
2020 Article 69328
2020 Article 69328
You might also like
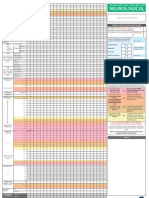
- Adult Early Warning Score Observation Chart For Neurosurgical UnitDocument1 pageAdult Early Warning Score Observation Chart For Neurosurgical UnitalexipsNo ratings yet
- Basic Pathology - An Introduction To The Mechanisms of Disease (PDFDrive)Document340 pagesBasic Pathology - An Introduction To The Mechanisms of Disease (PDFDrive)edo58No ratings yet
- Infograph Eatingdisorders Rubric1Document2 pagesInfograph Eatingdisorders Rubric1api-296522338No ratings yet
- Pathophysiology of Hepatitis BDocument9 pagesPathophysiology of Hepatitis BDianne G Ignacio100% (4)
- Identi Fication of Synovial Fluid Biomarkers For Knee Osteoarthritis and Correlation With Radiographic AssessmentDocument6 pagesIdenti Fication of Synovial Fluid Biomarkers For Knee Osteoarthritis and Correlation With Radiographic AssessmentIndraYudhiNo ratings yet
- WOMAC Osteoarthritis Index-Additional Dimensions For Use in Subjects With Post-Traumatic Osteoarthritis of The KneeDocument6 pagesWOMAC Osteoarthritis Index-Additional Dimensions For Use in Subjects With Post-Traumatic Osteoarthritis of The KneeDian MuslimahNo ratings yet
- Efficacy and Safety of Avocado Soybean Unsaponifiables For The Treatment of Hip and Knee Osteoarthritis - A Systematic Review and Meta Analysis of Randomized Placebo Controlled TrialsDocument10 pagesEfficacy and Safety of Avocado Soybean Unsaponifiables For The Treatment of Hip and Knee Osteoarthritis - A Systematic Review and Meta Analysis of Randomized Placebo Controlled Trialsabo_youssof20047438No ratings yet
- Type 2 Diabetes Mellitus Is Associated With Increased Risks of Sarcopenia and Pre-Sarcopenia in Chinese ElderlyDocument7 pagesType 2 Diabetes Mellitus Is Associated With Increased Risks of Sarcopenia and Pre-Sarcopenia in Chinese ElderlyYafanita IzzatiNo ratings yet
- Psoas Muscle Index and Psoas Density As Predictors of Mortality in HaemodialysisDocument8 pagesPsoas Muscle Index and Psoas Density As Predictors of Mortality in HaemodialysisSvt Mscofficial2No ratings yet
- Corneal Thickness in An Ophthalmologically Normal Japanese PopulationDocument10 pagesCorneal Thickness in An Ophthalmologically Normal Japanese PopulationAndreas SimatupangNo ratings yet
- SCRIPTA SCORE Scientific Medical Journal Vol 2 No 1 OnlineDocument73 pagesSCRIPTA SCORE Scientific Medical Journal Vol 2 No 1 Online292Vien HardiyantiNo ratings yet
- A Study of Cartilage Oligomeric Matrix Protein (Comp) & Tumor Necrosis Factor - in Post Menopausal Knee Osteoarthritic Female Patient.Document4 pagesA Study of Cartilage Oligomeric Matrix Protein (Comp) & Tumor Necrosis Factor - in Post Menopausal Knee Osteoarthritic Female Patient.IJAR JOURNALNo ratings yet
- Resumo - SIICUSP - Ingles FinalDocument2 pagesResumo - SIICUSP - Ingles FinalSuel CostaNo ratings yet
- Primary Knee Arthroplasty For Osteoarthritis Restores Patients' Health-Related Quality of Life To Normal Population LevelsDocument8 pagesPrimary Knee Arthroplasty For Osteoarthritis Restores Patients' Health-Related Quality of Life To Normal Population LevelsShiv KolheNo ratings yet
- Arth2011 580632Document6 pagesArth2011 580632hylee102594No ratings yet
- 151 Effects of Physiotherapy Treatment On Knee Oa Gai 2009 Osteoarthritis AnDocument2 pages151 Effects of Physiotherapy Treatment On Knee Oa Gai 2009 Osteoarthritis AnEmad Tawfik AhmadNo ratings yet
- 1 EndometriozaDocument33 pages1 EndometriozaMandici ConstantinNo ratings yet
- Posters (Third Part) : SciencedirectDocument2 pagesPosters (Third Part) : SciencedirectshewaleakhileshNo ratings yet
- Neu 2021 0351Document9 pagesNeu 2021 0351divinechp07No ratings yet
- A Naturally Aging Knee or Development of Early KN - 2018 - Osteoarthritis and CDocument6 pagesA Naturally Aging Knee or Development of Early KN - 2018 - Osteoarthritis and CVanessa MartinsNo ratings yet
- Dir-23-5-385 VickyDocument5 pagesDir-23-5-385 Vickyvicky jessicauNo ratings yet
- Evaluation of The Kinematic Parameters of Normal-Paced Gait in Subjects With Gonarthrosis and The Influence of Gonarthrosis On The Function of The Ankle Joint and Hip JointDocument8 pagesEvaluation of The Kinematic Parameters of Normal-Paced Gait in Subjects With Gonarthrosis and The Influence of Gonarthrosis On The Function of The Ankle Joint and Hip JointRaluca ZamfirescuNo ratings yet
