Download as pdf or txt
You might also like
- The Fauci COVID-19 DossierDocument205 pagesThe Fauci COVID-19 DossierStanko Fiser100% (8)
- Of Diseases and Related Health Problems (ICD-10) Contains Guidelines ForDocument29 pagesOf Diseases and Related Health Problems (ICD-10) Contains Guidelines FornorthernNo ratings yet
- ICD-11 An International Classification of DiseasesDocument11 pagesICD-11 An International Classification of DiseasesVictoria HavrylivNo ratings yet
- 5.ICD.10 Vol.1Document1,080 pages5.ICD.10 Vol.1isnainicoding27No ratings yet
- ICD-11 An International Classification of DiseasesDocument10 pagesICD-11 An International Classification of DiseasesMuhammad Farel Ikram MaulanaNo ratings yet
- WWW (1) .Who - Int Barra Classifications Barra Terminology Barra UstunDocument17 pagesWWW (1) .Who - Int Barra Classifications Barra Terminology Barra Ustunapi-3785090No ratings yet
- Pengenalan Icd-10 Struktur & IsiDocument15 pagesPengenalan Icd-10 Struktur & IsiL. JamilNo ratings yet
- The New Traumatic Dental Injury Classification of The World Health OrganizationDocument5 pagesThe New Traumatic Dental Injury Classification of The World Health OrganizationLia BaqueroNo ratings yet
- Who Pen 2020Document85 pagesWho Pen 2020Faye PalmaresNo ratings yet
- SEY-PEN (Package of Essential Non Communicable Diseases)Document85 pagesSEY-PEN (Package of Essential Non Communicable Diseases)Patrick CommettantNo ratings yet
- International Classification of Diseases Codes and Their Use in DentistryDocument15 pagesInternational Classification of Diseases Codes and Their Use in DentistryRekam Medis Puri Bunda MalangNo ratings yet
- The Selection and Use of Essential in Vitro Diagnostics: WHO Technical Report SeriesDocument380 pagesThe Selection and Use of Essential in Vitro Diagnostics: WHO Technical Report SeriesJOSHITHANo ratings yet
- Acute Medicine Surgery - 2022 - Ishizawa - Characteristics of Patients With Hip Fractures and Comorbid Fall RelatedDocument5 pagesAcute Medicine Surgery - 2022 - Ishizawa - Characteristics of Patients With Hip Fractures and Comorbid Fall RelatedSanja RhodesNo ratings yet
- ICD10Document1,080 pagesICD10Otniel Budi Krisetya100% (1)
- (2020) Revising The WHO Classication Female Genital Tract TumoursDocument7 pages(2020) Revising The WHO Classication Female Genital Tract TumourstungmapuNo ratings yet
- Resuscitator Systems Design GuidanceDocument21 pagesResuscitator Systems Design GuidanceRicardo Olmos Mentado100% (1)
- Pengenalan Icd-10 Struktur & IsiDocument16 pagesPengenalan Icd-10 Struktur & IsichintaNo ratings yet
- HIV The Question Is Not When To Treat, But How ToDocument1 pageHIV The Question Is Not When To Treat, But How ToHamza IlyasNo ratings yet
- 2018 05 29 Icd 11Document34 pages2018 05 29 Icd 11VahiraNo ratings yet
- Icd 11 Introduction ClinicalDocument50 pagesIcd 11 Introduction ClinicalMuhammad Farooq Ul HassanNo ratings yet
- Treatment Data Using A Topical Povidone-Iodine Antiseptic in Patients With Super Ficial Skin AbscessesDocument6 pagesTreatment Data Using A Topical Povidone-Iodine Antiseptic in Patients With Super Ficial Skin AbscessesADENo ratings yet
- GutjnlDocument8 pagesGutjnlfitriNo ratings yet
- Revising The WHO Classification: Female Genital Tract TumoursDocument6 pagesRevising The WHO Classification: Female Genital Tract TumoursAnna JuniedNo ratings yet
