Download as pdf or txt
You might also like
- Test Bank For Pathophysiology Concepts of Human Disease 1st Edition Matthew Sorenson Lauretta Quinn Diane KleinDocument36 pagesTest Bank For Pathophysiology Concepts of Human Disease 1st Edition Matthew Sorenson Lauretta Quinn Diane Kleinknobbyettinjn4u4f100% (44)
- VanPutte Seeleys Essentials 11e Chap11 PPT AccessibleDocument49 pagesVanPutte Seeleys Essentials 11e Chap11 PPT AccessibleJoshua UyNo ratings yet
- ElectrocardiogramDocument11 pagesElectrocardiogramAbby BhevNo ratings yet
- LITFL - Wellens SyndromeDocument8 pagesLITFL - Wellens Syndromesunil abrahamNo ratings yet
- Wellens Syndrome - LITFL - ECG Library EponymDocument1 pageWellens Syndrome - LITFL - ECG Library Eponymchinmoysaha17No ratings yet
- The Mysterious U Wave PDFDocument3 pagesThe Mysterious U Wave PDFYaxkin NikNo ratings yet
- Wellen EcgDocument9 pagesWellen EcgElokNo ratings yet
- WellensDocument7 pagesWellenscardiologiaimss34No ratings yet
- Wellens Syndrome Is An Easy ToDocument14 pagesWellens Syndrome Is An Easy Toprofemt1No ratings yet
- ECG Discussion: Wellens Syndrome: A Subtle ECG FindingDocument1 pageECG Discussion: Wellens Syndrome: A Subtle ECG FindingEINSTEIN2DNo ratings yet
- 21 - 23 - 59 - 17 - 03 - 2024 - Sunday Academic MeetDocument14 pages21 - 23 - 59 - 17 - 03 - 2024 - Sunday Academic MeettamilmathisajuNo ratings yet
- T Wave PDFDocument6 pagesT Wave PDFgabernNo ratings yet
- Im 2Document3 pagesIm 2neni budiNo ratings yet
- Wellens Syndrome.Document4 pagesWellens Syndrome.Kuldeep ShahNo ratings yet
- Ecg Changes in Acute Myocardial InfractionDocument13 pagesEcg Changes in Acute Myocardial Infractionarif mahammad bhuniyaNo ratings yet
- Ekg MorphologyDocument1 pageEkg MorphologyTeresa MartinsNo ratings yet
- Jamainternal Zhang 2021 Ce 210028 1635441147.09994Document2 pagesJamainternal Zhang 2021 Ce 210028 1635441147.09994gwyneth.green.512No ratings yet
- Proximal RCA Occlusion Producing Anterior ST Segment Elevation, Q Waves, and T Wave InversionDocument5 pagesProximal RCA Occlusion Producing Anterior ST Segment Elevation, Q Waves, and T Wave InversionsunhaolanNo ratings yet
- Wellens SyndromeDocument4 pagesWellens Syndromeqayyum consultantfpscNo ratings yet
- ECG in MI or ACSDocument47 pagesECG in MI or ACSmaya_pradipNo ratings yet
- Lipinski 2018Document14 pagesLipinski 2018gino loja villenaNo ratings yet
- Lightning+Learning+ +Wellens+Syndrome+ (v1.0)Document1 pageLightning+Learning+ +Wellens+Syndrome+ (v1.0)Ardie FratamaNo ratings yet
- ECG in Acute Coronary Syndrome: DR Awadhesh Kumar Sharma Deptt of CardiologyDocument47 pagesECG in Acute Coronary Syndrome: DR Awadhesh Kumar Sharma Deptt of CardiologyIndomedikgramNo ratings yet
- EKG - Bagian 2Document56 pagesEKG - Bagian 2lintang andilaNo ratings yet
- Wellens Syndrome - StatPearls - NCBI BookshelfDocument7 pagesWellens Syndrome - StatPearls - NCBI BookshelfCecilio MartínNo ratings yet
- Stemi, Stemi Equivalents and STEMI Mimics: Kyaw Soe WinDocument114 pagesStemi, Stemi Equivalents and STEMI Mimics: Kyaw Soe WinYoung MilkNo ratings yet
- Prevalensi Atrioventrikular Blok Di RSUP Prof. Dr. R. D. Kandou Manado Periode 2013 - 2014Document6 pagesPrevalensi Atrioventrikular Blok Di RSUP Prof. Dr. R. D. Kandou Manado Periode 2013 - 2014Herlinda Puji LNo ratings yet
- 12 Lead ECG Intro To 12 Lead Ischemia Injury and Infarction 2022-2Document68 pages12 Lead ECG Intro To 12 Lead Ischemia Injury and Infarction 2022-2Ali GiriunasNo ratings yet
- Interpretasi ElektrokardiogramDocument36 pagesInterpretasi ElektrokardiogramendahNo ratings yet