- 7225 39494 1 PBDocument9 pages7225 39494 1 PBBainaka De-LavangéarNo ratings yet
- A Novel Method For Assessing Postoperative Femoral Head Reduction in Developmental Dysplasia of The HipDocument6 pagesA Novel Method For Assessing Postoperative Femoral Head Reduction in Developmental Dysplasia of The HipmicNo ratings yet
- Kerangka Konsep PenelitianDocument29 pagesKerangka Konsep PenelitianGabriel KlemensNo ratings yet
- BMM 13 5Document7 pagesBMM 13 5zeravoneNo ratings yet
- Jpts 26 629Document3 pagesJpts 26 629Evelin HanaNo ratings yet
- Admin, Ahmad MulyadiDocument6 pagesAdmin, Ahmad MulyadiDinda SaviraNo ratings yet
- cc161 1Document6 pagescc161 1Hamza AhmedNo ratings yet
- Oarsi 2Document3 pagesOarsi 2Mohd Yusof BaharuddinNo ratings yet
- Body Mass Index and Susceptibility To Knee Osteoarthritis: A Systematic Review and Meta-AnalysisDocument7 pagesBody Mass Index and Susceptibility To Knee Osteoarthritis: A Systematic Review and Meta-AnalysisAmalia RosaNo ratings yet
- Prevalence of Glaucoma in India: A Review: Ronnie George, Lingam VijayaDocument5 pagesPrevalence of Glaucoma in India: A Review: Ronnie George, Lingam VijayaprinceamitNo ratings yet
- 1756-185X.13082) Huang, Lanfeng Guo, Bin Xu, Feixiang Zhao, Jinsong - Effects of Quadriceps Functional Exercise With IsDocument8 pages1756-185X.13082) Huang, Lanfeng Guo, Bin Xu, Feixiang Zhao, Jinsong - Effects of Quadriceps Functional Exercise With IsTrisna ArinataNo ratings yet
- Diagnosing OsteomyelitisDocument12 pagesDiagnosing Osteomyelitisna huNo ratings yet
- La Eficacia de Los Biomarcadores de Muerte Celular en Suero para Diagnosticar El Cáncer Del Tracto BiliarDocument7 pagesLa Eficacia de Los Biomarcadores de Muerte Celular en Suero para Diagnosticar El Cáncer Del Tracto BiliarNicolás MateoJrNo ratings yet
- Manifestaciones Clinicas de OsteoartritisDocument10 pagesManifestaciones Clinicas de OsteoartritisMeny GarciaNo ratings yet
- Muscular and Functional Capacity in Subjects Under TreatmentDocument7 pagesMuscular and Functional Capacity in Subjects Under Treatmentdavid fernandezNo ratings yet
- Faktor Risiko Hemoroid Korea NatureDocument9 pagesFaktor Risiko Hemoroid Korea NatureRatu AstridNo ratings yet
- Knee Osteo ArthritisDocument9 pagesKnee Osteo ArthritisSondang SamosirNo ratings yet
- Jurnal 5Document5 pagesJurnal 5Devita SanangkaNo ratings yet
- Zwad 229Document11 pagesZwad 229VaniNo ratings yet
- (2023) Effects of Running On The Development of Knee OsteoarthritisDocument6 pages(2023) Effects of Running On The Development of Knee Osteoarthritiscalixto1995No ratings yet
- Lateral Spine Backbone: Scoliosis: Sideways (Document3 pagesLateral Spine Backbone: Scoliosis: Sideways (khangkhungkhernitxNo ratings yet
- Biomarkers of Neutrophil Extracellular Traps NETsDocument10 pagesBiomarkers of Neutrophil Extracellular Traps NETsFriNo ratings yet
- PDF 8Document11 pagesPDF 8Amina GoharyNo ratings yet
- Age and Sex Specific Reference Intervals For Blood Urea Nitrogen in Chinese General PopulationDocument7 pagesAge and Sex Specific Reference Intervals For Blood Urea Nitrogen in Chinese General PopulationVarna AmaliaNo ratings yet
- Zwad 229Document11 pagesZwad 229Rizky AisNo ratings yet
- Osteoporosis and Osteoarthritis 2011 ConferenceDocument39 pagesOsteoporosis and Osteoarthritis 2011 ConferencetarikeopsNo ratings yet
- Comparison of Functional Disability in Patients of Knee Osteoarthritis (KOA), Among Rural and Urban KOA PatientsDocument11 pagesComparison of Functional Disability in Patients of Knee Osteoarthritis (KOA), Among Rural and Urban KOA PatientsInternational Health ReviewNo ratings yet
- بحث الثاني كامل copyDocument9 pagesبحث الثاني كامل copyasmarafie289No ratings yet
- Animals 14 00986Document11 pagesAnimals 14 00986andreza.beatrizNo ratings yet
- Medical Review: Medicinska RevijaDocument5 pagesMedical Review: Medicinska RevijaNikolina Nina MileticNo ratings yet
- Effect of The Site of Measurement of Waist Circumference On The Prevalence of The Metabolic SyndromeDocument5 pagesEffect of The Site of Measurement of Waist Circumference On The Prevalence of The Metabolic SyndromeAngie OsorioNo ratings yet