- The Impact of The COVID-19 Pandemic On Hip and Knee Arthroplasty: A Systematic ReviewDocument10 pagesThe Impact of The COVID-19 Pandemic On Hip and Knee Arthroplasty: A Systematic ReviewLasa SiahaanNo ratings yet
- Dental Traumatology - 2022 - Petti - NA0D The New Traumatic Dental Injury Classification of The World Health OrganizationDocument5 pagesDental Traumatology - 2022 - Petti - NA0D The New Traumatic Dental Injury Classification of The World Health OrganizationJAYASOORYAN S P M.D.S. CONSERVATIVE DENTISTRY AND ENDODONTICSNo ratings yet
- Pathology Lab GuidelinesDocument68 pagesPathology Lab GuidelinesLUZVIMINDA GORDO100% (1)
- 924154502X Eng HR PDFDocument587 pages924154502X Eng HR PDFSnufkin GreyNo ratings yet
- Icd NaDocument300 pagesIcd Naindah kristinaNo ratings yet
- Framework: For Collaborative Action On Tuberculosis and ComorbiditiesDocument88 pagesFramework: For Collaborative Action On Tuberculosis and ComorbiditiesRatnaNo ratings yet
- Ecsat WhoDocument126 pagesEcsat WhoDanty IndriastutyNo ratings yet
- Cross2014 - AnnRheumDis 1316 22Document9 pagesCross2014 - AnnRheumDis 1316 22Nitya KrishnaNo ratings yet
- Ijerph 19 02026 v2Document18 pagesIjerph 19 02026 v2Cihan ÖzdemirNo ratings yet
- WHO Recommended Test For TBDocument40 pagesWHO Recommended Test For TBJasminNo ratings yet
- Icd-10 01Document962 pagesIcd-10 01Phureephak JinopengNo ratings yet
- The Concept of The Family of Classification 1551867041Document10 pagesThe Concept of The Family of Classification 1551867041Jennie wuNo ratings yet
- Review of A Controversial Treatment Method in The Fight Against COVID-19 With The Example of AlgeriaDocument8 pagesReview of A Controversial Treatment Method in The Fight Against COVID-19 With The Example of AlgeriaHannah JanawaNo ratings yet
- Assessment of Activities of Daily Living in Patients Post COVID-19: A Systematic ReviewDocument18 pagesAssessment of Activities of Daily Living in Patients Post COVID-19: A Systematic Reviewjavieron11No ratings yet
- Key Features, Achievements and Challenges in Peru: Budgeting For Results in HealthDocument44 pagesKey Features, Achievements and Challenges in Peru: Budgeting For Results in HealthLaura Larrea MantillaNo ratings yet
- Erc ERC 23 0021Document10 pagesErc ERC 23 0021UnicornFlavoredNo ratings yet
- International Classification of Diseases: Presented By: DR Arijit Kundu Guided By: Prof. Sumitra PattanaikDocument56 pagesInternational Classification of Diseases: Presented By: DR Arijit Kundu Guided By: Prof. Sumitra PattanaikpriyagerardNo ratings yet
- Frotis SanguineoDocument4 pagesFrotis SanguineoMarcos RosalesNo ratings yet
- 10 3389@fdgth 2020 00008Document11 pages10 3389@fdgth 2020 00008Diego CornelioNo ratings yet
- Application of The International Classification of Diseases To Neurology (2nd Ed., 1997)Document586 pagesApplication of The International Classification of Diseases To Neurology (2nd Ed., 1997)I.m. DanielNo ratings yet
- TeleconsultationandTeletreatmentProtocoltoDiagnoseandManagePatientswithBenignParoxysmalPositionalVertigoBPPVduringtheCOVID 19pandemicDocument10 pagesTeleconsultationandTeletreatmentProtocoltoDiagnoseandManagePatientswithBenignParoxysmalPositionalVertigoBPPVduringtheCOVID 19pandemicMairaNo ratings yet
