Download as pdf or txt
You might also like
- Nursing Mock Interview TemplateDocument13 pagesNursing Mock Interview TemplateJanmarie Bongcaron100% (1)
- Basic, High-Risk, and Critical Care Intrapartum Nursing: Clinical Competencies and Education Guide, 6th EditionDocument22 pagesBasic, High-Risk, and Critical Care Intrapartum Nursing: Clinical Competencies and Education Guide, 6th EditionAji SadamNo ratings yet
- Neonatal Ventilation Made EasyDocument97 pagesNeonatal Ventilation Made EasyCảnh HoàngNo ratings yet
- Reflection Identification of Area of Practice To Be Developed What Went Well? What Was Difficult?Document3 pagesReflection Identification of Area of Practice To Be Developed What Went Well? What Was Difficult?Mc SantosNo ratings yet
- Applied Learning Project Tri-Fold Board Final DraftDocument1 pageApplied Learning Project Tri-Fold Board Final Draftapi-527938320No ratings yet
- MCN Intro and AssessmentDocument29 pagesMCN Intro and AssessmentJOVEMEA LIRAYNo ratings yet
- WaterlaseDocument1 pageWaterlaseJackie CooperNo ratings yet
- RLE JOURNAL - Night BDH OBWard - RamosDocument2 pagesRLE JOURNAL - Night BDH OBWard - RamosPang ProjectNo ratings yet
- Becoming A Doctor: One Physician's Journey Beyond CompetenceDocument4 pagesBecoming A Doctor: One Physician's Journey Beyond CompetenceElla TillockNo ratings yet
- Midterm 3021Document9 pagesMidterm 3021api-283170120No ratings yet
- Learning ExperienceDocument2 pagesLearning ExperienceMhica PrestozaNo ratings yet
- Objective Activities Time Allotment EvaluationDocument3 pagesObjective Activities Time Allotment EvaluationBexve C. BRA�ANo ratings yet
- IDoR2015 Paediatric-Imaging-Book FINAL PDFDocument129 pagesIDoR2015 Paediatric-Imaging-Book FINAL PDFMelii LujanNo ratings yet
- Midterm Evaluation - NselkirkDocument12 pagesMidterm Evaluation - Nselkirkapi-313720439No ratings yet
- Senior TrifoldDocument1 pageSenior Trifoldapi-528343107No ratings yet
- MindfulnessDocument2 pagesMindfulnessAndreaBuitragoMalaverNo ratings yet
- Example of An Individual Learning PlanDocument1 pageExample of An Individual Learning PlanfayaNo ratings yet
- So Why Do You Want To Become An Anesthesiologist?Document4 pagesSo Why Do You Want To Become An Anesthesiologist?tia_drNo ratings yet
- CC4 CAACBAY Katelene SLI8Document2 pagesCC4 CAACBAY Katelene SLI8Cáit AnuaNo ratings yet
- 1 Seminar 2 Podcast MentorshipDocument4 pages1 Seminar 2 Podcast MentorshipJade MalabananNo ratings yet
- RLE JOURNAL - Emmaus - RamosDocument4 pagesRLE JOURNAL - Emmaus - RamosPang ProjectNo ratings yet
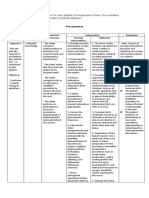
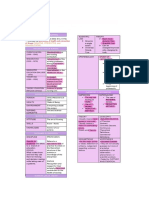
- Pre OperativeDocument7 pagesPre OperativeSiena KaleiNo ratings yet
- Ped Ob Reflection 1Document4 pagesPed Ob Reflection 1api-581678058No ratings yet
- Patient TalkDocument1 pagePatient Talkapi-633690952No ratings yet
- The Medicalization of Nursing The Loss of A Discipline's Unique IdentityDocument8 pagesThe Medicalization of Nursing The Loss of A Discipline's Unique IdentityМарго КоваленкоNo ratings yet
- Personal Development PlanningDocument2 pagesPersonal Development PlanningMuhmmad HassanNo ratings yet
- Mcclafferty Nur 460 Capstone Practicum LogDocument3 pagesMcclafferty Nur 460 Capstone Practicum Logapi-598255967No ratings yet
- Lesson Plan: General ObjectiveDocument6 pagesLesson Plan: General ObjectiveSarita yadavNo ratings yet
- A Reflection On Nursing in Neurosurgery.1Document1 pageA Reflection On Nursing in Neurosurgery.1lolNo ratings yet
- Professional Portfolio - GenericDocument17 pagesProfessional Portfolio - GenericGracie S. VergaraNo ratings yet