- 2018 The Learning Curve Associated With Robotic-Arm Assisted Unicompartmental Knee Arthroplasty - A Prospective Cohort StudyDocument10 pages2018 The Learning Curve Associated With Robotic-Arm Assisted Unicompartmental Knee Arthroplasty - A Prospective Cohort Studysumon.huqNo ratings yet
- Acute Effect of Partial Body Weight Suspension On The Level of Cocontraction and Gait Biomechanics in Women With Knee OsteoarthritisDocument9 pagesAcute Effect of Partial Body Weight Suspension On The Level of Cocontraction and Gait Biomechanics in Women With Knee OsteoarthritisSango AyraNo ratings yet
- Journal of Taibah University Medical SciencesDocument7 pagesJournal of Taibah University Medical SciencesIlham Amal MNo ratings yet
- Maturitas: SciencedirectDocument6 pagesMaturitas: Sciencedirectaeroforce20No ratings yet
- Outcomes of Systemic Lupus Erythematosus in Patients Who DiscontinueDocument7 pagesOutcomes of Systemic Lupus Erythematosus in Patients Who DiscontinueirsyadilfikriNo ratings yet
- Vertebral Fracture Risk (VFR) Score For Fracture Prediction in Postmenopausal WomenDocument11 pagesVertebral Fracture Risk (VFR) Score For Fracture Prediction in Postmenopausal WomenAdhiatma DotNo ratings yet
- Mascle Mass Measurement Using ML With MEGDocument14 pagesMascle Mass Measurement Using ML With MEGfuyaratasnimNo ratings yet
- Pereira 2015Document9 pagesPereira 2015Amalia RosaNo ratings yet
- Sindrome de GitelmanDocument7 pagesSindrome de GitelmanHenry Perugachi MendezNo ratings yet
- Association of Radiographic Severity of LumbarDocument2 pagesAssociation of Radiographic Severity of LumbarSumanta KamilaNo ratings yet
- Recent Advances of Sarcopenia and Frailty in CKDFrom EverandRecent Advances of Sarcopenia and Frailty in CKDAkihiko KatoNo ratings yet
- Developments in Stem Cell Derived Islet Replacement Therapy F - 2023 - Cell StemDocument19 pagesDevelopments in Stem Cell Derived Islet Replacement Therapy F - 2023 - Cell Stemdimiz77No ratings yet
- SPMBS1785Document4 pagesSPMBS1785dimiz77No ratings yet
- Clonally Resolved Single Cell Multi Omics Identifies Routes of 2023 Cell STDocument25 pagesClonally Resolved Single Cell Multi Omics Identifies Routes of 2023 Cell STdimiz77No ratings yet
- Dyspareunia - StatPearls - NCBI BookshelfDocument6 pagesDyspareunia - StatPearls - NCBI Bookshelfdimiz77No ratings yet
- 2016 Article 873Document15 pages2016 Article 873dimiz77No ratings yet
- Shantipriya Reddy, Enhancing Palatal Wound HealingDocument3 pagesShantipriya Reddy, Enhancing Palatal Wound Healingdimiz77No ratings yet
- Ed Ling 2018Document43 pagesEd Ling 2018dimiz77No ratings yet
- Biomed Res Int 2014 Tunali 209548Document7 pagesBiomed Res Int 2014 Tunali 209548dimiz77No ratings yet
- Astm. .D7246Document3 pagesAstm. .D7246dimiz77No ratings yet
- Spmbs 1805Document4 pagesSpmbs 1805dimiz77No ratings yet
- Park 2013Document10 pagesPark 2013dimiz77No ratings yet
- 1 s2.0 S0022202X15404245 MainDocument11 pages1 s2.0 S0022202X15404245 Maindimiz77No ratings yet
- PRISYM Labels Ensuring Quality Labels GuideDocument1 pagePRISYM Labels Ensuring Quality Labels Guidedimiz77No ratings yet
- Aps 43 430 2Document8 pagesAps 43 430 2dimiz77No ratings yet
- Biomed Clear Sterilization Results-5Document6 pagesBiomed Clear Sterilization Results-5dimiz77No ratings yet
- Usdm Vap Accelerator Pack MedDocument2 pagesUsdm Vap Accelerator Pack Meddimiz77No ratings yet
- 2022 Article 435-3Document10 pages2022 Article 435-3dimiz77No ratings yet
- Corp Catalog Digital All Updated 040523Document97 pagesCorp Catalog Digital All Updated 040523dimiz77No ratings yet
- Bartender Robar Case Study Zimmer BiometDocument2 pagesBartender Robar Case Study Zimmer Biometdimiz77No ratings yet
- Restigen Package InsertDocument2 pagesRestigen Package Insertdimiz77No ratings yet
- Multiple Faces of Succinate Beyond Metabolism in Blood: Review ArticleDocument7 pagesMultiple Faces of Succinate Beyond Metabolism in Blood: Review Articledimiz77No ratings yet
- Zha Image-Brochure GB RMF Reduced-2Document18 pagesZha Image-Brochure GB RMF Reduced-2dimiz77No ratings yet
