Professional Documents
Culture Documents
Trimaran and Trigger Study
Trimaran and Trigger Study
Uploaded by
mytriciallorinCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Trimaran and Trigger Study
Trimaran and Trigger Study
Uploaded by
mytriciallorinCopyright:
Available Formats
Articles
Single inhaler extrafine triple therapy in uncontrolled
asthma (TRIMARAN and TRIGGER): two double-blind,
parallel-group, randomised, controlled phase 3 trials
Johann Christian Virchow*, Piotr Kuna, Pierluigi Paggiaro, Alberto Papi, Dave Singh, Sandrine Corre, Florence Zuccaro, Andrea Vele, Maxim Kots,
George Georges, Stefano Petruzzelli, Giorgio Walter Canonica*
Summary
Background To date, no studies have assessed the efficacy of single-inhaler triple therapy in asthma. Here we report on Published Online
two studies that compared the single-inhaler extrafine combination of beclometasone dipropionate (BDP; inhaled September 30, 2019
https://doi.org/10.1016/
corticosteroid), formoterol fumarate (FF; long-acting β2 agonist), and glycopyrronium (G; long-acting muscarinic S0140-6736(19)32215-9
antagonist) with the combination of BDP with FF.
See Online/Comment
https://doi.org/10.1016/
Methods Two parallel-group, double-blind, randomised, active-controlled, phase 3 trials (Triple in Asthma With S0140-6736(19)32216-0
Uncontrolled Patients on Medium Strength of ICS + LABA [TRIMARAN] and Triple in Asthma High Strength *Contributed equally
Versus ICS/LABA HS and Tiotropium [TRIGGER]) recruited patients from 171 sites across 16 countries Universitätsmedizin Rostock,
(TRIMARAN), and from 221 sites across 17 countries (TRIGGER). The sites were a mixture of secondary and Zentrum für Innere Medizin,
tertiary care centres and specialised investigation units. Eligible patients were adults (aged 18–75 years) with Abteilung für Pneumologie,
Rostock, Germany
uncontrolled asthma, a history of one or more exacerbations in the previous year, and previously treated with (Prof J C Virchow MD); Division
inhaled corticosteroid (TRIMARAN: medium dose; TRIGGER: high dose) plus a long-acting β2 agonist. Enrolled of Internal Medicine, Asthma
patients were initially treated with BDP/FF (TRIMARAN: 100 μg BDP and 6 µg FF; TRIGGER: 200 μg BDP and and Allergy, Medical University
6 µg FF) for 2 weeks, then randomly assigned to treatment using an interactive response technology system with of Łódź, Łódź, Poland
(Prof P Kuna MD); Department
a balanced block randomisation scheme stratified by country. Patients, investigators, site staff, and sponsor staff of Surgery, Medicine, Molecular
were masked to BDP/FF/G and BDP/FF assignment. In TRIMARAN, patients were randomly assigned (1:1) to Biology, and Critical Care,
52 weeks of BDP/FF/G (100 μg BDP, 6 μg FF, and 10 μg G) or BDP/FF (100 μg BDP and 6 µg FF), two inhalations University of Pisa, Pisa, Italy
(Prof P Paggiaro MD); Section of
twice daily. In TRIGGER, patients were randomly assigned (2:2:1) to 52 weeks of BDP/FF/G (200 μg BDP, 6 μg FF,
Cardiorespiratory and Internal
and 10 µg G) or BDP/FF (200 BDP and 6 µg FF), both two inhalations twice daily, or open-label BDP/FF (200 μg BDP Medicine, Department of
and 6 µg FF) two inhalations twice daily plus tiotropium 2·5 µg two inhalations once daily. Coprimary endpoints Medical Sciences, University of
for both trials (BDP/FF/G vs BDP/FF) were pre-dose forced expiratory volume in 1 s (FEV1) at week 26 and rate of Ferrara, Ferrara, Italy
(Prof A Papi MD); Medicines
moderate and severe exacerbations over 52 weeks. Safety was assessed in all patients who received at least one
Evaluation Unit, The University
dose of study treatment. These trials were registered with ClinicalTrials.gov, NCT02676076 (TRIMARAN), of Manchester, Manchester
NCT02676089 (TRIGGER). University NHS Foundation
Trust, Manchester, UK
(Prof D Singh MD); Global
Findings Between Feb 17, 2016, and May 17, 2018, 1155 patients in TRIMARAN were given BDP/FF/G (n=579) or
Clinical Development, Chiesi
BDP/FF (n=576). Between April 6, 2016, and May 28, 2018, 1437 patients in TRIGGER were given BDP/FF/G (n=573), Farmaceutici, Parma, Italy
BDP/FF (n=576), or BDP/FF plus tiotropium (n=288). Compared with the BDP/FF group, week 26 predose FEV1 (S Corre MSc, F Zuccaro MSc,
improved in the BDP/FF/G group by 57 mL (95% CI 15–99; p=0·0080) in TRIMARAN and by 73 mL (26–120; p=0·0025) A Vele MSc, M Kots MD,
G Georges MD, S Petruzzelli MD);
in TRIGGER, with reductions in the rate of moderate and severe exacerbations of 15% (rate ratio 0·85, 95% CI
and Humanitas University and
0·73–0·99; p=0·033) in TRIMARAN and 12% (0·88, 0·75–1·03; p=0·11) in TRIGGER. Four patients had treatment- Research Hospital, Center of
related serious adverse events, one in TRIMARAN in the BDP/FF/G group and three in TRIGGER—one in the Personalized Medicine: Asthma
BDP/FF/G and two in the BDP/FF group. Three patients in the BDP/FF/G group in TRIMARAN and two patients in and Allergy, Milan, Italy
(Prof G W Canonica MD)
TRIGGER—one in the BDP/FF/G group and one in the BDP/FF group—had adverse events leading to death. None of
Correspondence to:
the deaths were considered as related to treatment.
Prof J Christian Virchow,
Universitätsmedizin Rostock,
Interpretation In uncontrolled asthma, addition of a long-acting muscarinic antagonist to inhaled corticosteroid plus Zentrum für Innere Medizin,
long-acting β2-agonist therapy improves lung function and reduces exacerbations. Medizinische Klinik,
Abteilung Pneumologie and
Interdisziplinäre Internistische
Funding Chiesi Farmaceutici. Intensivmedizin, Rostock 18057,
Germany
Copyright © 2019 Elsevier Ltd. All rights reserved. j.c.virchow@med.uni-rostock.de
Introduction of chronic airway inflammation; hence inhaled cortico
Goals of asthma management are to achieve symptom steroids are the mainstay of therapy.1 Many patients are
control and avoid future risks, especially risks of able to achieve good disease control, especially from
exacerbations.1 Asthma is characterised by the presence an inhaled corticosteroid plus long-acting β2 agonist
www.thelancet.com Published online September 30, 2019 https://doi.org/10.1016/S0140-6736(19)32215-9 1
Articles
Research in context
Evidence before this study tiotropium to inhaled corticosteroid plus a long-acting
We searched PubMed for articles published from database β2 agonist, which was similar to inhaled corticosteroid plus a
inception until April 4, 2019, using the search term “drug long-acting β2 agonist alone. In the third article, the addition of
therapy, combination" [MeSH terms] OR triple AND asthma tiotropium improved airflow and reduced airway wall thickness
AND trial NOT theophylline NOT montelukast, with no after 48 weeks. All three studies assessed the effect of
restrictions. Of the 1068 hits, eight articles presented data from tiotropium plus inhaled corticosteroid plus long-acting
clinical trials that assessed the efficacy of triple therapy β2-agonist therapy in patients with spirometrically assessed
comprising an inhaled corticosteroid plus a long-acting persistent airflow limitation (ie, ratio of forced expiratory
β2 agonist plus a long-acting muscarinic antagonist. Of these volume in 1 s to forced vital capacity <0·7).
articles, six reported data in adults (the other two reported data
Added value of this study
in children or adolescents), of which one article was a
TRIMARAN and TRIGGER are the first studies to assess the
short-term (4-week) study, one reported pooled safety data,
efficacy and safety of single-inhaler triple therapy compared
and one reported subgroup analyses of studies presented in
with inhaled corticosteroid plus a long-acting β2 agonist in
another manuscript. The remaining three articles reported data
adults with asthma. Additionally, these are the first long-term
from studies in which the long-acting muscarinic antagonist
studies undertaken in patients who had no requirement to show
tiotropium was added as a free combination to any inhaled
persistent airflow limitation after short-acting β2 agonist use.
corticosteroid and long-acting β2 agonist. The first of these
articles presented data from two 48-week studies, in which the Implications of all the available evidence
addition of tiotropium to high-dose inhaled corticosteroid plus The combination of a long-acting muscarinic antagonist with
a long-acting β2 agonist delayed the time to first asthma an inhaled corticosteroid plus long-acting β2-agonist therapy in
exacerbation and reduced the overall risk of these events, adults with uncontrolled asthma results in improved lung
with improvements in lung function. The second article focused function. In large, long-term studies, triple therapy has a
on the long-term (52-week) safety profile of the addition of positive effect on severe exacerbations.
combination.2 However, until recently, few options were In this Article, we report the results of two phase 3,
available for patients who could not achieve controlled 52-week studies (Triple in Asthma With Uncontrolled
asthma with such combinations. Patients on Medium Strength of ICS + LABA [TRIMARAN]
The addition of the long-acting muscarinic antagonist and Triple in Asthma High Strength Versus ICS/LABA
tiotropium to inhaled corticosteroid plus long-acting HS and Tiotropium [TRIGGER]) comparing the efficacy
β2-agonist therapy has been shown to improve lung and safety of medium-strength (TRIMARAN) and high-
function and, in longer studies (48-week duration), strength (TRIGGER) BDP/FF/G with that of the medium-
reduce the risk of exacerbations in patients with asthma, strength (TRIMARAN) and high-strength (TRIGGER)
although in a subgroup of patients with persistent beclometasone dipropionate plus formoterol fumarate
airflow limitation.3–5 However, the addition of tiotro (BDP/FF) in patients with asthma that is poorly controlled
pium requires patients to use two different inhalers on medium-dose (TRIMARAN) or high-dose (TRIGGER)
of different design with different instructions for use, inhaled corticosteroid plus long-acting β2 agonist therapy.
