Download as pdf or txt
You might also like
- Science: Quarter 3 - Module 2: The Female Reproductive System and The Menstrual CycleDocument25 pagesScience: Quarter 3 - Module 2: The Female Reproductive System and The Menstrual Cyclejane mamon100% (1)
- Bleeding in Early PregnancyDocument25 pagesBleeding in Early PregnancyAnnapurna DangetiNo ratings yet
- Uterine MalformationsDocument6 pagesUterine MalformationssubashikNo ratings yet
- Contraceptive TechnologyDocument68 pagesContraceptive TechnologySravanthi Karingula100% (1)
- Anatomy of Womans Sex OrganDocument5 pagesAnatomy of Womans Sex Organsumeer khan63% (8)
- Polycystic Ovarian SyndromeDocument47 pagesPolycystic Ovarian SyndromeAnonymous HgX3mN1o100% (1)
- First Trimester BleedingDocument93 pagesFirst Trimester BleedingScribdTranslationsNo ratings yet
- SafaDocument7 pagesSafafafe fefeyNo ratings yet
- 2.uterine AbnormalitiesDocument11 pages2.uterine AbnormalitiesKuleshwar SahuNo ratings yet
- Uterine Malformations PDFDocument6 pagesUterine Malformations PDFsaritha OrugantiNo ratings yet
- Uterine Malformations PDFDocument6 pagesUterine Malformations PDFsaritha OrugantiNo ratings yet
- Ectopic Pregnancy: Clinical PracticeDocument9 pagesEctopic Pregnancy: Clinical PracticeNurul WulandariNo ratings yet
- Reflection Urinary Tract InfectionDocument1 pageReflection Urinary Tract InfectionAce Dioso TubascoNo ratings yet
- The Evaluation of Abnormal Uterine BleedingDocument16 pagesThe Evaluation of Abnormal Uterine BleedingEstefania gonzalez torresNo ratings yet
- Benin LesionDocument14 pagesBenin Lesionsandeepv08No ratings yet
- Seminar On BepDocument35 pagesSeminar On BepJyothi RameshNo ratings yet
- Anomalies of The Female Genital TractDocument2 pagesAnomalies of The Female Genital TractAnastasia KasapiNo ratings yet
- Abnormalities of The Female Reproductive Tract Mullerian DefectsDocument1 pageAbnormalities of The Female Reproductive Tract Mullerian DefectsPreethi ShivanandNo ratings yet
- Under Supervision Of: Dr. Enas AdnanDocument9 pagesUnder Supervision Of: Dr. Enas AdnanSarraa NajimNo ratings yet
- Mullerian MalformationsDocument6 pagesMullerian MalformationsMau JkjlNo ratings yet
- Benign Conditions of The BreastDocument9 pagesBenign Conditions of The BreastSalim Mwiti NabeaNo ratings yet
- Mullerian AgenesisDocument6 pagesMullerian Agenesislestertallulah11No ratings yet
- Ectopic Pregnancy - StatPearls - NCBI BookshelfDocument9 pagesEctopic Pregnancy - StatPearls - NCBI BookshelfKatherine DavilaNo ratings yet
- Uterine Anomalies - OB-GYNDocument4 pagesUterine Anomalies - OB-GYNNatnael GetahunNo ratings yet
- Ectopic Pregnancy - StatPearls - NCBI BookshelfDocument6 pagesEctopic Pregnancy - StatPearls - NCBI BookshelfLaura valentina ramos mezaNo ratings yet
- Uterine Displacement MainDocument23 pagesUterine Displacement MainRai RaiNo ratings yet
- 14 Abortion Noted PDFDocument37 pages14 Abortion Noted PDFmohammed farajiNo ratings yet
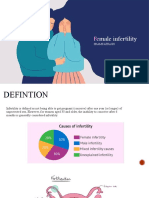
- Female Infertility: Harsha Joseph M17LS25 Msc. Life ScienceDocument10 pagesFemale Infertility: Harsha Joseph M17LS25 Msc. Life ScienceHarsha JosephNo ratings yet
- Obg AbortionDocument62 pagesObg Abortionkashyap priyankaNo ratings yet
- Bleeding During PregnancyDocument69 pagesBleeding During PregnancyMohnnad Hmood AlgaraybhNo ratings yet
- Rupture of The Uterus English RefratDocument11 pagesRupture of The Uterus English RefratassicaNo ratings yet
- BCC 2008Document5 pagesBCC 2008mesNo ratings yet