- Method of Analysis For Sodium Citrate: PharmaguidelineDocument3 pagesMethod of Analysis For Sodium Citrate: Pharmaguidelinedimiz77No ratings yet
- Analysis of Citrate Content in Bone Using High Performance LiquidDocument268 pagesAnalysis of Citrate Content in Bone Using High Performance Liquiddimiz77No ratings yet
- Sensitive Ion Chromatographic Determination of CitDocument10 pagesSensitive Ion Chromatographic Determination of Citdimiz77No ratings yet
- AstroHood S III CSHT AFP CS 107ADocument2 pagesAstroHood S III CSHT AFP CS 107Adimiz77No ratings yet
- 669-Manuscript Text-2748-1-10-20090527Document5 pages669-Manuscript Text-2748-1-10-20090527dimiz77No ratings yet
- PSR1000Document2 pagesPSR1000dimiz77No ratings yet
- MAC-T Grid System Brochure - 0518Document4 pagesMAC-T Grid System Brochure - 0518dimiz77No ratings yet
- Akustik - Border: Akustik - Border Is The L-Shaped' Band To Be Easily Installed On The Perimetrical WallsDocument1 pageAkustik - Border: Akustik - Border Is The L-Shaped' Band To Be Easily Installed On The Perimetrical Wallsdimiz77No ratings yet
- Product Bulletin - NutriferonDocument2 pagesProduct Bulletin - Nutriferonshaklee480No ratings yet
- Fresh Frozen Plasma Transfusion - Guideline For PracticeDocument16 pagesFresh Frozen Plasma Transfusion - Guideline For PracticeMohd Anas SheikhNo ratings yet
- 4 5920472882638490310 Removed RemovedDocument97 pages4 5920472882638490310 Removed Removedsameena vNo ratings yet
- Drug ClassificationsDocument3 pagesDrug ClassificationsLaura Hernandez100% (3)
- PEDIA RLE Multiple Case Studies - 2Document4 pagesPEDIA RLE Multiple Case Studies - 2R-Chian Jose GermanpNo ratings yet
- Complication During PregnancyDocument43 pagesComplication During PregnancyRizza Domalaon BalangitanNo ratings yet
- Atangen CHN Journal CariagaDocument2 pagesAtangen CHN Journal CariagaTyn TynNo ratings yet
- Informasi Produk Azithromycin 0.5 G InjDocument22 pagesInformasi Produk Azithromycin 0.5 G InjVirghost14 WNo ratings yet
- Demystifying Viral Anterior Uveitis: A Review: Nicole Shu-Wen Chan Mbbs - Soon-Phaik Chee Frcophth Mmed (S'Pore)Document14 pagesDemystifying Viral Anterior Uveitis: A Review: Nicole Shu-Wen Chan Mbbs - Soon-Phaik Chee Frcophth Mmed (S'Pore)Dr Pranesh BalasubramaniamNo ratings yet
- Done Don't Need - Physical Exam TipsDocument3 pagesDone Don't Need - Physical Exam Tipskabal321No ratings yet
- Association of Microbiome With Oral Squamous CellDocument21 pagesAssociation of Microbiome With Oral Squamous CellGhimpu DanielaNo ratings yet
- Polycrest RemediesDocument2 pagesPolycrest RemediesMd. NazimNo ratings yet
- Format For Clinical and Family Case PresentationDocument4 pagesFormat For Clinical and Family Case PresentationCATHERINE HAYNESNo ratings yet
- Middle Meatal AntrostomyDocument2 pagesMiddle Meatal AntrostomymajidjankakakhelNo ratings yet
- 4.2.2 Risk Factors of Breast Cancer Among Women A Meta AnalysisDocument15 pages4.2.2 Risk Factors of Breast Cancer Among Women A Meta AnalysisNoob KidNo ratings yet
- Drug Study - Amiodaron HydrochlorideDocument4 pagesDrug Study - Amiodaron HydrochlorideTwinkle SalongaNo ratings yet
- Course Task 4 - Thrombophlebitis (De Jesus, LG E.)Document2 pagesCourse Task 4 - Thrombophlebitis (De Jesus, LG E.)LOVELLE GRACE DE JESUSNo ratings yet
- MPT - 1 Year Question Paper (Physical and Functional Diag.)Document10 pagesMPT - 1 Year Question Paper (Physical and Functional Diag.)aishp2897No ratings yet
- Abnormal Uterine Bleeding TreatmentDocument6 pagesAbnormal Uterine Bleeding TreatmentdrdivyakumargynaecNo ratings yet
- Polien Antifungal: Henny RachdiatiDocument33 pagesPolien Antifungal: Henny Rachdiatidiana agustinaNo ratings yet
- Case Study: MYXEDEMATOUS COMADocument5 pagesCase Study: MYXEDEMATOUS COMAjisooNo ratings yet
- Community Health Nursing Doh Related Programs: Epi - Types of VaccinesDocument32 pagesCommunity Health Nursing Doh Related Programs: Epi - Types of VaccinesAngelaNo ratings yet
- Adrenal GlandsDocument116 pagesAdrenal GlandsBrandon AreteNo ratings yet
- Print HDF 6eDocument3 pagesPrint HDF 6eManish AgrawalNo ratings yet
- Tumor StagingDocument9 pagesTumor Stagingmalaran.deboraheloisaNo ratings yet
- Biliary AtresiaDocument21 pagesBiliary AtresiaBeverly PagcaliwaganNo ratings yet






















































































