- Thinking About Ecgs (Garcia)Document9 pagesThinking About Ecgs (Garcia)Filip IonescuNo ratings yet
- Somers 2002Document9 pagesSomers 2002MariaannaNo ratings yet
- ECG Made Easy - An Abnormal LookDocument46 pagesECG Made Easy - An Abnormal LookabdallahNo ratings yet
- Basicelectrocardiogram ppt2013Document134 pagesBasicelectrocardiogram ppt2013Catalin LeonteNo ratings yet
- ABC of Clinical Electrocardiography - Introduction. II-Basic Terminology - PMCDocument11 pagesABC of Clinical Electrocardiography - Introduction. II-Basic Terminology - PMCRuban RichardNo ratings yet
- ST Segment ElevationsDocument114 pagesST Segment ElevationsMuruganandham RNo ratings yet
- ST-T Depression HannaDocument11 pagesST-T Depression Hannadrimran570No ratings yet
- ECG Findings: Valvular Heart Disease Cardiomyopathies MyocarditisDocument30 pagesECG Findings: Valvular Heart Disease Cardiomyopathies MyocarditisensiNo ratings yet
- ECG Master Class-3Document97 pagesECG Master Class-3Shohag ID CenterNo ratings yet
- EKG Interpretation: UNC Emergency Medicine Medical Student Lecture SeriesDocument58 pagesEKG Interpretation: UNC Emergency Medicine Medical Student Lecture SeriesRenn Karlo LindoNo ratings yet
- EKG Interpretation: UNS Cardiovascular Dept Medical Student Lecture SeriesDocument85 pagesEKG Interpretation: UNS Cardiovascular Dept Medical Student Lecture Seriesandina rosmalianti100% (1)
- Onderwijs ECG Quiz 2014 AntwoordenDocument3 pagesOnderwijs ECG Quiz 2014 AntwoordenKelsey van SonNo ratings yet
- Wellen's Syndrome EHJ (E-Poster)Document1 pageWellen's Syndrome EHJ (E-Poster)Aris MarutoNo ratings yet
- 4-Subtle ECG in ACSDocument20 pages4-Subtle ECG in ACSyandraNo ratings yet
- ECG Hipertrofii Atriale Si Ventriculare, Blocuri de Ramura, IschemieDocument60 pagesECG Hipertrofii Atriale Si Ventriculare, Blocuri de Ramura, IschemieAndreea ŞtefănescuNo ratings yet
- EkgDocument3 pagesEkgMihaela GaidurNo ratings yet
- Ekg InterpretationDocument8 pagesEkg InterpretationEngelbert AddonganNo ratings yet
- The Kiss of The Girl From IpanemaDocument4 pagesThe Kiss of The Girl From IpanemaDrMarcus KeyboardNo ratings yet
- Clinical ECG RoundsDocument2 pagesClinical ECG RoundsKai Siang ChanNo ratings yet
- ST-segment Depression: All Are Not Created Equal!Document6 pagesST-segment Depression: All Are Not Created Equal!asclepiuspdfsNo ratings yet
- Wellen SyndromeDocument8 pagesWellen SyndromeAkif AhamadNo ratings yet
- EKG PJK Co AssDocument115 pagesEKG PJK Co AsssalmaNo ratings yet
- 4.17 Keane Aortic StenosisDocument61 pages4.17 Keane Aortic StenosisFarman JaaferNo ratings yet
- An Ominous Anterior T Wave Changes: A Case Report On Wellens' SyndromeDocument3 pagesAn Ominous Anterior T Wave Changes: A Case Report On Wellens' SyndromeJayden WaveNo ratings yet
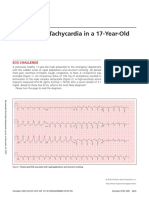
- A Wide QRS Tachycardia in A 17-Year-OldDocument4 pagesA Wide QRS Tachycardia in A 17-Year-OldTaynan MassaroNo ratings yet
- ECG ExaminationDocument70 pagesECG ExaminationPercy Caceres OlivaresNo ratings yet
- Basic ECG InterpretationDocument16 pagesBasic ECG InterpretationKim BadillesNo ratings yet
- Ecg 4Document18 pagesEcg 4api-3757039100% (3)
- ECG DiscussionDocument33 pagesECG Discussionyrx8k8j9qyNo ratings yet
- ECG On ACSDocument28 pagesECG On ACSAlshity Nur HariyatiNo ratings yet
- Decoding Cardiac Electrophysiology: Understanding the Techniques and Defining the JargonFrom EverandDecoding Cardiac Electrophysiology: Understanding the Techniques and Defining the JargonAfzal SohaibNo ratings yet
