Download as pdf or txt
You might also like
- Embalming History Theory and Practice Fifth Edition Ebook PDF VersionDocument62 pagesEmbalming History Theory and Practice Fifth Edition Ebook PDF Versionadolfo.milliken178100% (52)
- Unit IG2: Risk AssessmentDocument13 pagesUnit IG2: Risk AssessmentNauman Qureshi91% (11)
- Management-Of-Mutilated-Teeth - (1) (1) - 1Document57 pagesManagement-Of-Mutilated-Teeth - (1) (1) - 1Khushboo Gupta75% (4)
- TCMDocument4 pagesTCMxuxumoNo ratings yet
- COVID-19 Pandemic On Global Polio EradicationDocument7 pagesCOVID-19 Pandemic On Global Polio EradicationRai AlfiahNo ratings yet
- Polio by The Numbers-A Global PerspectiveDocument10 pagesPolio by The Numbers-A Global PerspectiveSaminur FauzanNo ratings yet
- MainDocument9 pagesMainSURYONONo ratings yet
- WTP Assessment COVID VaccineDocument6 pagesWTP Assessment COVID VaccineGeorge DomNo ratings yet
- Impact of The COVID 19 Pandemic On Adolescent Vaccinations Projected Time To Reverse Deficits in Routine Adolescent Vaccination in The United StatesDocument12 pagesImpact of The COVID 19 Pandemic On Adolescent Vaccinations Projected Time To Reverse Deficits in Routine Adolescent Vaccination in The United StatesArumm88No ratings yet
- Vaksin 2Document9 pagesVaksin 2Arumm88No ratings yet
- Willingness-To-Pay For A COVID-19 Vaccine and Its Associated Determinants in IndonesiaDocument8 pagesWillingness-To-Pay For A COVID-19 Vaccine and Its Associated Determinants in IndonesianovireandysasmitaNo ratings yet
- 1 s2.0 S1477893921000375 MainDocument3 pages1 s2.0 S1477893921000375 MainjimiNo ratings yet
- Safety Science: SciencedirectDocument2 pagesSafety Science: SciencedirectYat SonNo ratings yet
- Concepts in Disaster MedicineDocument8 pagesConcepts in Disaster MedicinedaniaNo ratings yet
- Alam Et Al. - 2021 - Challenges To COVID-19 Vaccine Supply Chain ImpliDocument16 pagesAlam Et Al. - 2021 - Challenges To COVID-19 Vaccine Supply Chain Impliprat.nitjsrNo ratings yet
- Lilliput COVID-19: Vaccination ProblemsDocument13 pagesLilliput COVID-19: Vaccination ProblemscitraNo ratings yet
- Public Policy Lessons From The Covid 19 Outbreak: How To Deal With It in The Post Pandemic World?Document14 pagesPublic Policy Lessons From The Covid 19 Outbreak: How To Deal With It in The Post Pandemic World?MeemNo ratings yet
- Editorial: Global Health May 2020 Editorial. To LongitudinallyDocument1 pageEditorial: Global Health May 2020 Editorial. To Longitudinallyjei5003No ratings yet
- Clinical Outcomes of A COVID-19 Vaccine: Implementation Over EfficacyDocument19 pagesClinical Outcomes of A COVID-19 Vaccine: Implementation Over EfficacyIraNo ratings yet
- Running Head: Benefits of The Covid-19 Vaccine 1Document7 pagesRunning Head: Benefits of The Covid-19 Vaccine 1bonnieNo ratings yet
- The Impact of COVID 19 Vaccination On Stock Market Is There Any Di 2022 HelDocument8 pagesThe Impact of COVID 19 Vaccination On Stock Market Is There Any Di 2022 HelMixa TekluNo ratings yet
- Readersdpiis2468042722000069token &OriginRegion Us East 1&OriginCreationDocument13 pagesReadersdpiis2468042722000069token &OriginRegion Us East 1&OriginCreationMelanie Anaud Magro-AmosNo ratings yet