Download as pdf or txt
You might also like
- Adult Early Warning Score Observation Chart For Neurosurgical UnitDocument1 pageAdult Early Warning Score Observation Chart For Neurosurgical UnitalexipsNo ratings yet
- Basic Pathology - An Introduction To The Mechanisms of Disease (PDFDrive)Document340 pagesBasic Pathology - An Introduction To The Mechanisms of Disease (PDFDrive)edo58No ratings yet
- Infograph Eatingdisorders Rubric1Document2 pagesInfograph Eatingdisorders Rubric1api-296522338No ratings yet
- Pathophysiology of Hepatitis BDocument9 pagesPathophysiology of Hepatitis BDianne G Ignacio100% (4)
- Identi Fication of Synovial Fluid Biomarkers For Knee Osteoarthritis and Correlation With Radiographic AssessmentDocument6 pagesIdenti Fication of Synovial Fluid Biomarkers For Knee Osteoarthritis and Correlation With Radiographic AssessmentIndraYudhiNo ratings yet
- WOMAC Osteoarthritis Index-Additional Dimensions For Use in Subjects With Post-Traumatic Osteoarthritis of The KneeDocument6 pagesWOMAC Osteoarthritis Index-Additional Dimensions For Use in Subjects With Post-Traumatic Osteoarthritis of The KneeDian MuslimahNo ratings yet
- Efficacy and Safety of Avocado Soybean Unsaponifiables For The Treatment of Hip and Knee Osteoarthritis - A Systematic Review and Meta Analysis of Randomized Placebo Controlled TrialsDocument10 pagesEfficacy and Safety of Avocado Soybean Unsaponifiables For The Treatment of Hip and Knee Osteoarthritis - A Systematic Review and Meta Analysis of Randomized Placebo Controlled Trialsabo_youssof20047438No ratings yet
- Type 2 Diabetes Mellitus Is Associated With Increased Risks of Sarcopenia and Pre-Sarcopenia in Chinese ElderlyDocument7 pagesType 2 Diabetes Mellitus Is Associated With Increased Risks of Sarcopenia and Pre-Sarcopenia in Chinese ElderlyYafanita IzzatiNo ratings yet
- Psoas Muscle Index and Psoas Density As Predictors of Mortality in HaemodialysisDocument8 pagesPsoas Muscle Index and Psoas Density As Predictors of Mortality in HaemodialysisSvt Mscofficial2No ratings yet
- Corneal Thickness in An Ophthalmologically Normal Japanese PopulationDocument10 pagesCorneal Thickness in An Ophthalmologically Normal Japanese PopulationAndreas SimatupangNo ratings yet
- SCRIPTA SCORE Scientific Medical Journal Vol 2 No 1 OnlineDocument73 pagesSCRIPTA SCORE Scientific Medical Journal Vol 2 No 1 Online292Vien HardiyantiNo ratings yet
- A Study of Cartilage Oligomeric Matrix Protein (Comp) & Tumor Necrosis Factor - in Post Menopausal Knee Osteoarthritic Female Patient.Document4 pagesA Study of Cartilage Oligomeric Matrix Protein (Comp) & Tumor Necrosis Factor - in Post Menopausal Knee Osteoarthritic Female Patient.IJAR JOURNALNo ratings yet
- Resumo - SIICUSP - Ingles FinalDocument2 pagesResumo - SIICUSP - Ingles FinalSuel CostaNo ratings yet
- Primary Knee Arthroplasty For Osteoarthritis Restores Patients' Health-Related Quality of Life To Normal Population LevelsDocument8 pagesPrimary Knee Arthroplasty For Osteoarthritis Restores Patients' Health-Related Quality of Life To Normal Population LevelsShiv KolheNo ratings yet
- Arth2011 580632Document6 pagesArth2011 580632hylee102594No ratings yet
- 151 Effects of Physiotherapy Treatment On Knee Oa Gai 2009 Osteoarthritis AnDocument2 pages151 Effects of Physiotherapy Treatment On Knee Oa Gai 2009 Osteoarthritis AnEmad Tawfik AhmadNo ratings yet
- 1 EndometriozaDocument33 pages1 EndometriozaMandici ConstantinNo ratings yet
- Posters (Third Part) : SciencedirectDocument2 pagesPosters (Third Part) : SciencedirectshewaleakhileshNo ratings yet
- Neu 2021 0351Document9 pagesNeu 2021 0351divinechp07No ratings yet
- A Naturally Aging Knee or Development of Early KN - 2018 - Osteoarthritis and CDocument6 pagesA Naturally Aging Knee or Development of Early KN - 2018 - Osteoarthritis and CVanessa MartinsNo ratings yet
- Dir-23-5-385 VickyDocument5 pagesDir-23-5-385 Vickyvicky jessicauNo ratings yet
- Evaluation of The Kinematic Parameters of Normal-Paced Gait in Subjects With Gonarthrosis and The Influence of Gonarthrosis On The Function of The Ankle Joint and Hip JointDocument8 pagesEvaluation of The Kinematic Parameters of Normal-Paced Gait in Subjects With Gonarthrosis and The Influence of Gonarthrosis On The Function of The Ankle Joint and Hip JointRaluca ZamfirescuNo ratings yet
