarrhea in ChildrenIPNATC NEPALNo ratings yet
- CholeraDocument1 pageCholeraRevan NasirNo ratings yet
- IMCIDocument17 pagesIMCIapi-3707883No ratings yet
- ch2 fs1Document2 pagesch2 fs1ry beNo ratings yet
- General Tonic Monograph and Pharmacology Shi Quan Da Bu WanDocument8 pagesGeneral Tonic Monograph and Pharmacology Shi Quan Da Bu WanrikiNo ratings yet
- Case ReportDocument27 pagesCase ReportRuni ArumndariNo ratings yet
- Diarrhea AnilDocument52 pagesDiarrhea Anilanil sahNo ratings yet
- Dermatitis Herpetiformis: A Concise Guide to Causes, Tests and Treatment OptionsFrom EverandDermatitis Herpetiformis: A Concise Guide to Causes, Tests and Treatment OptionsNo ratings yet
- Soak It In: Hydrotherapy Treatments In 20 Minutes or Less for Health and BeautyFrom EverandSoak It In: Hydrotherapy Treatments In 20 Minutes or Less for Health and BeautyNo ratings yet
- 73. Vaishnavi HospitalDocument17 pages73. Vaishnavi HospitalDevil DevilNo ratings yet
- Patient Registration Form - 1284034 - 27-02-2022Document1 pagePatient Registration Form - 1284034 - 27-02-2022Devil DevilNo ratings yet
- NEET 2023 Solutions Code E2Document55 pagesNEET 2023 Solutions Code E2Devil DevilNo ratings yet
- NEET 2023 Question Paper Code E2Document32 pagesNEET 2023 Question Paper Code E2Devil DevilNo ratings yet
- 01june2019 EEJ IAINDocument17 pages01june2019 EEJ IAINDevil DevilNo ratings yet
- 28-Randomised Controlled Trial-YangBF 09.5.12Document14 pages28-Randomised Controlled Trial-YangBF 09.5.12sanjivdasNo ratings yet
- Cohort Study: Dr. Rahul Netragaonkar Associate ProfessorDocument37 pagesCohort Study: Dr. Rahul Netragaonkar Associate ProfessorRahul NetragaonkarNo ratings yet
- HIV Related LawsDocument7 pagesHIV Related LawsRMNo ratings yet
- REV Skripsi LR Hubungan Pemberian ASIE DG Kejadian Stunting PD Bad YWKAe5GDocument89 pagesREV Skripsi LR Hubungan Pemberian ASIE DG Kejadian Stunting PD Bad YWKAe5GFauziyah AnnisaaNo ratings yet
- eZH Ealth: Dosage Seq. Date (Mm/dd/yyyy) Vaccine Brand Name of Vaccinator Batch No. Lot NoDocument1 pageeZH Ealth: Dosage Seq. Date (Mm/dd/yyyy) Vaccine Brand Name of Vaccinator Batch No. Lot NoRvBombetaNo ratings yet
- Genital Tract InfectionsDocument1 pageGenital Tract InfectionsKatrina TaracatacNo ratings yet
- Bilateral Coperation in Health ManualDocument30 pagesBilateral Coperation in Health ManualHussen AbdulmenanNo ratings yet
- Vaginal Breech Delivery at Term and Neonatal Morbidity and Mortality - A Population-Based Cohort Study in SwedenDocument17 pagesVaginal Breech Delivery at Term and Neonatal Morbidity and Mortality - A Population-Based Cohort Study in SwedenRegina SeptianaNo ratings yet
- G2 Basic Sanitation Action PlanDocument3 pagesG2 Basic Sanitation Action PlanDontogan BarangayNo ratings yet
- Recommendation FormsDocument5 pagesRecommendation FormsRezi Sabutanan AmerilaNo ratings yet
- MCN Questionnaire DraftDocument8 pagesMCN Questionnaire DraftJenny AjocNo ratings yet
- PFAS in Drinking WaterDocument2 pagesPFAS in Drinking WaterWDET 101.9 FMNo ratings yet
- Week 29 - DRRRDocument5 pagesWeek 29 - DRRRMira VeranoNo ratings yet
- 2183 9417 Nas 31 03 206Document6 pages2183 9417 Nas 31 03 206VITOR HUGO PEREZNo ratings yet
- Philippine College of Occupational Medicine, Inc.: Phil M. Pangilinan, MD, Mha, FPSMS, Dpcom, PafpDocument3 pagesPhilippine College of Occupational Medicine, Inc.: Phil M. Pangilinan, MD, Mha, FPSMS, Dpcom, PafpANNLNo ratings yet
- Colorado Road Map For In-Person Learning: Letter To TeachersDocument4 pagesColorado Road Map For In-Person Learning: Letter To TeachersMichael_Roberts2019No ratings yet
- Call To Action For Contraceptive SafetyDocument16 pagesCall To Action For Contraceptive SafetyPopulation & Development Program (PopDev)No ratings yet
- FGBFRHTH Reduce 1 PDFDocument385 pagesFGBFRHTH Reduce 1 PDFAbu Abid Al-FatihNo ratings yet
- Cervicitis Symptoms, Treatment, Causes & TypesDocument1 pageCervicitis Symptoms, Treatment, Causes & Typesramit singlaNo ratings yet
- No Rinse Food Contact Cleaner Sanitizer PDFDocument2 pagesNo Rinse Food Contact Cleaner Sanitizer PDFJaime Lagos BorquezNo ratings yet
- Developing Political CompetenceDocument6 pagesDeveloping Political CompetencernrmmanphdNo ratings yet
- Australia Digital Passenger Declaration (DPD)Document2 pagesAustralia Digital Passenger Declaration (DPD)Anish bhandariNo ratings yet
- Serological Response To Myxomatosis Vaccination by Different Inoculations Systems On Farm RabbitsDocument12 pagesSerological Response To Myxomatosis Vaccination by Different Inoculations Systems On Farm RabbitsCamilaNo ratings yet
- Ovarian Cancer Prevention and Screening.22Document19 pagesOvarian Cancer Prevention and Screening.22tri erdiansyahNo ratings yet
- Sentinel-Event Root Cause Analysis RCADocument11 pagesSentinel-Event Root Cause Analysis RCAavsuNo ratings yet