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookFrom EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookNo ratings yet
- Appendicitis - ClinicalKeyDocument38 pagesAppendicitis - ClinicalKeyjpma2197No ratings yet
- AnemiaDocument10 pagesAnemiaRamesh VaradharajanNo ratings yet
- HYGIENEDocument3 pagesHYGIENECHRISTIAN ROY MAXINONo ratings yet
- Sensitivity Difference of Streptococcus Viridans On 35% Piper Betle Linn Extract and 10% Povidone Iodine Towards Recurrent Apthous StomatitisDocument7 pagesSensitivity Difference of Streptococcus Viridans On 35% Piper Betle Linn Extract and 10% Povidone Iodine Towards Recurrent Apthous StomatitisAhmad FadhilNo ratings yet
- WelchAllyn PIC30,40,50 Defibrillator - Service Manual PDFDocument289 pagesWelchAllyn PIC30,40,50 Defibrillator - Service Manual PDFandres2013bio100% (1)
- 2020 PRES and RCVSDocument8 pages2020 PRES and RCVSBryanNo ratings yet
- Neonatal Seizures: Lamiaa Mohsen, M.D Cairo UniversityDocument36 pagesNeonatal Seizures: Lamiaa Mohsen, M.D Cairo UniversityAdliah ZahiraNo ratings yet
- World Bispecific Summit Brochure v9Document20 pagesWorld Bispecific Summit Brochure v9Nadeem JamalNo ratings yet
- 6 2009 TylosinDocument37 pages6 2009 TylosinnickywulannNo ratings yet
- Chapter-1 Edi WowDocument8 pagesChapter-1 Edi WowJanette Cosip GaboNo ratings yet
- Eau Guidelines On Urological Infections: (Limited Text Update March 2022)Document27 pagesEau Guidelines On Urological Infections: (Limited Text Update March 2022)Andrea Romano ForcinitiNo ratings yet
- Angelman Syndrome Rough DraftDocument8 pagesAngelman Syndrome Rough Draftapi-540190838No ratings yet
- Neoplastic Disease 1Document69 pagesNeoplastic Disease 1Heba IyadNo ratings yet
- Failure of Crowns andDocument7 pagesFailure of Crowns anddr.nahlla hellesNo ratings yet
- Grammar 5aDocument1 pageGrammar 5aRaquel AsensioNo ratings yet
- IjdaDocument5 pagesIjdaSyed NooraniNo ratings yet
- Futuristic NursingDocument15 pagesFuturistic Nursingmanu sethi79% (19)
- Public Health PHD Thesis PDFDocument7 pagesPublic Health PHD Thesis PDFBuyingCollegePapersOnlineCanada100% (2)
- A Study On The PH of Commonly Used Soaps/cleansers Available in The Indian MarketDocument3 pagesA Study On The PH of Commonly Used Soaps/cleansers Available in The Indian MarketpalliNo ratings yet
- English PP2 Final Gauge PredictionDocument58 pagesEnglish PP2 Final Gauge PredictionGreg LanternNo ratings yet
- 2021 Infection PreventionDocument20 pages2021 Infection PreventionSamaki KubwaNo ratings yet
- Tuoren Price List (2022 Dec)Document5 pagesTuoren Price List (2022 Dec)satan ghostNo ratings yet
- Public Health Final Edited BlueprintDocument28 pagesPublic Health Final Edited BlueprintMoybon DegefaNo ratings yet
- English 5-Q4-L3 ModuleDocument13 pagesEnglish 5-Q4-L3 ModuleElaine Joyce GarciaNo ratings yet
- Clinical Case Scenarios Slide Set Powerpoint 247326013Document51 pagesClinical Case Scenarios Slide Set Powerpoint 247326013rwev3No ratings yet
- Adherence To Medication. N Engl J Med: New England Journal of Medicine September 2005Document12 pagesAdherence To Medication. N Engl J Med: New England Journal of Medicine September 2005Fernanda GilNo ratings yet
- s11882 018 0806 6 PDFDocument7 pagess11882 018 0806 6 PDFHildreth Rosel SabioNo ratings yet
- Pengetahuan Tentang Cacingan Dan Upaya Pencegahan Kecacingan Oleh: Ganda Sigalingging, Selli Dosriani Sitopu, Dita Wiranti DaeliDocument9 pagesPengetahuan Tentang Cacingan Dan Upaya Pencegahan Kecacingan Oleh: Ganda Sigalingging, Selli Dosriani Sitopu, Dita Wiranti DaeliMorida FanadierNo ratings yet