- 7225 39494 1 PBDocument9 pages7225 39494 1 PBBainaka De-LavangéarNo ratings yet
- A Novel Method For Assessing Postoperative Femoral Head Reduction in Developmental Dysplasia of The HipDocument6 pagesA Novel Method For Assessing Postoperative Femoral Head Reduction in Developmental Dysplasia of The HipmicNo ratings yet
- Kerangka Konsep PenelitianDocument29 pagesKerangka Konsep PenelitianGabriel KlemensNo ratings yet
- BMM 13 5Document7 pagesBMM 13 5zeravoneNo ratings yet
- Jpts 26 629Document3 pagesJpts 26 629Evelin HanaNo ratings yet
- Admin, Ahmad MulyadiDocument6 pagesAdmin, Ahmad MulyadiDinda SaviraNo ratings yet
- cc161 1Document6 pagescc161 1Hamza AhmedNo ratings yet
- Oarsi 2Document3 pagesOarsi 2Mohd Yusof BaharuddinNo ratings yet
- Body Mass Index and Susceptibility To Knee Osteoarthritis: A Systematic Review and Meta-AnalysisDocument7 pagesBody Mass Index and Susceptibility To Knee Osteoarthritis: A Systematic Review and Meta-AnalysisAmalia RosaNo ratings yet
- Prevalence of Glaucoma in India: A Review: Ronnie George, Lingam VijayaDocument5 pagesPrevalence of Glaucoma in India: A Review: Ronnie George, Lingam VijayaprinceamitNo ratings yet
- 1756-185X.13082) Huang, Lanfeng Guo, Bin Xu, Feixiang Zhao, Jinsong - Effects of Quadriceps Functional Exercise With IsDocument8 pages1756-185X.13082) Huang, Lanfeng Guo, Bin Xu, Feixiang Zhao, Jinsong - Effects of Quadriceps Functional Exercise With IsTrisna ArinataNo ratings yet
- Diagnosing OsteomyelitisDocument12 pagesDiagnosing Osteomyelitisna huNo ratings yet
- La Eficacia de Los Biomarcadores de Muerte Celular en Suero para Diagnosticar El Cáncer Del Tracto BiliarDocument7 pagesLa Eficacia de Los Biomarcadores de Muerte Celular en Suero para Diagnosticar El Cáncer Del Tracto BiliarNicolás MateoJrNo ratings yet
- Manifestaciones Clinicas de OsteoartritisDocument10 pagesManifestaciones Clinicas de OsteoartritisMeny GarciaNo ratings yet
- Muscular and Functional Capacity in Subjects Under TreatmentDocument7 pagesMuscular and Functional Capacity in Subjects Under Treatmentdavid fernandezNo ratings yet
- Faktor Risiko Hemoroid Korea NatureDocument9 pagesFaktor Risiko Hemoroid Korea NatureRatu AstridNo ratings yet
- Knee Osteo ArthritisDocument9 pagesKnee Osteo ArthritisSondang SamosirNo ratings yet
- Jurnal 5Document5 pagesJurnal 5Devita SanangkaNo ratings yet
- Zwad 229Document11 pagesZwad 229VaniNo ratings yet
- (2023) Effects of Running On The Development of Knee OsteoarthritisDocument6 pages(2023) Effects of Running On The Development of Knee Osteoarthritiscalixto1995No ratings yet
- Lateral Spine Backbone: Scoliosis: Sideways (Document3 pagesLateral Spine Backbone: Scoliosis: Sideways (khangkhungkhernitxNo ratings yet
- Biomarkers of Neutrophil Extracellular Traps NETsDocument10 pagesBiomarkers of Neutrophil Extracellular Traps NETsFriNo ratings yet
- PDF 8Document11 pagesPDF 8Amina GoharyNo ratings yet
- Age and Sex Specific Reference Intervals For Blood Urea Nitrogen in Chinese General PopulationDocument7 pagesAge and Sex Specific Reference Intervals For Blood Urea Nitrogen in Chinese General PopulationVarna AmaliaNo ratings yet
- Zwad 229Document11 pagesZwad 229Rizky AisNo ratings yet
- Osteoporosis and Osteoarthritis 2011 ConferenceDocument39 pagesOsteoporosis and Osteoarthritis 2011 ConferencetarikeopsNo ratings yet
- Comparison of Functional Disability in Patients of Knee Osteoarthritis (KOA), Among Rural and Urban KOA PatientsDocument11 pagesComparison of Functional Disability in Patients of Knee Osteoarthritis (KOA), Among Rural and Urban KOA PatientsInternational Health ReviewNo ratings yet
- بحث الثاني كامل copyDocument9 pagesبحث الثاني كامل copyasmarafie289No ratings yet
- Animals 14 00986Document11 pagesAnimals 14 00986andreza.beatrizNo ratings yet
- Medical Review: Medicinska RevijaDocument5 pagesMedical Review: Medicinska RevijaNikolina Nina MileticNo ratings yet
- Effect of The Site of Measurement of Waist Circumference On The Prevalence of The Metabolic SyndromeDocument5 pagesEffect of The Site of Measurement of Waist Circumference On The Prevalence of The Metabolic SyndromeAngie OsorioNo ratings yet