- Global, Regional Prevalence, Incidence and Risk Factors of Knee Osteoarthritis PopulationDocument13 pagesGlobal, Regional Prevalence, Incidence and Risk Factors of Knee Osteoarthritis PopulationnurjannahnasirNo ratings yet
- International Statistical Classification of Diseases and Related Health Problems, 10 Revision (ICD-10)Document2 pagesInternational Statistical Classification of Diseases and Related Health Problems, 10 Revision (ICD-10)Fern Insom-nyaNo ratings yet
- 4532ryDocument26 pages4532rySergio Sepúlveda GallegosNo ratings yet
- Paliatif WhoDocument72 pagesPaliatif WhoRuwaedaNasruddinNo ratings yet
- Assessing The Development of Palliative Care Worldwide: A Set of Actionable IndicatorsDocument72 pagesAssessing The Development of Palliative Care Worldwide: A Set of Actionable IndicatorsRanga PereraNo ratings yet
- WHO Consolidated Guideline On TB Module 1 PreventionDocument60 pagesWHO Consolidated Guideline On TB Module 1 PreventionDavid DwiputeraNo ratings yet
- Using X Ray Images and Deep Learning For Automated Detection of Coronavirus DiseaseDocument13 pagesUsing X Ray Images and Deep Learning For Automated Detection of Coronavirus DiseasebhattajagdishNo ratings yet
- Too Soon: Decade of Action On Preterm BirthDocument122 pagesToo Soon: Decade of Action On Preterm BirthNguyễn Đặng Tường Y2018No ratings yet
- COVID-19-Orthodontic Care During and After The Pandemic: A Narrative ReviewDocument15 pagesCOVID-19-Orthodontic Care During and After The Pandemic: A Narrative ReviewAndreea Andrei AndreeaNo ratings yet
- The Neurological Adaptation of Icd-10 (Icd-10 Na) : Jenny J. Van Drimmelen-KrabbeDocument2 pagesThe Neurological Adaptation of Icd-10 (Icd-10 Na) : Jenny J. Van Drimmelen-KrabbeNopriNo ratings yet
- Scleritis - EyeWikiDocument3 pagesScleritis - EyeWikiJorge Leonardo BedoyaNo ratings yet
- International Statistical Classification of Diseases and Related Health ProblemsDocument2,244 pagesInternational Statistical Classification of Diseases and Related Health ProblemsJemelito Constantino IINo ratings yet
- Nejmp1109150 PDFDocument3 pagesNejmp1109150 PDFAquaNo ratings yet
- Health Security Interventions for COVID-19 Response: Guidance NoteFrom EverandHealth Security Interventions for COVID-19 Response: Guidance NoteNo ratings yet
- The Race to Manufacture COVID-19 Vaccines: Emerging Vaccine TechnologiesFrom EverandThe Race to Manufacture COVID-19 Vaccines: Emerging Vaccine TechnologiesNo ratings yet
- Rift Valley Fever Action FrameworkFrom EverandRift Valley Fever Action FrameworkNo ratings yet
- Alternative FeedingDocument36 pagesAlternative FeedingEula Angelica OcoNo ratings yet
- Cold Chain SpotterDocument16 pagesCold Chain SpotterPravin SurendranNo ratings yet
- Ab Omas A L Ulceration Andtympanyofcalves: Tessa S. MarshallDocument12 pagesAb Omas A L Ulceration Andtympanyofcalves: Tessa S. Marshallana lauraNo ratings yet
- TII Textbook Complete Apr17Document634 pagesTII Textbook Complete Apr17CategoríaUno Lengua Inglesa COAPEHUMNo ratings yet
- Science 4Document34 pagesScience 4Giselle GiganteNo ratings yet
- Checklist Admin of MedsDocument5 pagesChecklist Admin of MedsKenneth SyNo ratings yet
- Triage Tool For UHCW Eye Casualty COVIDDocument5 pagesTriage Tool For UHCW Eye Casualty COVIDzahiraNo ratings yet