and often with different dosing regimens. Such a These are the first studies to assess single-inhaler triple
combination is not only inconvenient for patients and therapy in a broad asthma population not restricted to
health-care providers who instruct on correct inhaler those with persistent airflow limitation.
use, but can negatively affect treatment adherence
and persistence.6–9 A single-inhaler triple therapy Methods
consisting of an extrafine formulation (ie, with mass Study design and participants
median aerodynamic diameter <2 µm) of the inhaled TRIMARAN and TRIGGER were both randomised, paral
corticosteroid beclometasone dipropionate, the long- lel-group, double-blind, active-controlled phase 3 studies.
acting β2 agonist formoterol fumarate, and the long- The main difference between the studies was the inhaled
acting muscarinic antagonist glycopyrronium (known corticosteroid dose received before and during the study,
as BDP/FF/G from hereon) delivered via a pressurised with patients in TRIMARAN receiving a medium dose
metered-dose inhaler is in development for patients and patients in TRIGGER receiving a high dose.
with asthma. Such extrafine formulations result in Patients were recruited for TRIMARAN from 171 sites
improved deposition in the small airways,10 which is across 16 countries, and for TRIGGER patients were
potentially important given that patients with asthma recruited from 221 sites across 17 countries (countries
See Online for appendix with substantial dysfunction of the small airways tend listed in the appendix [p 2]). The sites were a mixture of
to have worse asthma control and quality of life and are secondary and tertiary care centres and specialised inves
at increased exacerbation risk.11 tigation units, and 126 sites participated in both studies.
2 www.thelancet.com Published online September 30, 2019 https://doi.org/10.1016/S0140-6736(19)32215-9
Articles
Patients were eligible if they were aged 18–75 years, technology provider, stratified by country. Patients,
with a documented history of asthma for at least 1 year investigators, site staff, and sponsor personnel were
before screening and that was diagnosed before age masked to BDP/FF/G and BDP/FF assignment for the
40 years, prebronchodilator forced expiratory volume in duration of the studies, with all patients using pressurised
1 s (FEV1) of less than 80% predicted normal value, and a metered-dose inhalers. In TRIGGER, the BDP/FF plus
change in FEV1 of more than 12% and over 200 mL at tiotropium group was open-label.
10–15 min after inhaling salbutamol 400 µg. Further
inclusion criteria were uncon trolled asthma (Asthma Procedures
Control Questionnaire-7 [ACQ-7] ≥1·5); at least one Patients who met the eligibility criteria at screening had
exacerbation requiring treat ment with sys temic their asthma maintenance therapy switched to extrafine
corticosteroids or an emergency department visit or BDP/FF at 100 μg of BDP and 6 µg of FF in TRIMARAN
inpatient admission to hospital in the previous and 200 μg of BDP and 6 µg of FF in TRIGGER, at two
12 months; and that the patient was receiving a stable inhalations twice daily via pressurised metered-dose
dose of an inhaled corticosteroid plus a long-acting inhaler for a 2-week open-label run-in period. At the end
β2 agonist for at least 4 weeks before study entry of the run-in period, patients were randomly assigned
(TRIMARAN medium dose and TRIGGER high dose of to treatment. In TRIMARAN, patients either continued
inhaled corticosteroid; dose equivalents are in the on BDP/FF at the same dose as the run-in period,
appendix [p 2]). Key exclusion criteria were a history of at two inhalations twice daily, or received extrafine
near fatal asthma or previous admission to an intensive BDP/FF/G at 100 μg of BDP, 6 μg of FF, and 10 µg of G,
care unit for asthma that might place the patient at risk; a two inhalations twice daily via pressurised metered-dose
severe exacerbation in the 4 weeks before study entry or inhaler. In TRIGGER, patients either continued on
during the run-in period; any other substantial lung BDP/FF at the same dose as the run-in period with
disease that could interfere with study assessments; two inhalations twice daily via a pressurised metered-
current smokers or former smokers with 10 or more dose inhaler; or received extrafine BDP/FF/G at 200 μg
pack-years of exposure or who stopped smoking 1 year or of BDP, 6 μg of FF, and 10 µg of G with two inhalations
less before screening; current treatment with monoclonal twice daily; or open-label BDP/FF at 200 μg of BDP
antibodies or other biological drugs; clinically significant and 6 µg of FF at two inhalations twice daily via a pres
cardiovascular conditions or laboratory abnormalities; or surised metered-dose inhaler plus tiotropium 2·5 µg
unstable concurrent disease that could affect efficacy or at two inhalations once daily via a soft mist inhaler
safety. Full inclusion and exclusion criteria and non- (Respimat, Boehringer Ingelheim, Ingelheim am Rhein,
permitted asthma medications are listed in the appendix Germany). Over the 52-week treatment period, patients
(pp 2–5). attended visits at weeks 4, 12, 26, 40, and 52. Salbutamol
The studies were approved by the ethics committee or via pressurised metered-dose inhaler was permitted as
institutional review board at each site and were under rescue medication, but not within 6 h before any visit.
taken in accordance with the Declaration of Helsinki At each visit during the treatment period, data were
and the International Conference on Harmonization collected for spirometry (predose and 15 min, 30 min,
Good Clinical Practice (ICH/CPMP/135/95). There 1 h, 2 h, and 3 h after dose, with centralised spirometry)
were no substantial protocol amendments that affected and ACQ-7. Asthma exacerbations were captured
any patients who were randomly assigned to treatment. throughout the study. Each day, before treatment in the
The two protocols had one substantial amendment to morning and evening, patients recorded their peak
the inclusion criteria: to clarify that any long-acting expiratory flow (PEF), asthma symptoms (on a scale of 0
β2 agonist was permitted as previous medication, to 3, where 0 was no symptoms), and study treatment
providing it was taken at an approved daily dose that and rescue medication use in an electronic diary.
was clinically comparable to formoterol 24 μg, Treatment-emergent adverse events (defined as events
salmeterol 100 μg, or vilanterol 25 μg. All patients starting on or after first intake of randomly assigned
provided written informed consent before any study- study medication) were captured by the investigators
related procedures. throughout the study, along with severity and association
with study medication.
Randomisation and masking
After a run-in period of treatment with BDP/FF, Outcomes
eligible patients were randomly assigned to treatment. The coprimary endpoints for both studies were morning
In TRIMARAN, patients were randomly assigned (1:1) predose FEV1 at week 26 and the rate of moderate and
to either BDP/FF or extrafine BDP/FF/G. In TRIGGER, severe exacerbations over 52 weeks in each study. The key
patients were randomly assigned (2:2:1) to BDP/FF, secondary objectives were change from baseline in peak
extrafine BDP/FF/G, or open-label BDP/FF plus tio FEV1 at week 26 and average morning PEF over the first
tropium. Randomisation was done according to a ran 26 weeks in each study, and the rate of severe exac
domisation list generated by the interactive response erbations using data pooled from the two studies.
www.thelancet.com Published online September 30, 2019 https://doi.org/10.1016/S0140-6736(19)32215-9 3
Articles
Other secondary endpoints were change from baseline an approximate 13% drop-out rate at week 12, 16·5% at
in peak and predose FEV1 at all other visits; FEV1 area week 26, and 20% at week 52. Considering a two-sided
under the curve from 0 to 3 h after dose (AUC0–3h) at all significance level of 0·05, these numbers of patients
clinical visits; FEV1 response (change from baseline in would result in an approximately 99% power to detect a
predose FEV1 ≥100 mL) at weeks 26 and 52; change from mean difference of 90 mL in favour of BDP/FF/G over
baseline in ACQ-7 at all visits and ACQ-7 response BDP/FF in change from baseline in predose FEV1
(decrease from baseline score of at least 0·5 units) at at week 26, assuming an SD of 311 mL; approximately
weeks 26 and 52; change from baseline in average 93% power to detect a rate ratio (RR) of 0·80 between
morning and evening PEF over each between-visit BDP/FF/G and BDP/FF using a negative binomial model
period and over 52 weeks, and average evening PEF over and assuming an annualised rate of 2·70 moderate and
the first 26 weeks of treatment; time to first moderate severe exacerbations per patient in the BDP/FF group and
exacerbation and first moderate or severe exacerbation; an overdispersion parameter of the negative binomial
rate of moderate exacerbations; and rescue medication distribution of 0·56; approximately 99% power to detect a
use, days without rescue medication, daily asthma mean difference of 100 mL in favour of BDP/FF/G over
symptoms, asthma symptom-free days, and asthma BDP/FF in peak FEV1 change from baseline at week 26,
control days (ie, days with a total asthma symptoms score assuming an SD of 338 mL; at least 99% power to detect a
of 0 and no rescue medication use) over each between- mean difference of 20 L/min in favour of BDP/FF/G over
visit period and over the first 26 weeks and 52 weeks of BDP/FF in morning PEF change from baseline over the
treatment. Data were pooled from the two studies to 26-week treatment period, assuming an SD of 45 L/min;
compare BDP/FF/G with BDP/FF for the time to first and approximately 86% power to detect an RR of 0·80
moderate, severe, and moderate or severe exacerbation, between BDP/FF/G and BDP/FF in the pooled analysis,
and the rate of moderate exacerbations and combined using a negative binomial model and assuming an
moderate and severe exacerbations. Severe exacerbations annualised rate of 0·60 severe exacerbations per patient in
were pre specified to be analysed only in the pooled the BDP/FF group and an overdispersion parameter of the
population because we anticipated that the occurrence of negative binomial distribution of 0·56.