- 2018 The Learning Curve Associated With Robotic-Arm Assisted Unicompartmental Knee Arthroplasty - A Prospective Cohort StudyDocument10 pages2018 The Learning Curve Associated With Robotic-Arm Assisted Unicompartmental Knee Arthroplasty - A Prospective Cohort Studysumon.huqNo ratings yet
- Acute Effect of Partial Body Weight Suspension On The Level of Cocontraction and Gait Biomechanics in Women With Knee OsteoarthritisDocument9 pagesAcute Effect of Partial Body Weight Suspension On The Level of Cocontraction and Gait Biomechanics in Women With Knee OsteoarthritisSango AyraNo ratings yet
- Journal of Taibah University Medical SciencesDocument7 pagesJournal of Taibah University Medical SciencesIlham Amal MNo ratings yet
- Maturitas: SciencedirectDocument6 pagesMaturitas: Sciencedirectaeroforce20No ratings yet
- Outcomes of Systemic Lupus Erythematosus in Patients Who DiscontinueDocument7 pagesOutcomes of Systemic Lupus Erythematosus in Patients Who DiscontinueirsyadilfikriNo ratings yet
- Vertebral Fracture Risk (VFR) Score For Fracture Prediction in Postmenopausal WomenDocument11 pagesVertebral Fracture Risk (VFR) Score For Fracture Prediction in Postmenopausal WomenAdhiatma DotNo ratings yet
- Mascle Mass Measurement Using ML With MEGDocument14 pagesMascle Mass Measurement Using ML With MEGfuyaratasnimNo ratings yet
- Pereira 2015Document9 pagesPereira 2015Amalia RosaNo ratings yet
- Sindrome de GitelmanDocument7 pagesSindrome de GitelmanHenry Perugachi MendezNo ratings yet
- Association of Radiographic Severity of LumbarDocument2 pagesAssociation of Radiographic Severity of LumbarSumanta KamilaNo ratings yet
- Recent Advances of Sarcopenia and Frailty in CKDFrom EverandRecent Advances of Sarcopenia and Frailty in CKDAkihiko KatoNo ratings yet
- Developments in Stem Cell Derived Islet Replacement Therapy F - 2023 - Cell StemDocument19 pagesDevelopments in Stem Cell Derived Islet Replacement Therapy F - 2023 - Cell Stemdimiz77No ratings yet
- SPMBS1785Document4 pagesSPMBS1785dimiz77No ratings yet
- Clonally Resolved Single Cell Multi Omics Identifies Routes of 2023 Cell STDocument25 pagesClonally Resolved Single Cell Multi Omics Identifies Routes of 2023 Cell STdimiz77No ratings yet
- Dyspareunia - StatPearls - NCBI BookshelfDocument6 pagesDyspareunia - StatPearls - NCBI Bookshelfdimiz77No ratings yet
- 2016 Article 873Document15 pages2016 Article 873dimiz77No ratings yet
- Shantipriya Reddy, Enhancing Palatal Wound HealingDocument3 pagesShantipriya Reddy, Enhancing Palatal Wound Healingdimiz77No ratings yet
- Ed Ling 2018Document43 pagesEd Ling 2018dimiz77No ratings yet
- Biomed Res Int 2014 Tunali 209548Document7 pagesBiomed Res Int 2014 Tunali 209548dimiz77No ratings yet
- Astm. .D7246Document3 pagesAstm. .D7246dimiz77No ratings yet
- Spmbs 1805Document4 pagesSpmbs 1805dimiz77No ratings yet
- Park 2013Document10 pagesPark 2013dimiz77No ratings yet
- 1 s2.0 S0022202X15404245 MainDocument11 pages1 s2.0 S0022202X15404245 Maindimiz77No ratings yet
- PRISYM Labels Ensuring Quality Labels GuideDocument1 pagePRISYM Labels Ensuring Quality Labels Guidedimiz77No ratings yet
- Aps 43 430 2Document8 pagesAps 43 430 2dimiz77No ratings yet
- Biomed Clear Sterilization Results-5Document6 pagesBiomed Clear Sterilization Results-5dimiz77No ratings yet
- Usdm Vap Accelerator Pack MedDocument2 pagesUsdm Vap Accelerator Pack Meddimiz77No ratings yet
- 2022 Article 435-3Document10 pages2022 Article 435-3dimiz77No ratings yet
- Corp Catalog Digital All Updated 040523Document97 pagesCorp Catalog Digital All Updated 040523dimiz77No ratings yet
- Bartender Robar Case Study Zimmer BiometDocument2 pagesBartender Robar Case Study Zimmer Biometdimiz77No ratings yet
- Restigen Package InsertDocument2 pagesRestigen Package Insertdimiz77No ratings yet
- Multiple Faces of Succinate Beyond Metabolism in Blood: Review ArticleDocument7 pagesMultiple Faces of Succinate Beyond Metabolism in Blood: Review Articledimiz77No ratings yet
- Zha Image-Brochure GB RMF Reduced-2Document18 pagesZha Image-Brochure GB RMF Reduced-2dimiz77No ratings yet