- COVID Macro ScenariosDocument45 pagesCOVID Macro ScenariosEsteban Andrés Pullas100% (1)
- Covid 19Document16 pagesCovid 19Mazia MansoorNo ratings yet
- 2021 Article 26475Document10 pages2021 Article 26475JefrioSuyantoNo ratings yet
- PolioPipeline 08Document8 pagesPolioPipeline 08Subhajit BhattacharjeeNo ratings yet
- SSRN Id3547729Document45 pagesSSRN Id3547729Anita BedónNo ratings yet
- Benefit of Covid-19 VaccineDocument9 pagesBenefit of Covid-19 VaccineKevo KarisNo ratings yet
- Warnings Regarding The Potential Coronavirus Disease 2019 Covid 19 Transmission Risk Vaccination Is Not EnoughDocument1 pageWarnings Regarding The Potential Coronavirus Disease 2019 Covid 19 Transmission Risk Vaccination Is Not Enoughfrancheskaam27No ratings yet
- Covid ImpactDocument9 pagesCovid ImpactAlejandro Gabriel ArancibiaNo ratings yet
- Controlo Da Pandemia em Portugal Na Fase Da VacinaçãoDocument15 pagesControlo Da Pandemia em Portugal Na Fase Da VacinaçãopedromelaoNo ratings yet
- The Use of The Health Belief Model To Assess Predictors of Intent To Receive The COVID 19 Vaccine and Willingness To PayDocument12 pagesThe Use of The Health Belief Model To Assess Predictors of Intent To Receive The COVID 19 Vaccine and Willingness To PayMuhammad ImranNo ratings yet
- Hib ArticleDocument7 pagesHib ArticlePhoebe CubarrubiaNo ratings yet
- Global Impact of The First Year of COVID-19 VaccinationDocument10 pagesGlobal Impact of The First Year of COVID-19 VaccinationStavya DubeyNo ratings yet
- Playing Fiddle While The World Burns - PrEP4AllDocument14 pagesPlaying Fiddle While The World Burns - PrEP4AlllbernsteinNo ratings yet
- EJ1351173Document8 pagesEJ1351173adaamibny07No ratings yet
- Global Incidence, Prevalence, Years Lived With Disability YLDs, Disability-Adjusted Life-YearsDocument29 pagesGlobal Incidence, Prevalence, Years Lived With Disability YLDs, Disability-Adjusted Life-Yearsluis sanchezNo ratings yet
- Deb PDocument19 pagesDeb PJean M Huaman FiallegaNo ratings yet
- Reflections On Modeling Poliovirus Transmission and The Polio Eradication EndgameDocument19 pagesReflections On Modeling Poliovirus Transmission and The Polio Eradication EndgameBolohan BiatriceNo ratings yet
- Vaccines 10 01714 v2Document21 pagesVaccines 10 01714 v2Irene KoutsodontiNo ratings yet
- 8 PDFDocument10 pages8 PDFLuciana MihaelaNo ratings yet
- The Effect of The COVID-19 Vaccine On Daily Cases and Deaths Based On Global Vaccine DataDocument12 pagesThe Effect of The COVID-19 Vaccine On Daily Cases and Deaths Based On Global Vaccine DataCorneliu PaschanuNo ratings yet
- 1 s2.0 S1755436524000240 MainDocument10 pages1 s2.0 S1755436524000240 Main7fkqx7zh7pNo ratings yet
- Antes e Durante PandemiaDocument10 pagesAntes e Durante Pandemiapallomabarbosa.biomedNo ratings yet
- Polio Eradication Falling at The Final HurdleDocument1 pagePolio Eradication Falling at The Final HurdlesandeepskareNo ratings yet
- Epidemiologie - Mesures de Controle Et Prevention: Lettre Coronavirus Covid-19Document13 pagesEpidemiologie - Mesures de Controle Et Prevention: Lettre Coronavirus Covid-19Alexandra IonițăNo ratings yet