- Subject: Advance Nursing Pratice: Lesson Plan On Nursing As A ProfessionDocument17 pagesSubject: Advance Nursing Pratice: Lesson Plan On Nursing As A ProfessionVaishali SinghNo ratings yet
- Cover Letter Bus Writing EditedDocument2 pagesCover Letter Bus Writing Editedapi-640472371No ratings yet
- Tog 12625Document8 pagesTog 12625saeed hasan saeedNo ratings yet
- Practice Summary PaperDocument15 pagesPractice Summary Paperapi-500176370No ratings yet
- NURS8015 Tanner'S Clinical Judgment Model For Practice ReflectionDocument10 pagesNURS8015 Tanner'S Clinical Judgment Model For Practice ReflectionMehgiba -No ratings yet
- Learning Feedback DiaryDocument3 pagesLearning Feedback DiaryNathalie kate petallarNo ratings yet
- Learning Feedback DiaryDocument3 pagesLearning Feedback DiaryDebbie beeNo ratings yet
- Cailao, CJ - Narrative Report PDFDocument10 pagesCailao, CJ - Narrative Report PDFCristel CailaoNo ratings yet
- Viora Rebirth Provides: Post Pregnancy Rejuvenation SolutionDocument1 pageViora Rebirth Provides: Post Pregnancy Rejuvenation SolutionRandy BranamNo ratings yet
- Professional Development Grid EhhDocument3 pagesProfessional Development Grid Ehhapi-354642078No ratings yet
- Good NotesDocument5 pagesGood NotesMikee BoomNo ratings yet
- Revitalizing-Ni Lab-MidtermDocument4 pagesRevitalizing-Ni Lab-MidtermJeannezelle Anne Mariz GazaNo ratings yet
- Venepuncture ReflectionDocument7 pagesVenepuncture ReflectionYour NameNo ratings yet
- Venepuncture ReflectionDocument7 pagesVenepuncture ReflectionYour NameNo ratings yet
- Attitude Is A Little Thing That Makes A Big DifferenceDocument12 pagesAttitude Is A Little Thing That Makes A Big DifferenceKeyser Dagiw-aNo ratings yet
- Bughao, Maria Angelika A. (Narrative Report)Document8 pagesBughao, Maria Angelika A. (Narrative Report)Maria Angelika Bughao100% (2)
- Final EvaluationDocument17 pagesFinal Evaluationapi-603938769No ratings yet
- Monthly Shot February 2024Document10 pagesMonthly Shot February 2024api-308247685No ratings yet
- Magnification Gordon Chis Tens enDocument4 pagesMagnification Gordon Chis Tens enIntegra Dental InnovationsNo ratings yet
- Funda ReviewerDocument3 pagesFunda ReviewerJohana Pinagayao AngkadNo ratings yet
- Articulo Terapia OcupacionalDocument13 pagesArticulo Terapia OcupacionalSara Merino EgidoNo ratings yet
- NCM103 (FUNDA) Module 1 Concept of NursingDocument4 pagesNCM103 (FUNDA) Module 1 Concept of NursingJohn Joseph CruzNo ratings yet
- Proofed - Nurs 3021 Final EvaulDocument20 pagesProofed - Nurs 3021 Final Evaulapi-313199824No ratings yet
- Feb 2021 Monthly Shot FinalDocument12 pagesFeb 2021 Monthly Shot Finalapi-308247685No ratings yet
- Volume 06 No.4Document24 pagesVolume 06 No.4Rebin AliNo ratings yet
- Pediatrics Journal - Module 4Document1 pagePediatrics Journal - Module 4Quenee Joyce CabelloNo ratings yet
- KELSEY3333Document4 pagesKELSEY3333Kelsey Sofia RojasNo ratings yet
- Objective: Short Term Objectives: Diagnostic: Sto: Partially MET, TheDocument2 pagesObjective: Short Term Objectives: Diagnostic: Sto: Partially MET, TheWayne LoriaNo ratings yet
- Blush Watercolor Organic Weekly JournalDocument1 pageBlush Watercolor Organic Weekly Journal202211020No ratings yet
- Peplau's TheoryDocument9 pagesPeplau's TheoryJasmine Nicole EnriquezNo ratings yet
- Evidence Based, Cost Effective, And Compassionate Surgical Care of the Spine Injured Worker: Comprehensive Review of the Literature and Experience-Based Fair and Balanced ApproachFrom EverandEvidence Based, Cost Effective, And Compassionate Surgical Care of the Spine Injured Worker: Comprehensive Review of the Literature and Experience-Based Fair and Balanced ApproachNo ratings yet
