Download as pdf or txt
You might also like
- CYCLES of Dev Pam LevinDocument5 pagesCYCLES of Dev Pam LevinRaul Arturo Velasco Rodríguez100% (2)
- Reflective QuestionsDocument2 pagesReflective Questionsayne joulceNo ratings yet
- Krishnamacharya's Practice Guidelines: Yoga Makaranda (1934) Yoga Makaranda (Part II) Yogasanagalu (1941)Document52 pagesKrishnamacharya's Practice Guidelines: Yoga Makaranda (1934) Yoga Makaranda (Part II) Yogasanagalu (1941)rashid_1806100% (1)
- CP2 MidtermsDocument278 pagesCP2 MidtermsDiana WadwasinNo ratings yet
- Metabolic Disese of LiverDocument52 pagesMetabolic Disese of LiverRashmi KATTINo ratings yet
- Hyperglycemia: Clinical Conditions of Carbohydrate MetabolismDocument4 pagesHyperglycemia: Clinical Conditions of Carbohydrate MetabolismCristel Magauay BanquirigNo ratings yet
- Inborn Errors or MetabolismDocument21 pagesInborn Errors or Metabolismsaleema11No ratings yet
- Lesson 7.1 Inborn Errors of MetabolismDocument119 pagesLesson 7.1 Inborn Errors of Metabolismmisaki06100% (2)
- DiabetesDocument52 pagesDiabetesAbdul HoqueNo ratings yet
- Paeda DMDocument38 pagesPaeda DMAmanuel LemiNo ratings yet
- Clinical SignificanceDocument31 pagesClinical Significancejav israelNo ratings yet
- Diabetes Mellitus: Prepared by Divya Bhusal B.SC - Nursing 3 YearDocument43 pagesDiabetes Mellitus: Prepared by Divya Bhusal B.SC - Nursing 3 YearSristi LamsalNo ratings yet
- DB31 - Pathophysiology of Diabetes Mellitus and HypoglycemiaDocument5 pagesDB31 - Pathophysiology of Diabetes Mellitus and HypoglycemiaNeil Alcazaren かわいいNo ratings yet
- Carbohydrate DisorderDocument74 pagesCarbohydrate DisorderEric YewNo ratings yet
- OMD-4 Diagnosis and Dental Managment of Diabetes Mellitus Lecture HandoutDocument13 pagesOMD-4 Diagnosis and Dental Managment of Diabetes Mellitus Lecture Handouthananalkadi94No ratings yet
- Assignment On BiochemistryDocument4 pagesAssignment On BiochemistryAIKA BAYANo ratings yet
- Storage DisordersDocument16 pagesStorage DisordersNithin DiwagarNo ratings yet
- Diabetes MellitusDocument3 pagesDiabetes MellitusShan NaseoulNo ratings yet
- Module 08 - Endocrine DisordersDocument43 pagesModule 08 - Endocrine DisordersKarina LojaNo ratings yet
- Diabetic Mellitus and Nursing ManagementDocument57 pagesDiabetic Mellitus and Nursing ManagementSukses TinggiNo ratings yet
- Emd2 k10 Hipoglisemia IniDocument16 pagesEmd2 k10 Hipoglisemia Ini103Juffry PrayogaNo ratings yet
- DIABETESDocument44 pagesDIABETESJessa MaeNo ratings yet
- Diah BingDocument10 pagesDiah BingDiah FebruarieNo ratings yet
- Emd166 Slide Acute Complication of DiabetesDocument78 pagesEmd166 Slide Acute Complication of DiabetesSukma WicaturatmashudiNo ratings yet
- Care of Clients With Glucose Metabolism ProblemsDocument5 pagesCare of Clients With Glucose Metabolism ProblemsRyel Lixel DivinagraciaNo ratings yet
- Patologi Pankreas Endokrin & AdrenalDocument69 pagesPatologi Pankreas Endokrin & AdrenalSonia Afika AzizaNo ratings yet
- Chap 135Document6 pagesChap 135Jalajarani AridassNo ratings yet
- Case PresentationDocument12 pagesCase PresentationnatashafiroshNo ratings yet
- Endocrine & Metabolic DisordersDocument38 pagesEndocrine & Metabolic DisordersBala UrmarNo ratings yet
- Seminar DMDocument42 pagesSeminar DMRubina MasihNo ratings yet
- The Endocrine Pancreas IIDocument134 pagesThe Endocrine Pancreas IIHoque Mohammed Newaz ShorifulNo ratings yet