- A Two-Phase Stochastic Dynamic Model For COVID-19 Mid-Term Policy Recommendations in Greece: A Pathway Towards Mass VaccinationDocument21 pagesA Two-Phase Stochastic Dynamic Model For COVID-19 Mid-Term Policy Recommendations in Greece: A Pathway Towards Mass VaccinationiFellixeNo ratings yet
- Microbial Biotechnology - 2022 - BR Ssow - Can A Combination of Vaccination and Face Mask Wearing Contain The COVID 19Document17 pagesMicrobial Biotechnology - 2022 - BR Ssow - Can A Combination of Vaccination and Face Mask Wearing Contain The COVID 19Caryl DagamiNo ratings yet
- Can Phytotherapy With Polyphenols Serve As A Powerful Approach For The Prevention and Therapy Tool of Novel Coronavirus Disease 2019? 2020Document20 pagesCan Phytotherapy With Polyphenols Serve As A Powerful Approach For The Prevention and Therapy Tool of Novel Coronavirus Disease 2019? 2020Kelly DickinsonNo ratings yet
- Como A Pandemia de COVID-19 Mudou As Atitudes de Vacinação Contra A Gripe Entre Os Profissionais de Saúde de Um Centro de Câncer ItalianoDocument7 pagesComo A Pandemia de COVID-19 Mudou As Atitudes de Vacinação Contra A Gripe Entre Os Profissionais de Saúde de Um Centro de Câncer ItalianoArquivo FisioNo ratings yet
- Strict Lockdown Versus Flexible Social Distance Strategy For Covid19 DiseaseDocument6 pagesStrict Lockdown Versus Flexible Social Distance Strategy For Covid19 DiseaseHaleluya LeulsegedNo ratings yet
- Interim Statement On COVID-19 Vaccines in The Context of The Circulation of The Omicron SARS-CoV-2 Variant From The WHO Technical Advisory Group On COVID-19 Vaccine Composition (TAG-CO-VAC)Document5 pagesInterim Statement On COVID-19 Vaccines in The Context of The Circulation of The Omicron SARS-CoV-2 Variant From The WHO Technical Advisory Group On COVID-19 Vaccine Composition (TAG-CO-VAC)Sneha SinghNo ratings yet
- HotezDocument6 pagesHotezapi-547285914No ratings yet
- The Lancet VaccinationDocument19 pagesThe Lancet VaccinationyosefNo ratings yet
- 1 s2.0 S0377221720306913 MainDocument17 pages1 s2.0 S0377221720306913 Mainsupartyani wayanNo ratings yet
- Impacts of COVID-19Document43 pagesImpacts of COVID-19ShahRukh YunasNo ratings yet
- Chapter 5Document12 pagesChapter 5Nikhil ShuklaNo ratings yet
- WHO WHE SPP 2023.1 EngDocument20 pagesWHO WHE SPP 2023.1 Engpenelitian.shellyNo ratings yet
- SceirdDocument9 pagesSceirdGiaWay HsuNo ratings yet
- Covid 19.edited (1) .EditedDocument16 pagesCovid 19.edited (1) .EditedMORRIS ANUNDANo ratings yet
- Who Strategic Action Against COVID 19: 2021 Mid-Year ReportDocument26 pagesWho Strategic Action Against COVID 19: 2021 Mid-Year ReportJeyp MacaroyNo ratings yet
- Vaccine: Michele Kohli, Michael Maschio, Debbie Becker, Milton C. WeinsteinDocument8 pagesVaccine: Michele Kohli, Michael Maschio, Debbie Becker, Milton C. Weinsteinfareha riazNo ratings yet
- Pandemic Preparedness and Response Strategies: COVID-19 Lessons from the Republic of Korea, Thailand, and Viet NamFrom EverandPandemic Preparedness and Response Strategies: COVID-19 Lessons from the Republic of Korea, Thailand, and Viet NamNo ratings yet