these events would be relatively low. To account for multiplicity, we did the comparisons
A severe asthma exacerbation was defined as worsening between BDP/FF/G and BDP/FF in terms of coprimary
of asthma that required treatment with systemic and key secondary efficacy endpoints according to the
corticosteroids for at least 3 days (with any associated following prespecified hierarchical testing procedure:
emergency department visit or admission to hospital (1) predose FEV1 at week 26, and rate of moderate and
documented). Moderate exacerbations were defined in severe exacerbations over 52 weeks; (2) peak FEV1 at
accordance with the American Thoracic Society and week 26; (3) average morning PEF over the first 26 weeks
European Respiratory Society joint statement12 as of treatment; and (4) rate of severe exacerbations over
meeting one or more of the following criteria: nocturnal 52 weeks in the pooled analysis.
awakenings due to asthma requiring a short-acting As a first step, we had to show superiority of BDP/FF/G
β2 agonist for 2 consecutive nights or an increase of 0·75 over BDP/FF for both coprimary endpoints. Thereafter,
or more from baseline in daily symptom score on we could only make confirmatory claims when
2 consecutive days; increase from baseline in use of superiority had been shown in all preceding steps. We
short-acting β2 agonist on 2 consecutive days (minimum did not apply multiplicity adjustments to the other
increase 4 puffs per day); 20% or more decrease in PEF secondary endpoints, and so these p values are
from baseline on at least 2 consecutive mornings or descriptive, as are the comparisons between BDP/FF/G
evenings, or 20% or more decrease in FEV1 from baseline; and BDP/FF plus tiotropium.
or a visit to an emergency department or a study site for We analysed predose and peak FEV1 at week 26 and
asthma treatment not requiring systemic corticosteroids. average morning PEF over 26 weeks using a linear mixed
Safety was assessed throughout the study. Major adverse model for repeated measures including treatment, visit,
cardiovascular events were adjudicated by an independent treatment by visit interaction, and country as fixed
committee, comprising three cardiologists. effects, and baseline value and baseline by visit inter
action as covariates (visit effect being replaced by
Statistical analysis between-visit period effect for PEF), and present these
To show superiority of BDP/FF/G over BDP/FF in terms data as adjusted means (ie, least squares means) and
of the coprimary and key secondary endpoints in both adjusted mean differences between treatments, with
studies, 574 patients needed to be randomly assigned to associated 95% CIs and p values. We assumed an
each treatment group. Since patients were randomly unstructured covariance matrix. We analysed the number
assigned in a ratio of 2:2:1 in TRIGGER, 287 patients were of asthma exacerbations over the 52-week treatment
needed for the BDP/FF plus tiotropium group. As such, a period using a negative binomial model including
total of 1148 patients in TRIMARAN and 1435 in TRIGGER treatment, country, and number of exacerbations (1 or >1)
would be needed. Our sample size calculation assumed in the previous year as fixed effects, and log-time on
4 www.thelancet.com Published online September 30, 2019 https://doi.org/10.1016/S0140-6736(19)32215-9
Articles
A
1628 patients assessed for eligibility of TRIMARAN
473 excluded
389 did not meet eligibility criteria
58 withdrew consent
4 had adverse events during run-in period
4 had asthma exacerbations during run-in period
1 lost to follow-up during run-in period
17 other
1155 randomly assigned
579 allocated to the BDP/FF/G group 576 allocated to the BDP/FF group
576 received allocated intervention 574 received allocated intervention
3 did not receive allocated intervention (randomly assigned in error) 2 did not receive allocated intervention (randomly assigned in error)
34 discontinued 35 discontinued
22 withdrew consent 26 withdrew consent
4 protocol violation 5 had adverse events
2 lost to follow-up 2 protocol violation
3 died 2 lost to follow-up
1 had an asthma exacerbation
2 other
542 completed treatment 539 completed treatment
576 included in safety population 574 included in safety population
575 included in efficacy population* 574 included in efficacy population
B
2100 patients assessed for eligibility of TRIGGER
663 excluded
579 did not meet inclusion criteria
63 withdrew consent
4 had adverse events during run-in period
3 lost to follow-up during run-in period
1 had an asthma exacerbation during run-in period
13 other
1437 randomly assigned
Figure 1: Study profile for
TRIMARAN (A) and
TRIGGER (B)
573 allocated to the BDP/FF/G group 576 allocated to the BDP/FF group 288 allocated to the BDP/FF plus tiotropium group BDP=beclometasone
571 received allocated intervention 573 received allocated intervention 287 received allocated intervention
dipropionate. FF=formoterol
2 did not receive allocated intervention 3 did not receive allocated intervention 1 did not receive allocated intervention
(randomly assigned in error) (randomly assigned in error) (randomly assigned in error) fumarate. G=glycopyrronium.
TRIGGER=Triple in Asthma
High Strength Versus
37 discontinued 40 discontinued 25 discontinued
ICS/LABA HS and Tiotropium.
26 withdrew consent 25 withdrew consent 20 withdrew consent TRIMARAN=Triple in Asthma
3 had adverse events 7 had adverse events 2 had adverse events With Uncontrolled Patients on
2 lack of efficacy 5 protocol violation 1 lost to follow up Medium Strength of
1 died 1 died 2 other ICS + LABA study. *One patient
1 protocol violation 1 lost to follow up in TRIMARAN and
4 other 1 other two patients in TRIGGER were
randomly assigned in error
(did not meet inclusion
534 completed treatment 533 completed treatment 262 completed treatment criteria), and received the first
dose of study medication
before being discontinued
571 included in safety population 573 included in safety population 287 included in safety population from the study without
571 included in efficacy population 571 included in efficacy population* 287 included in efficacy population providing any efficacy data
after the baseline assessment.
www.thelancet.com Published online September 30, 2019 https://doi.org/10.1016/S0140-6736(19)32215-9 5
Articles
study as offset, and present these data as adjusted rate of We analysed most of the secondary efficacy endpoints
asthma exacerbations, and adjusted RRs with 95% CIs using similar methods to the coprimary and key second
and p values. ary endpoints. We compared FEV1 response and ACQ-7
TRIMARAN TRIGGER
BDP/FF/G group BDP/FF group BDP/FF/G group BDP/FF group BDP/FF plus tiotropium
(n=576) (n=574) (n=571) (n=573) group (n=287)
Sex
Male 221 (38%) 221 (39%) 212 (37%) 245 (43%) 103 (36%)
Female 355 (62%) 353 (61%) 359 (63%) 328 (57%) 184 (64%)
Race
Asian 0 0 2 (<1%) 0 0
White 575 (100%) 574 (100%) 569 (>99%) 573 (100%) 286 (>99%)
Other 1 (<1%) 0 0 0 1 (<1%)
Age, years 52·6 (12·4) 52·5 (12·2) 53·1 (12·2) 54·0 (11·9) 51·6 (12·3)
Body-mass index, kg/m² 28·0 (4·81) 27·9 (5·07) 28·4 (5·14) 28·7 (5·87) 28·5 (5·21)
≥30 173 (30%) 170 (30%) 204 (36%) 205 (36%) 102 (36%)
Smoking status
Former smoker 92 (16%) 76 (13%) 83 (15%) 80 (14%) 42 (15%)
Non-smoker 484 (84%) 498 (87%) 488 (85%) 493 (86%) 245 (85%)
Smoking history (pack-years)* 4·1 (2·4) 4·8 (2·5) 4·9 (2·4) 4·8 (2·3) 5·6 (2·6)
Duration of asthma, years 24·8 (12·9) 25·2 (12·8) 24·8 (12·2) 26·2 (12·6) 24·5 (12·4)
Exacerbations in the previous year
1 474 (82%) 473 (82%) 439 (77%) 452 (79%) 229 (80%)
>1 102 (18%) 101 (18%) 132 (23%) 121 (21%) 58 (20%)
Before-salbutamol FEV1, L† 1·7 (0·56) 1·7 (0·56) 1·6 (0·56) 1·6 (0·57) 1·6 (0·59)
Before-salbutamol FEV1, % of 55·2 (12·3) 55·7 (12·0) 51·9 (13·5) 51·8 (13·5) 52·1 (13·2)
predicted normal value†
Range 17–79 20–79 15–79 16–79 22–79
Reversibility, % 32·5 (24·72) 30·8 (20·53) 33·2 (20·21) 33·9 (21·87) 34·9 (26·99)
Range 12·1–419·2 12·1–163·0 12·1–147·9 12·0–152·5 12·2–234·5
Before-salbutamol FEV1/FVC ratio† 0·60 (0·12) 0·61 (0·12) 0·59 (0·12) 0·59 (0·13) 0·59 (0·12)
Range 0·26–0·96 0·27–0·94 0·23–0·95 0·27–0·94 0·29–0·88
After-salbutamol FEV1/FVC ratio‡ 0·65 (0·11) 0·65 (0·11) 0·63 (0·12)§ 0·63 (0·12) 0·63 (0·12)
Range 0·31–0·97 0·32–0·91 0·27–0·93 0·26–0·92 0·34–0·96
Previous inhaled corticosteroid or long-acting β2-agonist therapy¶
Inhaled corticosteroid 61 (11%) 72 (13%) 153 (27%) 144 (25%) 67 (23%)
Inhaled corticosteroid plus 531 (92%) 515 (90%) 525 (92%) 520 (91%) 267 (93%)
long-acting β2 agonist
Long-acting β2 agonist 55 (10%) 66 (11%) 74 (13%) 71 (12%) 35 (12%)
ACQ-7 score|| 2·3 (0·52) 2·3 (0·53) 2·5 (0·53)§ 2·4 (0·54)** 2·4 (0·53)
Peak expiratory flow, L/min††
Morning 297 (107·5)‡‡ 299 (106·0)‡‡ 279 (104·2)§§ 275 (101·2)¶¶ 287 (106·4)
Evening 310 (108·2)|||| 314 (107·6)‡‡ 292 (104·7)¶¶ 287 (103·1)|||| 299 (107·6)
Daily asthma symptom scores†† 0·76 (0·49) 0·77 (0·50) 0·81 (0·52) 0·83 (0·51) 0·84 (0·50)
Percentage of asthma symptom-free 9·9% (22·78) 11·0% (24·19) 10·2% (23·09) 9·5% (23·14) 10·8% (26·58)
days††
Percentage of asthma control days†† 9·1% (21·45) 10·4% (23·48) 9·9% (22·66) 8·9% (22·24) 10·1% (26·22)
Data are n (%), mean (SD), or range. TRIMARAN=Triple in Asthma With Uncontrolled Patients on Medium Strength of ICS + LABA study. TRIGGER=Triple in Asthma High
Strength Versus ICS/LABA HS and Tiotropium study. BDP=beclometasone dipropionate. FF=formoterol fumarate. G=glycopyrronium. FEV1=forced expiratory volume in 1 s.