- Diabetes MellitusDocument18 pagesDiabetes MellitusAadhan ArveeNo ratings yet
- Chem-Reviewer cDocument9 pagesChem-Reviewer cserdeniamarilen393No ratings yet
- Carbohydrate Metabolism Disorders Stom 10-11Document61 pagesCarbohydrate Metabolism Disorders Stom 10-11Artem GrigoryanNo ratings yet
- Hypoglycemia UMYDocument60 pagesHypoglycemia UMYTommy AkromaNo ratings yet
- s2 Ikd Willy 2016Document16 pagess2 Ikd Willy 2016Muhammad Ali MashuriNo ratings yet
- Clinical Biochemical Investigations For Inborn Errors of MetabolismDocument19 pagesClinical Biochemical Investigations For Inborn Errors of Metabolismzain and mariamNo ratings yet
- Endocrine - DI, DM I & II 04/13/2016: Review of Endocrine Pancreas: Endocrine and Exocrine Gland Alpha CellsDocument6 pagesEndocrine - DI, DM I & II 04/13/2016: Review of Endocrine Pancreas: Endocrine and Exocrine Gland Alpha Cellsapi-314805004No ratings yet
- Blok Sistem Metabolik & Endokrin (2015)Document107 pagesBlok Sistem Metabolik & Endokrin (2015)Pretty HiaNo ratings yet
- Diabetes Mellitus - Nursing CareDocument51 pagesDiabetes Mellitus - Nursing CareJoice DasNo ratings yet
- Endocrine Disorders: Patho Phys Iolog yDocument20 pagesEndocrine Disorders: Patho Phys Iolog yCres Padua QuinzonNo ratings yet
- Group 8: Reporters: Marjorie D. Vesido Franklin "Mama" Abdon Jenny "Hermes" Mendoza Mark Cyrus SangcoDocument37 pagesGroup 8: Reporters: Marjorie D. Vesido Franklin "Mama" Abdon Jenny "Hermes" Mendoza Mark Cyrus Sangcoacidic1217ixNo ratings yet
- Supplementary Information To Chapter 32: Inborn Errors of Metabolism General ConsiderationsDocument24 pagesSupplementary Information To Chapter 32: Inborn Errors of Metabolism General ConsiderationsAaron JoseNo ratings yet
- Diabetes Melitus: Dr. Ihsanil Husna, SPPDDocument67 pagesDiabetes Melitus: Dr. Ihsanil Husna, SPPDnathan timothyNo ratings yet
- Pathophysiology of Carbohydrates MetabolismDocument54 pagesPathophysiology of Carbohydrates MetabolismMaui TingNo ratings yet
- Malabsorption ANGOLDocument30 pagesMalabsorption ANGOLAvramut IulianNo ratings yet
- Blood GlucoseDocument8 pagesBlood Glucoseعبدالرحمن عابدNo ratings yet
- Endocrine Emergencies: Lynn K. Wittwer, MD MPD Clark County EMSDocument37 pagesEndocrine Emergencies: Lynn K. Wittwer, MD MPD Clark County EMSSyahril FauziNo ratings yet
- Glycogen Storage Disease (GSD) Type IVDocument26 pagesGlycogen Storage Disease (GSD) Type IVAnonymous t5TDwdNo ratings yet
- Diabetes Mellitus 1Document5 pagesDiabetes Mellitus 1Xarius FidelNo ratings yet
- Diabetes Mellitus Type2: Case StudyDocument48 pagesDiabetes Mellitus Type2: Case StudyJohn Carlo GarciaNo ratings yet
- Diabetes Mellitus: WAHYUDI, S.Farm., AptDocument31 pagesDiabetes Mellitus: WAHYUDI, S.Farm., AptMayesti FransiskaNo ratings yet
- DIABETES MELLITUS Presentation (1) .PPTMDocument124 pagesDIABETES MELLITUS Presentation (1) .PPTMfrankNo ratings yet
- Diabetes Mellitus LectureDocument68 pagesDiabetes Mellitus LectureDikyAksiramNo ratings yet
- Diabetes Mellitus: NCM 116 Metabolism & Endocrine BSN 3Document19 pagesDiabetes Mellitus: NCM 116 Metabolism & Endocrine BSN 3Karen Kate AblesNo ratings yet
- Review Notes For Diabetes MellitusDocument8 pagesReview Notes For Diabetes MellitusEditha LucasNo ratings yet
- Diabetes MellitusDocument26 pagesDiabetes MellitusKamlesh KishorNo ratings yet
- Dks HhsDocument16 pagesDks HhsDebora Putri Fernanda SaragihNo ratings yet
- GSDDocument26 pagesGSDFahad Ali NadeemNo ratings yet