- Early Part ComplicationDocument86 pagesEarly Part ComplicationyewollolijfikreNo ratings yet
- Acute Complications of PregnancyDocument25 pagesAcute Complications of PregnancyRocky PangerapanNo ratings yet
- Artículo Menopausia 2Document17 pagesArtículo Menopausia 2daniela otaNo ratings yet
- Obgyn SGDocument40 pagesObgyn SGNatalieNo ratings yet
- Female InfertilityDocument32 pagesFemale InfertilityShams AtrashNo ratings yet
- JM Biomedik,+ok+ (4) +Erna+Suparman+334-337+doiDocument4 pagesJM Biomedik,+ok+ (4) +Erna+Suparman+334-337+doibutterflyNo ratings yet
- Pregnancy and LeimyomaDocument5 pagesPregnancy and Leimyomasamsara vrindaNo ratings yet
- Midwifery Triage of First Trimester Bleeding: Susan A. Krause,, and Barbara W. GravesDocument12 pagesMidwifery Triage of First Trimester Bleeding: Susan A. Krause,, and Barbara W. GravesRival Risvaldi RusliNo ratings yet
- Healy1994 PDFDocument6 pagesHealy1994 PDFAdiNo ratings yet
- Differential DiagnosisDocument85 pagesDifferential DiagnosisSayyeda niha AkhtarNo ratings yet
- Hadawale N. M, Thorat R. M., Gaikwad D. D., Jadhav S. LDocument4 pagesHadawale N. M, Thorat R. M., Gaikwad D. D., Jadhav S. LAditya VirayudhaNo ratings yet
- Hymen ImperforataDocument16 pagesHymen ImperforataImanuella KairupanNo ratings yet
- Successful Pregnancy Outcome in A Case of Bi-Cornuate Uterus With Boh With Secondary Infertility and GDM - A Very Rare Case Report - Medisun AcademyDocument4 pagesSuccessful Pregnancy Outcome in A Case of Bi-Cornuate Uterus With Boh With Secondary Infertility and GDM - A Very Rare Case Report - Medisun AcademyGautom Kumar PaulNo ratings yet
- 3 s2.0 B9780323359559000052Document19 pages3 s2.0 B9780323359559000052file fileNo ratings yet
- Congenital Anomalies of The Uterus and VaginaDocument3 pagesCongenital Anomalies of The Uterus and VaginaKhupe KafundaNo ratings yet
- Slides Mullerian AnomaliesDocument29 pagesSlides Mullerian AnomaliesAsunción AncoNo ratings yet
- Gynecologic Pain and Vaginal Bleeding: Jamie L. Collings and Nicholas A. BormDocument11 pagesGynecologic Pain and Vaginal Bleeding: Jamie L. Collings and Nicholas A. BormAnton ArifinNo ratings yet
- Committee Opinion No. 562 Müllerian Agenesis Diagnosis, Management, and TreatmentDocument4 pagesCommittee Opinion No. 562 Müllerian Agenesis Diagnosis, Management, and Treatmentvu hong chienNo ratings yet
- 1325 2431 1 SMDocument6 pages1325 2431 1 SMZenira PitalokaNo ratings yet
- Dun 2012Document16 pagesDun 2012Anonymous c4GVTgkvNo ratings yet
- 4.recent Advancement in Infertility TreatmentDocument23 pages4.recent Advancement in Infertility TreatmentVeena DalmeidaNo ratings yet
- 16 Prolapse IndonesianDocument17 pages16 Prolapse IndonesianDwi MahendraNo ratings yet
- GTD TogDocument6 pagesGTD TogNyoman TapayanaNo ratings yet
- PDF Wu P BSN 2 BLK 5 Final Manuscript Case PresDocument27 pagesPDF Wu P BSN 2 BLK 5 Final Manuscript Case PresAngela Nicole MarcosNo ratings yet
- Shehla PDFDocument4 pagesShehla PDFRahmayanti YuliaNo ratings yet
- Ob GynDocument13 pagesOb GynDianne Geremy RojoNo ratings yet
- M. Yusof (Dawood, M.D., M.MED. M.R.C.O.G.: University of College of Chicago, LlinoisDocument9 pagesM. Yusof (Dawood, M.D., M.MED. M.R.C.O.G.: University of College of Chicago, LlinoisS MpNo ratings yet
- Midwifery 102 Module 1Document10 pagesMidwifery 102 Module 1WynJoy NebresNo ratings yet
- Jurnal Internasional Ruptur UteriDocument5 pagesJurnal Internasional Ruptur UteriNovita MayasariNo ratings yet