FVC=forced vital capacity. ACQ-7=Asthma Control Questionnaire-7. *Calculated in former smokers only. †Measured at screening before administration of salbutamol. ‡Measured
at screening 10–15 min after administration of salbutamol. §Data available for 570 patients. ¶Calculated from asthma therapies being given before study entry (might add up to
more than 100% because of changes in asthma therapy in the 3 months before study or multiple therapies reported for the same patient). ||Measured at the randomisation visit
in the intention-to-treat population. **Data available for 568 patients. ††Measured during the run-in period in the intention-to-treat population; the intention-to-treat
populations were TRIMARAN n=575 in the BDP/FF/G group, n=574 in the BDP/FF group; TRIGGER n=571 in the BDP/FF/G group, n=571 in the BDP/FF group, and n=287 in the
BDP/FF plus tiotropium group. ‡‡Data available for 569 patients. §§Data available for 564 patients. ¶¶Data available for 565 patients. ||||Data available for 566 patients.
Table 1: Baseline characteristics of the safety population
6 www.thelancet.com Published online September 30, 2019 https://doi.org/10.1016/S0140-6736(19)32215-9
Articles
response between treatment groups using a logistic tiotropium group completed treatment (figure 1B).
model including treatment and country as factors and Baseline demographic charac teristics were similar
the respective baseline values for these measures as a across the five groups (table 1). Patients in TRIGGER
covariate. We analysed time to first exacerbation using a had a slightly worse lung function (as measured by
Cox proportional hazards model including treatment, before-salbutamol FEV1) and higher reversibility than
country, and number of exacerbations (1 or >1) in the those in TRIMARAN.
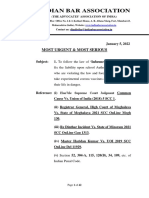
previous year as factors. Estimation of the logistic and The coprimary endpoint of change in predose FEV1 at
Cox proportional hazards models was based on events week 26 was met in both studies, with significant dif
per variable values well above the suggested thresholds, ferences between the BDP/FF/G and BDP/FF groups of
confirming the reliability of the study results.13–15 All 57 mL (95% CI 15 to 99; p=0·0080) in TRIMARAN and
analyses reported in this Article were prespecified in the 73 mL (26 to 120; p=0·0025) in TRIGGER (figure 2A;
statistical analysis plan.
Additionally, we did a number needed to treat analysis A
for the number of patients who would need to be treated Adjusted mean difference* 57 mL Adjusted mean difference* 73 mL
with BDP/FF/G rather than BDP/FF for 1 year to prevent (15 to 99); p=0·0080 (26 to 120); p=0·0025
one moderate or severe exacerbation, one moderate Adjusted mean difference –45 mL
exacerbation, or one severe exacerbation. 350 (–103 to 13); p=0·13
We analysed all efficacy endpoints in the intention- 274 mL
to-treat population, defined as all patients randomly 300 229 mL (227 to 321)
Predose FEV1 change from baseline, mL
(196 to 263)
assigned to treatment who received at least one dose of
250 185 mL
the study treatment and with at least one available (155 to 214) 157 mL
evaluation of efficacy (primary or secondary efficacy 200 (123 to 190)
127 mL
variables) after baseline. Safety data were analysed in (98 to 157)
the safety population, which comprised all patients 150
randomly assigned to treatment who received at least
one dose of study treatment. An independent Data 100
Safety Monitoring Board composed of three independent
50
clinicians and one independent biostatistician provided
a quarterly independent scrutiny of the study. 0
We did all analyses presented in this manuscript using
SAS software, version 9.4. The studies are registered with B
Adjusted rate ratio* 0·85 Adjusted rate ratio* 0·88
ClinicalTrials.gov: TRIMARAN, NCT02676076; TRIGGER, (0·73 to 0·99); p=0·033 (0·75 to 1·03); p=0·11
NCT02676089.
3·0 Adjusted rate ratio 1·07
Annualised rate of moderate and severe exacerbations
(0·88 to 1·30); p=0·50
Role of the funding source 2·16
2·5 (1·94 to 2·40) 1·96
The funder of the study had a role in the study design 1·83 (1·76 to 2·19)
1·73
and data analysis, oversaw study conduct, and was (1·63 to 2·04)
(1·54 to 1·93)
1·61
2·0 (1·37 to 1·90)
responsible for study report preparation. All authors
had full access to all data and the corresponding author
had final responsibility for the decision to submit for 1·5
publication.
1·0
Results
TRIMARAN was undertaken between Feb 17, 2016, and 0·5
May 17, 2018, during which time 1628 patients were
assessed for eligibility, of whom 1155 patients were 0
BDP/FF/G BDP/FF BDP/FF/G BDP/FF BDP/FF
randomly assigned to the BDP/FF/G group (n=579) or group group group group plus tiotropium
the BDP/FF group (n=576); 542 (94%) patients in the (n=575) (n=574) (n=571) (n=571) group (n=287)
BDP/FF/G group and 539 (94%) in the BDP/FF group TRIMARAN TRIGGER
completed treatment (figure 1A). TRIGGER was
Figure 2: Coprimary endpoints
undertaken between April 6, 2016, and May 28, 2018,
(A) Predose FEV1 change from baseline to week 26. (B) Annualised rate of moderate and severe exacerbations.
during which time 2100 patients were assessed for Results are from the intention-to-treat population. In panel A, data are adjusted means with 95% CIs shown as
eligibility, of whom 1437 were randomly assigned to the error bars and in parentheses, and adjusted mean differences with 95% CIs in parentheses. In panel B, data are
BDP/FF/G group (n=573), BDP/FF group (n=576), or adjusted exacerbation rates per patient per year with 95% CIs shown as error bars and in parentheses,
and adjusted rate ratios with 95% CIs in parentheses. BDP=beclometasone dipropionate. FEV1=forced expiratory
BDP/FF plus tiotropium group (n=288); 534 (93%)
volume in 1 s. FF=formoterol fumarate. G=glycopyrronium. TRIGGER=Triple in Asthma High Strength Versus
patients in the BDP/FF/G group, 533 (93%) in the ICS/LABA HS and Tiotropium study. TRIMARAN=Triple in Asthma With Uncontrolled Patients on Medium
BDP/FF group, and 262 (91%) in the BDP/FF plus Strength of ICS + LABA study. *Coprimary endpoints.
www.thelancet.com Published online September 30, 2019 https://doi.org/10.1016/S0140-6736(19)32215-9 7
Articles
absolute values are in the appendix [pp 19–20]). In
A TRIGGER, the predose FEV1 at week 26 was not different
Adjusted mean difference* 84 mL Adjusted mean difference* 105 mL between the BDP/FF/G and the BDP/FF plus tiotropium
(40 to 129); p=0·0002 (57 to 153); p<0·0001
groups (–45 mL, –103 to 13; p=0·13). The rate of moderate
Adjusted mean difference –33 mL and severe exacerbations in the BDP/FF/G group was
700 (–92 to 26); p=0·27
significantly reduced by 15% compared with the BDP/FF
522 mL 555 mL group in TRIMARAN (RR 0·85, 95% CI 0·73–0·99;
600 485 mL (488 to 556) (507 to 603)
p=0·033; figure 2B; appendix pp 19–20). The reduction in
Peak FEV1 change from baseline, mL
(453 to 516) 417 mL
500 401 mL (383 to 451) TRIGGER was 12% but was not significant (0·88, 95% CI
(369 to 432) 0·75–1·03; p=0·11). No difference was seen between the
400 BDP/FF/G group and BDP/FF plus tiotropium group in
TRIGGER (1·07, 0·88–1·30; p=0·50). Since this coprimary
300
endpoint was not significantly reduced in TRIGGER, in
200
accordance with the prespecified hierarchical testing
procedure, no formal claim of superiority can be made,
100 either in this study or for the key secondary endpoint of
rate of severe exacerbations (pooled analysis). Therefore,
0 the corresponding p values should be interpreted
descriptively.
B
Adjusted mean difference* 8·5 L/min Adjusted mean difference* 7·8 L/min For the key secondary endpoints of peak FEV1 at week 26
(3·6 to 13·3); p=0·0006 (3·0 to 12·6); p=0·0014
and average morning PEF over 26 weeks, the change
Adjusted mean difference –0·2 L/min from baseline was higher in the BDP/FF/G group than in
(–6·0 to 5·6); p=0·95 the BDP/FF group in both studies (p=0·0002 for peak
20
10·3 L/min FEV1 and p=0·0006 for morning PEF in TRIMARAN, and
Morning PEF change from baseline, L/min
10·1 L/min (5·5 to 15·0)
15 (6·7 to 13·5)
p<0·0001 for peak FEV1 and p=0·0014 for morning PEF
5·3 L/min
in TRIGGER), with no differences between the BDP/FF/G
10
(1·9 to 8·7) group and the BDP/FF plus tiotropium group in
2·3 L/min TRIGGER (p=0·27 for peak FEV1 and p=0·95 for morning
(–1·1 to 5·7)
5 –3·1 L/min
PEF; figure 3A and 3B; absolute values are in the appendix
(–6·5 to 0·3) [pp 19–20]). In the pooled analysis, patients in the
BDP/FF/G groups had a reduced rate of severe exacer
0
bations compared with those in the BDP/FF groups (23%;
p=0·0076; figure 3C; appendix pp 19–20).