- Method of Analysis For Sodium Citrate: PharmaguidelineDocument3 pagesMethod of Analysis For Sodium Citrate: Pharmaguidelinedimiz77No ratings yet
- Analysis of Citrate Content in Bone Using High Performance LiquidDocument268 pagesAnalysis of Citrate Content in Bone Using High Performance Liquiddimiz77No ratings yet
- Sensitive Ion Chromatographic Determination of CitDocument10 pagesSensitive Ion Chromatographic Determination of Citdimiz77No ratings yet
- AstroHood S III CSHT AFP CS 107ADocument2 pagesAstroHood S III CSHT AFP CS 107Adimiz77No ratings yet
- 669-Manuscript Text-2748-1-10-20090527Document5 pages669-Manuscript Text-2748-1-10-20090527dimiz77No ratings yet
- PSR1000Document2 pagesPSR1000dimiz77No ratings yet
- MAC-T Grid System Brochure - 0518Document4 pagesMAC-T Grid System Brochure - 0518dimiz77No ratings yet
- Akustik - Border: Akustik - Border Is The L-Shaped' Band To Be Easily Installed On The Perimetrical WallsDocument1 pageAkustik - Border: Akustik - Border Is The L-Shaped' Band To Be Easily Installed On The Perimetrical Wallsdimiz77No ratings yet
- Product Bulletin - NutriferonDocument2 pagesProduct Bulletin - Nutriferonshaklee480No ratings yet
- Fresh Frozen Plasma Transfusion - Guideline For PracticeDocument16 pagesFresh Frozen Plasma Transfusion - Guideline For PracticeMohd Anas SheikhNo ratings yet
- 4 5920472882638490310 Removed RemovedDocument97 pages4 5920472882638490310 Removed Removedsameena vNo ratings yet
- Drug ClassificationsDocument3 pagesDrug ClassificationsLaura Hernandez100% (3)
- PEDIA RLE Multiple Case Studies - 2Document4 pagesPEDIA RLE Multiple Case Studies - 2R-Chian Jose GermanpNo ratings yet
- Complication During PregnancyDocument43 pagesComplication During PregnancyRizza Domalaon BalangitanNo ratings yet
- Atangen CHN Journal CariagaDocument2 pagesAtangen CHN Journal CariagaTyn TynNo ratings yet
- Informasi Produk Azithromycin 0.5 G InjDocument22 pagesInformasi Produk Azithromycin 0.5 G InjVirghost14 WNo ratings yet
- Demystifying Viral Anterior Uveitis: A Review: Nicole Shu-Wen Chan Mbbs - Soon-Phaik Chee Frcophth Mmed (S'Pore)Document14 pagesDemystifying Viral Anterior Uveitis: A Review: Nicole Shu-Wen Chan Mbbs - Soon-Phaik Chee Frcophth Mmed (S'Pore)Dr Pranesh BalasubramaniamNo ratings yet
- Done Don't Need - Physical Exam TipsDocument3 pagesDone Don't Need - Physical Exam Tipskabal321No ratings yet
- Association of Microbiome With Oral Squamous CellDocument21 pagesAssociation of Microbiome With Oral Squamous CellGhimpu DanielaNo ratings yet
- Polycrest RemediesDocument2 pagesPolycrest RemediesMd. NazimNo ratings yet
- Format For Clinical and Family Case PresentationDocument4 pagesFormat For Clinical and Family Case PresentationCATHERINE HAYNESNo ratings yet
- Middle Meatal AntrostomyDocument2 pagesMiddle Meatal AntrostomymajidjankakakhelNo ratings yet
- 4.2.2 Risk Factors of Breast Cancer Among Women A Meta AnalysisDocument15 pages4.2.2 Risk Factors of Breast Cancer Among Women A Meta AnalysisNoob KidNo ratings yet
- Drug Study - Amiodaron HydrochlorideDocument4 pagesDrug Study - Amiodaron HydrochlorideTwinkle SalongaNo ratings yet
- Course Task 4 - Thrombophlebitis (De Jesus, LG E.)Document2 pagesCourse Task 4 - Thrombophlebitis (De Jesus, LG E.)LOVELLE GRACE DE JESUSNo ratings yet
- MPT - 1 Year Question Paper (Physical and Functional Diag.)Document10 pagesMPT - 1 Year Question Paper (Physical and Functional Diag.)aishp2897No ratings yet
- Abnormal Uterine Bleeding TreatmentDocument6 pagesAbnormal Uterine Bleeding TreatmentdrdivyakumargynaecNo ratings yet
- Polien Antifungal: Henny RachdiatiDocument33 pagesPolien Antifungal: Henny Rachdiatidiana agustinaNo ratings yet
- Case Study: MYXEDEMATOUS COMADocument5 pagesCase Study: MYXEDEMATOUS COMAjisooNo ratings yet
- Community Health Nursing Doh Related Programs: Epi - Types of VaccinesDocument32 pagesCommunity Health Nursing Doh Related Programs: Epi - Types of VaccinesAngelaNo ratings yet
- Adrenal GlandsDocument116 pagesAdrenal GlandsBrandon AreteNo ratings yet
- Print HDF 6eDocument3 pagesPrint HDF 6eManish AgrawalNo ratings yet
- Tumor StagingDocument9 pagesTumor Stagingmalaran.deboraheloisaNo ratings yet
- Biliary AtresiaDocument21 pagesBiliary AtresiaBeverly PagcaliwaganNo ratings yet