- Gestational and Placental Disorders: Ovary Pregnancy Results From TheDocument4 pagesGestational and Placental Disorders: Ovary Pregnancy Results From TheyepNo ratings yet
- Abnormal Uterine Bleeding: Understanding, Diagnosis, and TreatmentFrom EverandAbnormal Uterine Bleeding: Understanding, Diagnosis, and TreatmentNo ratings yet
- Body Map For Male and Female PDFDocument2 pagesBody Map For Male and Female PDFDOMINGO HENG-GE CHUANo ratings yet
- Male Anatomy ChartDocument2 pagesMale Anatomy ChartKikikikimmyNo ratings yet
- NHS Tayside Flowchart For Systemic HRT Prescribing: AbbreviationsDocument2 pagesNHS Tayside Flowchart For Systemic HRT Prescribing: AbbreviationspiNo ratings yet
- Overview of CircumcisionDocument43 pagesOverview of CircumcisionMakbruri Abdul AzizNo ratings yet
- AQA Biology GCSE Combined B11 Summary AnswersDocument5 pagesAQA Biology GCSE Combined B11 Summary AnswersMahebul MazidNo ratings yet
- MCN Menstrual Cycle LatestDocument8 pagesMCN Menstrual Cycle LatestsophienNo ratings yet
- Basic Investigation of An Infertile CoupleDocument53 pagesBasic Investigation of An Infertile CoupleRemelou Garchitorena AlfelorNo ratings yet
- Management and Prognosis of Congenital AbnomaliesDocument11 pagesManagement and Prognosis of Congenital AbnomaliesnugiexNo ratings yet
- Fertility AssessmentDocument38 pagesFertility AssessmentSkmc InfertilityNo ratings yet
- Understanding The SelfDocument48 pagesUnderstanding The SelfDaylight DreamerNo ratings yet
- Breast Stimulation Susilowati 2004138Document11 pagesBreast Stimulation Susilowati 2004138Ahmad SaifuddinNo ratings yet
- Male and Female Sex HormonesDocument20 pagesMale and Female Sex HormonesJose Fernando Gregana ElpaNo ratings yet
- Menstrual CycleDocument17 pagesMenstrual CycleDr.vaibhav agarwalNo ratings yet
- Polip Serviks: Clinical Science SectionDocument15 pagesPolip Serviks: Clinical Science SectionnsrinanaNo ratings yet
- What Is The Sound Like Fart Comes From Vagina AftDocument1 pageWhat Is The Sound Like Fart Comes From Vagina AftPrecious LadeeNo ratings yet
- Answers:: Homework #1Document3 pagesAnswers:: Homework #1Ibrahim ShanaaNo ratings yet
- OgenisisDocument52 pagesOgenisisBharat ThapaNo ratings yet
- Dysfunctional Uterine BleedingDocument2 pagesDysfunctional Uterine BleedingBen TaufikNo ratings yet
- Human Artificial InseminationDocument13 pagesHuman Artificial InseminationMary Joy JunioNo ratings yet
- Relly Yanuari Primariawan, DR., SpOG (K) - Kenapa Penting Terapi Post Op Endometriosis-1Document38 pagesRelly Yanuari Primariawan, DR., SpOG (K) - Kenapa Penting Terapi Post Op Endometriosis-1oktavianusNo ratings yet
- Principles of Ultrasonographic ImagingDocument89 pagesPrinciples of Ultrasonographic ImagingDamian Ana MariaNo ratings yet
- Human Menopausal Gonadotropins (HMG) : Coverage RationaleDocument11 pagesHuman Menopausal Gonadotropins (HMG) : Coverage RationaleMahmoud El MohamdyNo ratings yet
- Kualitas Hidup MenopauseDocument9 pagesKualitas Hidup MenopauseRoviqi Bozgank AzemNo ratings yet
- Cycles/ Stages of Menstrual Cycle: Follicles FollicleDocument6 pagesCycles/ Stages of Menstrual Cycle: Follicles FollicleAaliyah CarlobosNo ratings yet
- Assessment of Male Genitalia Procedure Findings PenisDocument2 pagesAssessment of Male Genitalia Procedure Findings PenisAlliah IsraelNo ratings yet
- Module 2 The Human Reproductive Anatomy and PhysiologyDocument27 pagesModule 2 The Human Reproductive Anatomy and PhysiologyJhunna Talangan100% (1)