- Diabetes MellitusDocument77 pagesDiabetes MellitusAshok100% (7)
- Diabetes MellitusDocument79 pagesDiabetes Mellituskhalid saifur rahman khanNo ratings yet
- Von Gierke Disease, (Glycogen Storage Disorder I) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandVon Gierke Disease, (Glycogen Storage Disorder I) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Katie ErikssonDocument20 pagesKatie ErikssonAltheia Fei EnriquezNo ratings yet
- QUARTER-1-EFDT - MATH 10 Learning-PlanDocument11 pagesQUARTER-1-EFDT - MATH 10 Learning-PlanFaculty SFANo ratings yet
- Research ActivitiesDocument8 pagesResearch ActivitiesJacqueline Acera BalingitNo ratings yet
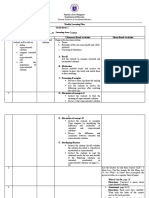
- Weekly Learning Plan Q1 Week 7Document3 pagesWeekly Learning Plan Q1 Week 7sagiNo ratings yet
- Adept Heterostruct TutorialDocument23 pagesAdept Heterostruct TutorialLavi TyagiNo ratings yet
- DLP 1 - Math2q1Document2 pagesDLP 1 - Math2q1Rogelio Jr AsisNo ratings yet
- Es 14Document394 pagesEs 14carlodolciNo ratings yet
- Resume WBSD - Wbms Ap - Degrand2021Document3 pagesResume WBSD - Wbms Ap - Degrand2021api-277190928No ratings yet
- Curriculum VitaeDocument3 pagesCurriculum VitaeShibu ThomasNo ratings yet
- Grade 6 - PPT - Tle-Ict - w4Document74 pagesGrade 6 - PPT - Tle-Ict - w4lynaibel.seguiNo ratings yet
- Cherubin Garden RatesDocument6 pagesCherubin Garden RatesJJ PernitezNo ratings yet
- A-Strength Based Perspective OaDocument20 pagesA-Strength Based Perspective OakkurtbrylleNo ratings yet
- Apex ComputersDocument3 pagesApex ComputersSusheel Kumar100% (1)
- Kurukshetra University Kurukshetra: For Admission To Ph.D. Course Through Entrance Test For The Academic Session 2019-20Document8 pagesKurukshetra University Kurukshetra: For Admission To Ph.D. Course Through Entrance Test For The Academic Session 2019-20Deep SidhuNo ratings yet
- BESCK104DDocument4 pagesBESCK104DNithin Gowdru0% (1)
- Doctor of Business Administration Dissertation SamplesDocument8 pagesDoctor of Business Administration Dissertation SamplesWebsiteThatWillWriteAPaperForYouSavannahNo ratings yet
- Voice RecogDocument25 pagesVoice RecogAnkita HatwarNo ratings yet
- Plan Business Analysis Information ManagementDocument2 pagesPlan Business Analysis Information Managementsonam tiwariNo ratings yet
- Manythings Handout 2005Document1 pageManythings Handout 2005GyurmedNo ratings yet
- Petition Letter To SKDocument2 pagesPetition Letter To SKJasmine SingletonNo ratings yet
- Executive SummeryDocument3 pagesExecutive SummerySyahlul MahfuzhNo ratings yet
- Armed Forces Institute of Radiology & Imaging: Reg NoDocument5 pagesArmed Forces Institute of Radiology & Imaging: Reg NoMahamnoorNo ratings yet
- Sri Chaitanya IIT Academy., India.: Key SheetDocument10 pagesSri Chaitanya IIT Academy., India.: Key SheetsumanthNo ratings yet
- Evolution of Teachers Technology Integration Knowledge Beliefs and Practices How Can We Support Beginning Teachers Use of TechnologyDocument24 pagesEvolution of Teachers Technology Integration Knowledge Beliefs and Practices How Can We Support Beginning Teachers Use of Technologybeatriz cabellosNo ratings yet
- Experience Gokul BoopathiDocument4 pagesExperience Gokul BoopathiKeerthi VarshiniNo ratings yet
- Lesson Plan 1 - PolygonsDocument3 pagesLesson Plan 1 - Polygonsapi-534905186No ratings yet
- Communities in Cyberspace Kollock PDFDocument2 pagesCommunities in Cyberspace Kollock PDFDawnNo ratings yet