–5
For the other secondary end points, patients in the
BDP/FF/G group had a reduced rate of moderate
–10
BDP/FF/G BDP/FF BDP/FF/G BDP/FF BDP/FF exacerbations (12%; p=0·043), and combined moderate
group group group group plus tiotropium and severe exacerbations (14%; p=0·0083) compared with
(n=575) (n=574) (n=571) (n=571) group (n=287)
those in the BDP/FF group (pooled analysis, figure 3C;
TRIMARAN TRIGGER appendix pp 19–20). In the individual studies, the same
trend for the reduced rate of exacerbations in the
C
Rate ratio* 0·77 Rate ratio 0·88 Rate ratio 0·86 BDP/FF/G group was observed for moderate exacer
(0·64 to 0·93); p=0·0076 (0·78 to 1·00); p=0·043 (0·77 to 0·96); p=0·0083
bations (p=0·086 in TRIMARAN and p=0·25 in
2·5
BDP/FF/G pooled (n=1146)
2·07 TRIGGER; appendix p 6).
(1·92 to 2·24)
BDP/FF pooled (n=1145) 1·79
1·72 (1·65 to 1·94)
2·0 (1·58 to 1·87)
1·52
Annualised rate of exacerbations
(1·39 to 1·65) Figure 3: Key secondary endpoints
1·5 (A) Peak FEV1 change from baseline at week 26. (B) Average morning PEF
change from baseline over 26 weeks. (C) Annualised rate of severe, moderate,
and moderate and severe exacerbations (pooled analysis). Results are from
1·0
the intention-to-treat population. Data in panels A and B are adjusted means
with 95% CI shown as error bars and in parentheses, and adjusted mean
differences with 95% CIs in parentheses. Data in panel C are adjusted annualised
0·31
0·24 (0·27 to 0·35) rate of exacerbations per patient, with 95% CIs as error bars and in parentheses,
0·5
(0·21 to 0·28) and adjusted rate ratios with 95% CIs in parentheses. BDP=beclometasone
dipropionate. FEV1=forced expiratory volume in 1 s. FF=formoterol fumarate.
G=glycopyrronium. PEF=peak expiratory flow. TRIGGER=Triple in Asthma High
0
Strength Versus ICS/LABA HS and Tiotropium study. TRIMARAN=Triple in Asthma
Severe exacerbations Moderate exacerbations Moderate and severe
exacerbations
With Uncontrolled Patients on Medium Strength of ICS + LABA study.
*Key secondary endpoints.
8 www.thelancet.com Published online September 30, 2019 https://doi.org/10.1016/S0140-6736(19)32215-9
Articles
The time to first moderate or severe exacerbation was or moderate in severity, and few were considered to be
longer in the BDP/FF/G group than in the BDP/FF group related to treatment. The most common adverse event in
in both TRIMARAN (hazard ratio [HR] 0·84, 95% CI all groups was asthma exacerbation, the occurrence of
0·73–0·98; p=0·022; figure 4A) and TRIGGER (0·80, which was lower with triple therapy than with BDP/FF in
0·69–0·93; p=0·0035), and was similar for the BDP/FF/G both studies. Four patients had treatment-related serious
and BDP/FF plus tiotropium groups in TRIGGER (0·97, adverse events: atrial fibrillation in a patient given
0·81–1·18; p=0·78; figure 4B). Likewise, the time to first
moderate exacerbation was longer in the BDP/FF/G
group than in the BDP/FF group in both studies A
100 BDP/FF/G group
(TRIMARAN HR 0·86, 95% CI 0·73–1·0; p=0·048; BDP/FF group
Probability of a moderate or severe
TRIGGER 0·81, 0·69–0·95; p=0·0089) and was similar
80
for the BDP/FF/G group and BDP/FF plus tiotropium
exacerbation (%)
group in TRIGGER (0·89, 0·73–1·09; p=0·27). In the 60
pooled analysis, time to first moderate or severe
exacerbation was longer in the BDP/FF/G group than 40
in the BDP/FF group (HR 0·82, 95% CI 0·74–0·91;
20
p=0·0002), as was time to first moderate exacerbation HR 0·84 (95% CI 0·73–0·98);
(0·83, 0·74–0·93; p=0·0010), and time to first severe p=0·022
0
exacerbation (0·79, 0·66–0·95; p=0·011; figure 4C). 0 4 12 26 40 52
Number at risk
Median times to first exacerbation are in the appendix BDP/FF/G group 575 455 368 293 252 155
(p 21). In the pooled analyses, the numbers needed to BDP/FF group 574 457 354 257 199 121
treat for 1 year with BDP/FF/G rather than BDP/FF to
B
prevent one moderate or severe exacerbation was three,
100 BDP/FF/G group
to prevent one severe exacerbation was 14, and to prevent BDP/FF group
Probability of a moderate or severe
one moderate exacerbation was five. BDP/FF plus tiotropium group
80
The results for the FEV1 secondary endpoints in
exacerbation (%)
TRIMARAN were consistent with the coprimary and 60
key secondary FEV1 endpoints, with improvements seen
in the BDP/FF/G group compared with the BDP/FF 40
BDP/FF/G vs BDP/FF:
group in predose FEV1 at most visits, peak FEV1 and HR 0·80 (95% CI 0·69–0·93); p=0·0035
20
FEV1 AUC0–3h at all visits, and FEV1 response at week 26 BDP/FF/G vs BDP/FF plus tiotropium:
HR 0·97 (95% CI 0·81–1·18); p=0·78
(appendix pp 7–9, 22–26). In TRIGGER, improvements 0
were seen in the BDP/FF/G group for predose FEV1, Number at risk
0 4 12 26 40 52
peak FEV1, and FEV1 AUC0–3h at all visits, and FEV1 BDP/FF/G group 571 460 363 292 253 148
response at weeks 26 and 52 compared with the BDP/FF BDP/FF group 571 421 331 252 213 129
BDP/FF plus tiotropium 287 222 175 146 128 76
group, with no differences between the BDP/FF/G group
group and BDP/FF plus tiotropium group (appendix
pp 7–9, 22–26). C
100 BDP/FF/G pooled groups
All PEF-based secondary endpoints improved in the
Probability of a severe exacerbation (%)
BDP/FF pooled groups
BDP/FF/G group compared with the BDP/FF group in 80
both studies (appendix pp 10–12). We saw no clinically
relevant differences between the BDP/FF/G group and 60
the BDP/FF or BDP/FF plus tiotropium group in HR 0·79 (95% CI 0·66–0·95);
p=0·011
TRIGGER in terms of ACQ-7 total score or response 40
(appendix pp 13, 22–26), or in the rescue medication use
20
endpoints (appendix pp 14–15, 22–26). Notably, we saw
an improvement from baseline in asthma symptoms, 0
asthma control, and rescue medication use in all five 0 4 12 26 40 52
groups over the duration of the studies, with similar Time since randomisation (weeks)
Number at risk
improvements seen in TRIMARAN for both the BDP/FF/G pooled groups 1146 1109 1048 984 924 590
BDP/FF pooled groups 1145 1098 1031 942 871 544
BDP/FF/G and BDP/FF groups and an improvement
seen in TRIGGER for the BDP/FF/G group compared Figure 4: Time to first moderate or severe exacerbation in TRIMARAN (A) and
with the BDP/FF group in terms of asthma symptom- TRIGGER (B; intention-to-treat populations), and pooled analysis of time to
free days and asthma control days from week 13 onwards first severe exacerbation (C)
BDP=beclometasone dipropionate; FF=formoterol fumarate. G=glycopyrronium.
(appendix pp 16–18, 22–26).
HR=hazard ratio. TRIGGER=Triple in Asthma High Strength Versus ICS/LABA HS
Overall, a similar proportion of patients had adverse and Tiotropium study. TRIMARAN=Triple in Asthma With Uncontrolled Patients
events in all five groups (table 2). Most events were mild on Medium Strength of ICS + LABA study.
www.thelancet.com Published online September 30, 2019 https://doi.org/10.1016/S0140-6736(19)32215-9 9
Articles
and acute cardiac failure). In TRIGGER, two patients had
TRIMARAN TRIGGER
an adverse event leading to death, one in the BDP/FF/G
BDP/FF/G BDP/FF BDP/FF/G BDP/FF BDP/FF plus group (cerebral haemorrhage) and one in the BDP/FF
group group group group tiotropium
(n=576) (n=574) (n=571) (n=573) (n=287) group (sudden death). None of the deaths in either study
was considered as related to study treatment.
Adverse events 431 (75%) 455 (79%) 410 (72%) 443 (77%) 210 (73%)
Asthma exacerbation 337 (59%) 379 (66%) 323 (57%) 364 (64%) 162 (56%)
Discussion
Nasopharyngitis 71 (12%) 79 (14%) 46 (8%) 63 (11%) 34 (12%)
TRIMARAN and TRIGGER are the first studies to assess
Headache 38 (7%) 46 (8%) 25 (4%) 27 (5%) 13 (5%)
the efficacy and safety of single-inhaler triple therapy in
Respiratory tract infection viral 15 (3%) 26 (5%) 17 (3%) 28 (5%) 14 (5%)
the management of asthma. The lung function (predose
Bronchitis 18 (3%) 22 (4%) 18 (3%) 18 (3%) 12 (4%)
FEV1) coprimary endpoint was met in both studies,
Pharyngitis 12 (2%) 16 (3%) 10 (2%) 12 (2%) 4 (1%)
with a slightly larger effect size in TRIGGER.