- 8758 - PPT AchondroplasiaDocument33 pages8758 - PPT AchondroplasiaFidesha Nurganiah SiregarNo ratings yet
- Full Chapter Practical Management of Pain 6E May 19 2022 6Th Edition Benzon MD PDFDocument53 pagesFull Chapter Practical Management of Pain 6E May 19 2022 6Th Edition Benzon MD PDFearnestine.cobb331100% (6)
- ICD 10 For Oral DiagnosisDocument12 pagesICD 10 For Oral DiagnosisStanley Santosa KamadjajaNo ratings yet
- CPG Managment of Neonatal Jaundice (Second Edition) NewDocument62 pagesCPG Managment of Neonatal Jaundice (Second Edition) NewHafiz HamidiNo ratings yet
- Chronic Inflammatory Demyelinating PolyradiculoneuropathyDocument5 pagesChronic Inflammatory Demyelinating PolyradiculoneuropathyDiego Fernando AlegriaNo ratings yet
- Mbbs - Lecture Notes, Study Material and Important Questions, AnswersDocument4 pagesMbbs - Lecture Notes, Study Material and Important Questions, AnswersM.V. TV67% (3)
- Benefits of Early Treatment Using Nasoalveolar Molding in An Infant With Unilateral Complete Cleft Lip and Palate A Case ReportDocument1 pageBenefits of Early Treatment Using Nasoalveolar Molding in An Infant With Unilateral Complete Cleft Lip and Palate A Case ReportGabriellaMariaNo ratings yet
- Scared Child With Scoring 1Document2 pagesScared Child With Scoring 1Fekete OrsolyaNo ratings yet
- A Cry For Equity in The Operating Room CinahlDocument5 pagesA Cry For Equity in The Operating Room Cinahl54786No ratings yet
- Economics of An Urgent Care Center in A Market of Emergency DepartmentsDocument6 pagesEconomics of An Urgent Care Center in A Market of Emergency Departmentsdaron_vchulekNo ratings yet
- Health Awards 2022Document22 pagesHealth Awards 2022Varun SoodNo ratings yet
- Project On Outpatient DepartmentDocument41 pagesProject On Outpatient DepartmentAnonymous utfuIcnNo ratings yet
- Jeehp 12 06Document4 pagesJeehp 12 06Sohini KhushiNo ratings yet
- Humidified High Flow Nasal Cannula Oxygen Guideline PDFDocument27 pagesHumidified High Flow Nasal Cannula Oxygen Guideline PDFjoaoalmeida_1955No ratings yet
- Stretch & SweepDocument3 pagesStretch & SweepYwagar YwagarNo ratings yet
- Gurrea Bruguera IJED 2014Document18 pagesGurrea Bruguera IJED 2014SitiKhadijahNo ratings yet
- Patellar Tendinitis Exercises - tcm28-180778Document5 pagesPatellar Tendinitis Exercises - tcm28-180778Maiko Gil HiwatigNo ratings yet
- Absorbance at 405Nm: United States PatentDocument20 pagesAbsorbance at 405Nm: United States Patentfelipe_fismed4429No ratings yet
- Antibiotic Therapy For Deep Neck AbscessDocument7 pagesAntibiotic Therapy For Deep Neck Abscessteu.yamNo ratings yet
- Referral HospitalDocument10 pagesReferral HospitalSundaramoorthy KaliappanNo ratings yet
- 35Document174 pages35sggdgdNo ratings yet
- 52 Review ArticlesDocument5 pages52 Review ArticlesmirabelladonnaNo ratings yet
- Cassidy Leroux ResumeDocument2 pagesCassidy Leroux Resumeapi-454372465No ratings yet
- 345-Article Text-1032-1-10-20180629Document4 pages345-Article Text-1032-1-10-20180629Regina AyediaNo ratings yet
- Lester Levenson StoryDocument25 pagesLester Levenson StoryAnonymous 2a1YI92k9LNo ratings yet
- Topics On Prosthetics & Orthotics - PDF CreDocument4 pagesTopics On Prosthetics & Orthotics - PDF CreSuprit MahakudNo ratings yet
- Conebeam CT of The Head and Neck, Part 2: Clinical ApplicationsDocument8 pagesConebeam CT of The Head and Neck, Part 2: Clinical ApplicationshaneefmdfNo ratings yet
- Bibliography For Ch. "Ophthalmology": Last Updated: May 9, 2019Document2 pagesBibliography For Ch. "Ophthalmology": Last Updated: May 9, 2019Okami PNo ratings yet
- GE Logiq S7 Radiology (Mid-Range) With 2 ProbesDocument3 pagesGE Logiq S7 Radiology (Mid-Range) With 2 ProbesserubimNo ratings yet