- Dr. Djohan Ardiansyah, SP.S (K)Document60 pagesDr. Djohan Ardiansyah, SP.S (K)satyagraha84No ratings yet
- Skripsi Tanpa Bab PembahasanDocument75 pagesSkripsi Tanpa Bab PembahasanIndah NNo ratings yet
- Part 1:-Safety On Workplace: Q 1) What Are The Health Hazards Mentioned inDocument5 pagesPart 1:-Safety On Workplace: Q 1) What Are The Health Hazards Mentioned inSalman AlshammariNo ratings yet
- A Guide To Well-BeingDocument111 pagesA Guide To Well-BeingAtul Pant100% (2)
- MEDICAL IMAGING Updated 2022Document25 pagesMEDICAL IMAGING Updated 2022Mengot Ashu RoseNo ratings yet
- Justice and Solicitor General Letter To Edmonton Mayor Public Safety 2022-05-26Document3 pagesJustice and Solicitor General Letter To Edmonton Mayor Public Safety 2022-05-26edmontonjournalNo ratings yet
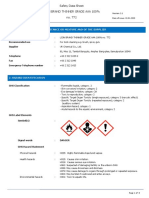
- MSDS - Thinner AAADocument8 pagesMSDS - Thinner AAAShafri ArifinNo ratings yet
- Project Feasibility Study and Evaluation 2011 Sports ComplexDocument264 pagesProject Feasibility Study and Evaluation 2011 Sports ComplexFongbeerNo ratings yet
- Should Drug Users Should Be Punish or HelpDocument25 pagesShould Drug Users Should Be Punish or HelpMaria Sandara PatajoNo ratings yet
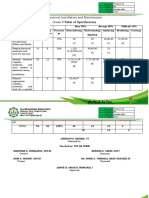
- Q1 Tle 9 Eim TosDocument2 pagesQ1 Tle 9 Eim TosjuzielouNo ratings yet
- Vaksin Influenza OverviewDocument27 pagesVaksin Influenza OverviewMaria Astika DewiNo ratings yet
- Erythroblastosis FetalisDocument3 pagesErythroblastosis FetalissolegrinNo ratings yet
- Political FrameDocument5 pagesPolitical Frameapi-523050935No ratings yet
- Jammu and Kashmir Delimitation: FactoidDocument4 pagesJammu and Kashmir Delimitation: Factoidsaumya bargotiNo ratings yet
- Bibliotherapy: Books As TherapyDocument33 pagesBibliotherapy: Books As TherapyNOR AZIRA BINTI AZIZ MoeNo ratings yet
- 2301B Dental Unit Manual-BeingDocument22 pages2301B Dental Unit Manual-BeingMr.SDNo ratings yet
- Dwnload Full Nursing For Wellness in Older Adults 7th Edition Miller Test Bank PDFDocument35 pagesDwnload Full Nursing For Wellness in Older Adults 7th Edition Miller Test Bank PDFmichaelcalhounjtypaegbnk100% (13)
- Color BlindnessDocument3 pagesColor BlindnessRainZZaKNo ratings yet
- F071-003 Your Company's Risk Management - Upon Receipt of Order 020312Document5 pagesF071-003 Your Company's Risk Management - Upon Receipt of Order 020312BALAJINo ratings yet
- Paggamot Sa Gitna NG PaggahasaDocument4 pagesPaggamot Sa Gitna NG PaggahasaOmar AculanNo ratings yet
- Jurnal Keperawatan Muhammadiyah: Pelangi Jiwa Aobama, Dedy PurwitoDocument11 pagesJurnal Keperawatan Muhammadiyah: Pelangi Jiwa Aobama, Dedy PurwitoVania Petrina CalistaNo ratings yet
- Katalog 27 September 2021Document28 pagesKatalog 27 September 2021Rafael BagusNo ratings yet
- Virtual Lab Tour Format - AgsaldaDocument2 pagesVirtual Lab Tour Format - AgsaldaEj AgsaldaNo ratings yet
- Posture and Factor Affecting Posture in Physical TherapyDocument28 pagesPosture and Factor Affecting Posture in Physical TherapyAnand Vaghasiya100% (2)
- Fit Aq Module 2 - Unit1Document26 pagesFit Aq Module 2 - Unit1REVELNo ratings yet
- Cmca Lec ReviewerDocument32 pagesCmca Lec Reviewercuteathena11No ratings yet