Viral upper respiratory tract 12 (2%) 16 (3%) 4 (1%) 8 (1%) 3 (1%) Furthermore, the rate of moderate and severe exacer
infection
bations coprimary endpoint was met in TRIMARAN,
Hypertension 16 (3%) 9 (2%) 10 (2%) 7 (1%) 7 (2%)
with a significant 15% reduction for BDP/FF/G versus
Upper respiratory tract infection 11 (2%) 10 (2%) 9 (2%) 15 (3%) 7 (2%)
BDP/FF, and although a similar effect size was seen in
Treatment-related adverse events 22 (4%) 19 (3%) 28 (5%) 24 (4%) 16 (6%)
TRIGGER, with a 12% reduction, it was not significant.
Dysphonia 9 (2%) 1 (<1%) 10 (2%) 8 (1%) 2 (1%)
In the key secondary endpoint analysis of data pooled
Cough 1 (<1%) 0 0 1 (<1%) 2 (1%)
from the two studies, BDP/FF/G reduced the rate of
Oral candidiasis 1 (<1%) 4 (1%) 3 (1%) 3 (1%) 3 (1%)
the more clinically relevant severe exacerbations by
Dry mouth 4 (1%) 0 3 (1%) 1 (<1%) 2 (1%)
23%. Furthermore, for the other secondary exacerbation
Electrocardiogram QT prolonged 1 (<1%) 3 (1%) 1 (<1%) 1 (<1%) 0
endpoints, in the pooled analyses, BDP/FF/G reduced
Muscle spasms 0 0 3 (1%) 3 (1%) 0 the rate of moderate exacerbations by 12% and combined
Serious adverse events 28 (5%) 22 (4%) 28 (5%) 33 (6%) 15 (5%) moderate and severe exacerbations by 14% and the time
Asthma exacerbation 7 (1%) 4 (1%) 11 (2%) 11 (2%) 6 (2%) to first moderate or severe exacerbation, first moderate
Pneumonia 0 3 (1%) 3 (1%) 5 (1%) 2 (1%) exacerbation, and first severe exacerbation was longer
Treatment-related serious adverse 1 (<1%) 0 1 (<1%) 2 (<1%) 0 with BDP/FF/G than with BDP/FF. Overall, these exacer
events
bation data therefore suggest that BDP/FF/G prevents
Severe adverse events 34 (6%) 38 (7%) 35 (6%) 55 (10%) 13 (5%)
these events to a greater degree than BDP/FF.
Major adverse cardiovascular 4 (1%) 1 (<1%) 3 (1%) 3 (1%) 0
events
Although care should be taken when comparing
studies, the 23% reduction in the rate of severe
Adverse events leading to study 4 (1%) 5 (1%) 4 (1%) 8 (1%) 2 (1%)
treatment discontinuation exacerbations along with the 21% reduction in risk (time
Adverse events leading to death 3 (1%) 0 1 (<1%) 1 (<1%) 0 to first severe exacerbation HR 0·79) are consistent
with the results of two long-term studies3 in which
Data are n (%). Preferred terms are listed when occurrence was 2·5% or higher in any treatment group for adverse events
and when occurrence was 0·5% or higher in any group for serious adverse events and treatment-related adverse events. tiotropium was added as a free combination to any
TRIMARAN=Triple in Asthma With Uncontrolled Patients on Medium Strength of ICS + LABA study. TRIGGER=Triple in inhaled corticosteroid and long-acting β2 agonist (with a
Asthma High Strength Versus ICS/LABA HS and Tiotropium study. BDP=beclometasone dipropionate. FF=formoterol 20% rate reduction and a 21% risk reduction for
fumarate. G=glycopyrronium.
tiotropium vs placebo on severe exacerbations).3 Impor
Table 2: Treatment-emergent adverse events and serious adverse events in the safety population tantly, however, TRIMARAN and TRIGGER had less
strict exclusion criteria than these studies and so enrolled
broader patient populations. Specifically, the tiotropium
BDP/FF/G in TRIMARAN and who had hypertension; studies were limited to a subgroup of patients with post-
oesophageal candidiasis in a patient given BDP/FF/G in bronchodilator FEV1 of 80% or less and FEV1 to forced
TRIGGER that resolved after therapy; pneumonia in a vital capacity (FVC) ratio of 70% or less,3 compared
patient given BDP/FF in TRIGGER that resolved after with pre-bronchodilator FEV1 of less than 80% in
therapy; and angle closure glaucoma in a patient given TRIMARAN and TRIGGER and no limitation on the
BDP/FF in TRIGGER that had not resolved by the time FEV1 to FVC ratio. Another key difference is that in
they completed the study. All these treatment-related the long-term tiotro pium studies triple therapy was
serious adverse events were moderate in severity and did administered via multiple inhalers and they did not
not require a change in study treatment. Five patients in supply or monitor the daily concomitant use of inhaled
TRIMARAN and six in TRIGGER had major adverse corticosteroids or long-acting β2 agonists.3 The use of
cardiovascular events, although none of the events in single-inhaler triple therapy in TRIMARAN and
either study were considered as related to study treatment TRIGGER ensured the delivery of all three components
(table 2; appendix p 27). Three patients in the BDP/FF/G and should poten tially optimise treatment adherence
group in TRIMARAN had an adverse event or events and persistence. However, we acknowledge that in
leading to death (one patient with left ventricular failure, TRIGGER for FEV1 and moderate-to-severe exacer
one with acute pancreatitis, and one with gastric cancer bations, patients in the BDP/FF plus tiotropium group
10 www.thelancet.com Published online September 30, 2019 https://doi.org/10.1016/S0140-6736(19)32215-9
Articles
(treatment administered open-label via separate inhalers) corticosteroids, emergency department visit, or inpatient
had non-significant, numerically greater improvements admission to hospital. In this context, the much lower
than those in the single inhaler (double-bind) BDP/FF/G rate of severe exacerbations observed during the studies
group. than reported in historical data (ie, the patient’s history
Most exacerbations in TRIMARAN and TRIGGER of at least one exacerbation in the previous year) is
were moderate in severity, and hence were predominantly similar to what has been found in several clinical trials
self-managed by patients. To our knowledge, this is the that recruited similar populations,16–20 potentially also
first study to assess the effect of inhaled therapy on reflecting increased adherence to therapy or improved
such exacerbations by applying the American Thoracic care as a result of clinical trial participation. Importantly,
Society and European Respiratory Society joint state when TRIMARAN and TRIGGER were designed, the
ment definition.12 Although we saw a consistent trend in rate of these more clinically relevant exacerbations
favour of triple therapy, we saw no significant treatment was antici pated to be lower than that of moderate
effect on the rate of moderate exacerbations in the exacerbations, which is why the only pre specified
individual studies, yet the time to first moderate analysis of rate of severe exacerbations was in the pooled
exacerbation was longer in the BDP/FF/G group than in population. Therefore, despite this low rate, a notable
the BDP/FF group, both in the pooled analysis and in 23% reduction in severe exacerbations was seen with
each individual study. The reasons for this finding are BDP/FF/G compared with BDP/FF.
unclear, although it might be due to the variability of Interpreting the clinical relevance of results when
symptoms in asthma (the worsening of which defines a assessing the additive effect of a therapy on top of
moderate exacerbation episode), so making precise therapies that are known to be effective is challenging.
assessment of this outcome is a challenge. Additionally, The differences that we observed between the BDP/FF/G
neither study was powered to assess the effect of treat group and BDP/FF group for some of the endpoints
ment on moderate exacerbations. The effect of triple could be argued to be numerically small (with the
therapy on the objective lung function endpoints of FEV1 differences in predose FEV1 at week 26 and morning PEF
and PEF was consistent, within and between studies, over 26 weeks being lower than those included in the
with both BDP/FF/G doses improving these endpoints powering assumptions), and indicate only a moderate
compared with BDP/FF for the duration of the studies. effect of triple therapy. However, the populations that we
Asthma control, symptom endpoints, and rescue studied have few treatment options available, and so even
medication use improved from baseline with all treat moderate incremental improvements can be valuable.