- Cece's Study Guides Part 1Document86 pagesCece's Study Guides Part 1Geraldine PatayanNo ratings yet
- Memorial-Case No 3Document20 pagesMemorial-Case No 3kajalpatil100% (2)
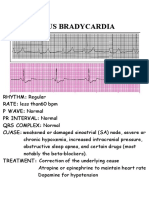
- Ecg NotesDocument16 pagesEcg NotesAszhiNo ratings yet
- Jurnal Reading - Kulit - I Nyoman Fidry Octora Young Amukty PDFDocument10 pagesJurnal Reading - Kulit - I Nyoman Fidry Octora Young Amukty PDFFidry YoungNo ratings yet
- BMC PsychiatryDocument18 pagesBMC PsychiatryLUIS FELIPE HENAONo ratings yet
- Bleeding: Mouth Nose Ear Urethra Vagina Anus SkinDocument3 pagesBleeding: Mouth Nose Ear Urethra Vagina Anus SkinJuliet Nillo RecepcionNo ratings yet
- Risk For Activity IntoleranceDocument2 pagesRisk For Activity IntoleranceBlessie FernandezNo ratings yet
- PDF The Integrated Nervous System A Systematic Diagnostic Case Based Approach 2Nd Edition Hendelman Ebook Full ChapterDocument49 pagesPDF The Integrated Nervous System A Systematic Diagnostic Case Based Approach 2Nd Edition Hendelman Ebook Full Chapterdavid.adams467100% (1)
- 744Document16 pages744Ruxandra DanuletNo ratings yet
- Pediatric Ophthalmology Anatomy and ExaminationDocument21 pagesPediatric Ophthalmology Anatomy and ExaminationGlydenne GayamNo ratings yet
- Cognitive Rehabilitation: A Goal-Planning Approach: Barbara A. Wilson, PHDDocument14 pagesCognitive Rehabilitation: A Goal-Planning Approach: Barbara A. Wilson, PHDMiguelySusy Ramos-RojasNo ratings yet
- What Is The Urinary System and How Does It Work?: KidneysDocument10 pagesWhat Is The Urinary System and How Does It Work?: KidneysAbdelrhman AboodaNo ratings yet
- 100-028-544 - ALLIANT SPORT PISTOL POWDER, 1LB - 69B - DefaultDocument13 pages100-028-544 - ALLIANT SPORT PISTOL POWDER, 1LB - 69B - DefaultDavid WilliamsNo ratings yet
- Viral Infection Host - Virus Interactions and Relationships and The Pathogenesis of Virus Disease Host-Virus InteractionsDocument3 pagesViral Infection Host - Virus Interactions and Relationships and The Pathogenesis of Virus Disease Host-Virus InteractionsOld LakeNo ratings yet
- Salin2 PPT ProposalDocument22 pagesSalin2 PPT ProposalSultan HSBNo ratings yet
- Women The Skilled Architect of The SocietyDocument4 pagesWomen The Skilled Architect of The SocietyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Pathology SGD 4: Diseases-Of-The-Immune-System: Group-4Document23 pagesPathology SGD 4: Diseases-Of-The-Immune-System: Group-4Kalpana JenaNo ratings yet
- AM19-Proceedings-Full ASCO PDFDocument652 pagesAM19-Proceedings-Full ASCO PDFrusgal8992100% (1)
- Hepar Sulph - The Homeopathic AntibioticDocument54 pagesHepar Sulph - The Homeopathic AntibioticGer DersenNo ratings yet
- Medical History Form (Only For International Exchange Students)Document1 pageMedical History Form (Only For International Exchange Students)Ana Romina Delfante VilaNo ratings yet
- Chelation BookDocument82 pagesChelation BookSean MoonshineNo ratings yet
- A Study On Work From Home, Motivation & Productivity of Employees in Indian Population During COVID-19 PandemicDocument15 pagesA Study On Work From Home, Motivation & Productivity of Employees in Indian Population During COVID-19 Pandemicمعن الفاعوريNo ratings yet
- Rishabh Letter Draft-1Document2 pagesRishabh Letter Draft-1Rishabh AgarwalNo ratings yet