ments. In TRIMARAN, both the BDP/FF/G and BDP/FF Uncontrolled asthma is associated with a substantial
groups had similar improvements in symptom-free days (and increasing) economic and health burden,21 especially
and asthma control days, whereas in TRIGGER we saw a because of exacerbations, and so additional therapies are
separation between the BDP/FF/G and BDP/FF groups, needed. In this context, a key finding is that all treat
particularly over the second half of the study. These ments were similarly well tolerated. This finding is again
results are similar to those of the previous tiotropium consistent with the results of several other triple therapy
studies, in which tiotropium administered separately to studies in asthma, in which the addition of a long-acting
an inhaled corticosteroid plus a long-acting β2 agonist muscarinic antagonist did not affect the overall adverse
resulted in consistent improvements in lung function, event profile.3–5,22
but less consistent improvements in ACQ-7 score,3,4 and Given the broad inclusion criteria of TRIMARAN
with a dissociation in effect between severe exacer and TRIGGER, the results should be generalisable to
bations and asthma control.3 For the populations that adults with asthma that is uncontrolled by an inhaled
we recruited (who had uncontrolled disease despite corticosteroid plus a long-acting β2 agonist, although
medium-dose or high-dose inhaled corticosteroid plus a we recognise that the recruited populations were
long-acting β2 agonist), the prevention of future exacer predominantly of white race. The Global Initiative for
bations (especially severe exacerbations) is arguably the Asthma report already includes recommendations
more important treatment goal. for add-on long-acting muscarinic antagonist use for
We acknowledge that the improvement in asthma con patients whose asthma is not well controlled on inhaled
trol and decrease in symptoms in all groups, including in corticosteroid plus long-acting β2-agonist therapy.1 For
those patients who continued BDP/FF therapy from the such patients, escalation of therapy to inhaled triple
run-in period across the 52-week trial period, suggests a therapy has been shown to be cost-effective compared with
clinical trial effect in both studies, which can occur at an inhaled corticosteroid plus a long-acting β2 agonist,23–27
least in part because of improved adherence. This clinical and is likely to be cost-effective compared with the addition
trial effect also appeared to affect severe exacerbations, of systemic biological therapy.25 Since BDP/FF/G delivers
with a low rate observed during the trial (0·31 in the the three molecules via one device, and based on the
pooled BDP/FF group), despite all patients being magnitude of reduction in the annual rate of severe asthma
required to have a history of at least one exacerbation in exacerbations observed in the prespecified pooled analysis
the previous year requiring treatment with systemic of TRIMARAN and TRIGGER, we expect that BDP/FF/G
www.thelancet.com Published online September 30, 2019 https://doi.org/10.1016/S0140-6736(19)32215-9 11
Articles
will provide an attractive treatment option and fulfil a Medicines Agency or the US Food and Drug Administration, or both,
substantial unmet need at both the individual-patient and after Jan 1, 2015, following the approval of any received research proposal
and the signature of a Data Sharing Agreement. Chiesi Farmaceutici
the overall health system level. provides access to clinical trial information consistently with the principle
Taken together, these data indicate that in adults with of safeguarding commercially confidential information and patient
uncontrolled asthma treated with a medium-to-high dose privacy. Other information on Chiesi’s data sharing commitment, access,
of inhaled corticosteroid plus a long-acting β2 agonist the and research request approval process are available in the Clinical Trial
Transparency section at http://www.chiesi.com/en/research-and-
addition of a long-acting muscarinic antagonist in a development/.
single inhaler BDP/FF/G triple therapy mainly improves
Acknowledgments
lung function with an associated positive effect on severe DS is supported by the National Institute for Health Research
exacerbations and some benefit in terms of asthma Manchester Biomedical Research Centre. These studies were funded by
symptoms and control. Chiesi Farmaceutici. We thank the investigators and patients at the
investigative sites for their support. Writing support was provided by
Contributors David Young of Young Medical Communications and Consulting,
The studies were conceived and designed by JCV, AP, MK, SP, and GWC. funded by Chiesi Farmaceutici.
Data were acquired by JCV, PK, PP, and GWC, analysed by AV, and
interpreted by all authors. MK and GG contributed to the medical data References
integrity. SC and FZ contributed to the conduct of the studies. SC and FZ 1 Reddel HK, FitzGerald JM, Bateman ED, et al. GINA 2019:
were Chiesi Farmaceutici clinical operation project managers, AV was a a fundamental change in asthma management: treatment of
asthma with short-acting bronchodilators alone is no longer
Chiesi Farmaceutici statistician, SP was head of Chiesi Farmaceutici
recommended for adults and adolescents. Eur Respir J 2019;
global clinical development, and GG was the Clinical Program Leader for
53: 1901046.
BDP/FF/G. JCV was the principal investigator for TRIMARAN and GWC
2 Hirst C, Calingaert B, Stanford R, Castellsague J. Use of long-acting
was the principal investigator for TRIGGER. The manuscript was revised
β-agonists and inhaled steroids in asthma: meta-analysis of
for intellectual content and approved for publication by all authors. observational studies. J Asthma 2010; 47: 439–46.
Declaration of interests 3 Kerstjens HAM, Engel M, Dahl R, et al. Tiotropium in asthma
JCV reports personal fees from Chiesi Farmaceutici during the conduct poorly controlled with standard combination therapy. N Engl J Med
of the study. JCV has previously lectured and received honoraria from 2012; 367: 1198–207.
AstraZeneca, Avontec, Bayer, Bencard, Bionorica, Boehringer Ingelheim, 4 Ohta K, Ichinose M, Tohda Y, et al. Long-term once-daily tiotropium
Chiesi, Essex/Schering-Plough, GlaxoSmithKline, Janssen-Cilag, Leti, respimat is well tolerated and maintains efficacy over 52 weeks in
MEDA, Merck, MSD, Mundipharma, Novartis, Nycomed/Altana, Pfizer, patients with symptomatic asthma in Japan: a randomised,
placebo-controlled study. PLoS One 2015; 10: e0124109.
Revotar, Sanofi/Regeneron, Sandoz-Hexal, Stallergens, TEVA,
UCB/Schwarz-Pharma, and Zydus/Cadila; participated in advisory 5 Hoshino M, Ohtawa J, Akitsu K. Effects of the addition of tiotropium
on airway dimensions in symptomatic asthma. Allergy Asthma Proc
boards and received honoraria from Avontec, Boehringer Ingelheim,
2016; 37: 147–53.
Chiesi, Essex/Schering-Plough, GlaxoSmithKline, Janssen-Cilag, MEDA,
6 Delea TE, Hagiwara M, Stanford RH, Stempel D. Effects of
MSD, Mundipharma, Novartis, Paul-Ehrlich Institut, Regeneron,
fluticasone propionate/salmeterol combination on asthma-related
Revotar, Roche, Sanofi-Aventis, Sanofi/Regeneron, Sandoz-Hexal, TEVA, health care resource utilization and costs and adherence in children
and UCB/Schwarz-Pharma; received funding for research from and adults with asthma. Clin Ther 2008; 30: 560–71.
Deutsche Forschungsgesellschaft, Land Mecklenburg-Vorpommern, 7 Marceau C, Lemière C, Berbiche D, Perreault S, Blais L.
GlaxoSmithKline, and MSD; and has advised the Bemeinsame Persistence, adherence, and effectiveness of combination therapy
Bundesausschuss (GBA). PK reports personal fees from Chiesi, among adult patients with asthma. J Allergy Clin Immunol 2006;
Novartis, AstraZeneca, Boehringer Ingelheim, Berlin Chemie Menarini, 118: 574–81.
Adamed, Polpharma, and Lekam outside of the submitted work. 8 Stoloff SW, Stempel DA, Meyer J, Stanford RH, Carranza Rosenzweig
PP reports grants and personal fees from AstraZeneca and Chiesi, and JR. Improved refill persistence with fluticasone propionate and
personal fees from GlaxoSmithKline, Menarini, Mundipharma, salmeterol in a single inhaler compared with other controller
Novartis, and Sanofi outside of the submitted work. AP reports grants, therapies. J Allergy Clin Immunol 2004; 113: 245–51.
personal fees, non-financial support, payment for advisory board 9 Stempel DA, Stoloff SW, Carranza Rosenzweig JR, Stanford RH,
membership, payment for consultancy, payment for lectures, grants for Ryskina KL, Legorreta AP. Adherence to asthma controller
research, and travel expenses reimbursement from Chiesi Farmaceutici, medication regimens. Respir Med 2005; 99: 1263–67.
AstraZeneca, GlaxoSmithKline, Boehringer Ingelheim, Mundipharma, 10 Lipworth B, Manoharan A, Anderson W. Unlocking the quiet zone: the
and TEVA; and personal fees and non-financial support from Menarini, small airway asthma phenotype. Lancet Respir Med 2014; 2: 497–506.
Novartis, Zambon, and Sanofi outside of the submitted work. DS reports 11 Postma DS, Brightling C, Baldi S, et al. Exploring the relevance and
personal fees from Chiesi Farmaceutici during the conduct of the study extent of small airways dysfunction in asthma (ATLANTIS):
and personal fees from AstraZeneca, Boehringer Ingelheim, Chiesi baseline data from a prospective cohort study. Lancet Respir Med
Farmaceutici, Cipla, Genentech, GlaxoSmithKline, Glenmark, Menarini, 2019; 7: 402–16.
Mundipharma, Novartis, Peptinnovate, Pfizer, Pulmatrix, Therevance, 12 Virchow JC, Backer V, de Blay F, et al. Defining moderate asthma
and Verona outside of the submitted work. SC, FZ, AV, MK, and SP are exacerbations in clinical trials based on ATS/ERS joint statement.
Respir Med 2015; 109: 547–56.
employees of Chiesi Farmaceutici. GG is an employee of Chiesi USA.
GWC reports personal fees from A Menarini, Alk-Abello, Allergy 13 Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR.
A simulation study of the number of events per variable in logistic
Therapeutics, AstraZeneca-Medimmune, Boehringer Ingelheim,
regression analysis. J Clin Epidemiol 1996; 49: 1373–79.
Chiesi Farmaceutici, Genentech, Guidotti-Malesci, GlaxoSmithKline,
14 Concato J, Peduzzi P, Holford TR, Feinstein AR. Importance of
Hal Allergy, MSD, Mundipharma, Novartis, Orion, Sanofi-Aventis,
events per independent variable in proportional hazards analysis I.
Sanofi Genzyme/Regeneron, Stallergenes-Greer, Uriach Pharma, TEVA, Background, goals, and general strategy. J Clin Epidemiol 1995;
Valeas, and ViforPharma outside of the submitted work. 48: 1495–501.
Data sharing 15 Peduzzi P, Concato J, Feinstein AR, Holford TR. Importance of
Chiesi Farmaceutici is committed to conducting legitimate research and events per independent variable in proportional hazards regression
sharing with qualified scientific and medical researchers the anonymised analysis. II. Accuracy and precision of regression estimates.
J Clin Epidemiol 1995; 48: 1503–10.
patient-level and study-level data, clinical protocol, and full clinical study
report of Chiesi Farmaceutici sponsored interventional clinical trials in 16 Ortega HG, Liu MC, Pavord ID, et al. Mepolizumab treatment in
patients with severe eosinophilic asthma. N Engl J Med 2014;
patients for medicines and indications approved by the European
371: 1198–207.
12 www.thelancet.com Published online September 30, 2019 https://doi.org/10.1016/S0140-6736(19)32215-9
Articles
17 Chupp GL, Bradford ES, Albers FC, et al. Efficacy of mepolizumab 22 Dahl R, Engel M, Dusser D, et al. Safety and tolerability of
add-on therapy on health-related quality of life and markers of once-daily tiotropium respimat as add-on to at least inhaled
asthma control in severe eosinophilic asthma (MUSCA): corticosteroids in adult patients with symptomatic asthma: a pooled
a randomised, double-blind, placebo-controlled, parallel-group, safety analysis. Respir Med 2016; 118: 102–11.
multicentre, phase 3b trial. Lancet Respir Med 2017; 5: 390–400. 23 Echave M, Ojanguren ME, Elias I, et al. Cost-effectiveness of
18 Bleecker ER, FitzGerald JM, Chanez P, et al. Efficacy and safety of tiotropium in the treatment of patients with asthma. Value Health
benralizumab for patients with severe asthma uncontrolled with 2015; 18: A501–02.
high-dosage inhaled corticosteroids and long-acting β2-agonists 24 Willson J, Bateman ED, Pavord I, Lloyd A, Krivasi T, Esser D.
(SIROCCO): a randomised, multicentre, placebo-controlled Cost effectiveness of tiotropium in patients with asthma poorly
phase 3 trial. Lancet 2016; 388: 2115–27. controlled on inhaled glucocorticosteroids and long-acting
19 FitzGerald JM, Bleecker ER, Nair P, et al. Benralizumab, β-agonists. Appl Health Econ Health Policy 2014; 12: 447–59.
an anti-interleukin-5 receptor α monoclonal antibody, as add-on 25 Zafari Z, Sadatsafavi M, Mark FitzGerald J. Cost-effectiveness of
treatment for patients with severe, uncontrolled, eosinophilic tiotropium versus omalizumab for uncontrolled allergic asthma in
asthma (CALIMA): a randomised, double-blind, placebo-controlled US. Cost Eff Resour Alloc 2018; 16: 3.
phase 3 trial. Lancet 2016; 388: 2128–41. 26 Pawlik M, Walczak J, Pieniazek I. Economic evaluation of
20 Castro M, Corren J, Pavord ID, et al. Dupilumab efficacy and safety tiotropium administrated through the respimat inhaler as add-on
in moderate-to-severe uncontrolled asthma. N Engl J Med 2018; therapy in patients with uncontrolled severe asthma in Poland.
378: 2486–96. Value Health 2015; 18: A502.
21 Yaghoubi M, Adibi A, Safari A, FitzGerald JM, Sadatsafavi M. 27 Silva Miguel L, Manaças M, Pinheiro B. Economic evaluation of
The projected economic and health burden of uncontrolled asthma tiotropium for severe persistent asthma in Portugal. Value Health
in the United States. Am J Respir Crit Care Med 2019; published 2015; 18: A502.
online June 5. DOI:10.1164/rccm.201901-0016OC.
www.thelancet.com Published online September 30, 2019 https://doi.org/10.1016/S0140-6736(19)32215-9 13
You might also like
- Familias Psicosomaticas (Salvador Minuchin, Bernice L. Rosman, Lester BakeDocument366 pagesFamilias Psicosomaticas (Salvador Minuchin, Bernice L. Rosman, Lester BakeRamoncito77100% (4)
- ICU Note Writing GuidelinesDocument2 pagesICU Note Writing GuidelinesMohammedNo ratings yet
- Implants in Maxillofacial Prosthodontics PDFDocument50 pagesImplants in Maxillofacial Prosthodontics PDFankita50% (2)
- Tribute TrialDocument9 pagesTribute TrialMr. LNo ratings yet
- TRIBUTE Manuscript Peer Amends 19 Jan 2018 PostDocument28 pagesTRIBUTE Manuscript Peer Amends 19 Jan 2018 PostOdessa EnriquezNo ratings yet
- Paper Alumnos 5Document14 pagesPaper Alumnos 5Victor Martinez HagenNo ratings yet
- Ethos 2020Document14 pagesEthos 2020Radu CiprianNo ratings yet
- Terapia Triple para EPOCDocument14 pagesTerapia Triple para EPOCSebastian Cebrian GuerreroNo ratings yet
- Ok O'ByrneDocument12 pagesOk O'ByrneChristian OliveiraNo ratings yet
- KRONOS Study - PaperDocument12 pagesKRONOS Study - PaperRadu CiprianNo ratings yet
- Guselkumab in Patients With Active PsA Who Were Biologic-naive or Had Previously Received TNFα DISCOVER-1Document11 pagesGuselkumab in Patients With Active PsA Who Were Biologic-naive or Had Previously Received TNFα DISCOVER-1Edmundo RomanoNo ratings yet
- 10 1056@NEJMoa1715274Document12 pages10 1056@NEJMoa1715274Paul ParrasNo ratings yet
- Guglielmetti Et Al., 2017Document11 pagesGuglielmetti Et Al., 2017hasan andrianNo ratings yet
- 11 Years' Follow-Up of Trastuzumab After Adjuvant Chemotherapy in HER2-positive Early Breast CancerDocument11 pages11 Years' Follow-Up of Trastuzumab After Adjuvant Chemotherapy in HER2-positive Early Breast CancermaleticjNo ratings yet
- 38 Pertuzumab UslessDocument13 pages38 Pertuzumab Uslessbawoji1763No ratings yet
- Outpatient Treatment of COVID-19 and Incidence of post-COVID-19 Condition Over 10 MonthsDocument11 pagesOutpatient Treatment of COVID-19 and Incidence of post-COVID-19 Condition Over 10 MonthsStavya DubeyNo ratings yet
- LatitudeDocument15 pagesLatitudeJulio MineraNo ratings yet
- FichaDocument9 pagesFichamariaNo ratings yet
- 2 BaeDocument7 pages2 BaeMaria Elisa MartínezNo ratings yet
- Trastuzumab Deruxtecan (DS-8201a) in Patients With Advanced HER2-positive Gastric Cancer: A Dose-Expansion, Phase 1 StudyDocument10 pagesTrastuzumab Deruxtecan (DS-8201a) in Patients With Advanced HER2-positive Gastric Cancer: A Dose-Expansion, Phase 1 Studybawoji1763No ratings yet
- Tofacitinib For Psoriatic Arthritis in Patients With An Inadequate Response To TNF InhibitorsDocument12 pagesTofacitinib For Psoriatic Arthritis in Patients With An Inadequate Response To TNF InhibitorsPutri YunandaNo ratings yet
- SELECT-MONOTHERAPY FullDocument9 pagesSELECT-MONOTHERAPY FullAlaitz GurreaNo ratings yet
- Adalimumab Added To A Treat-To-target With MTX and I-Art Triamcinolone in Early RADocument10 pagesAdalimumab Added To A Treat-To-target With MTX and I-Art Triamcinolone in Early RAElenaChiriacovaNo ratings yet
- 2013 Burmester (TOFA Vs PLA)Document10 pages2013 Burmester (TOFA Vs PLA)Marcel JinihNo ratings yet
- Articulo NeumologiaDocument11 pagesArticulo NeumologiaHernandoJoseViloriaSanchezNo ratings yet
- A Randomized Clinical TrialDocument11 pagesA Randomized Clinical TrialRandy PrayogoNo ratings yet
- Torres 2017Document11 pagesTorres 2017Richardo SaputroNo ratings yet
- Procalcitonin-Guided Use of Antibiotics For Lower Respiratory Tract InfectionDocument14 pagesProcalcitonin-Guided Use of Antibiotics For Lower Respiratory Tract InfectionAbulHasan Idrus IstarNo ratings yet
- Adherence To Oral Hypoglycemic MedicatioDocument20 pagesAdherence To Oral Hypoglycemic Medicatioashenafi woldesenbetNo ratings yet
- Original Research Article: Anurag Bijalwan, Pradeep Singhal, Syed AltamashDocument7 pagesOriginal Research Article: Anurag Bijalwan, Pradeep Singhal, Syed Altamashagus sukarnaNo ratings yet
- Jcem2157 PDFDocument6 pagesJcem2157 PDFRidwan Putra Beng-BengNo ratings yet
- Ahmad 2018Document14 pagesAhmad 2018Cristopher OchoaNo ratings yet
- Betalactamicos NAC RCT ENI Lancet 2021 PDFDocument9 pagesBetalactamicos NAC RCT ENI Lancet 2021 PDFLindsay PinargottyNo ratings yet
- Jamacardiology Cotter 2023 Oi 230063 1706752510.55879Document11 pagesJamacardiology Cotter 2023 Oi 230063 1706752510.55879qbn8zhzhwhNo ratings yet
- Discontinuing β-lactam treatment after 3 days for patients with community-acquired pneumonia in non-critical care wards (PTC) : a double-blind, randomised, placebo-controlled, non-inferiority trialDocument9 pagesDiscontinuing β-lactam treatment after 3 days for patients with community-acquired pneumonia in non-critical care wards (PTC) : a double-blind, randomised, placebo-controlled, non-inferiority trialSil BalarezoNo ratings yet
- Eectiveness Tolerability and Safety of Tofacitinib inDocument14 pagesEectiveness Tolerability and Safety of Tofacitinib indanny gomezNo ratings yet
- 1 s2.0 S235230262300073X MainDocument12 pages1 s2.0 S235230262300073X MainjaysuriarNo ratings yet
- Jjco/hyaa 030Document11 pagesJjco/hyaa 030yazidNo ratings yet
- Abiraterone Acetate Plus Prednisone Versus Placebo Abiratetone LancetDocument9 pagesAbiraterone Acetate Plus Prednisone Versus Placebo Abiratetone LancetMahesh TamhaneNo ratings yet
- Efficacy and Safety of Methotrexate Versus Placebo As Add - 2020 - Journal of THDocument4 pagesEfficacy and Safety of Methotrexate Versus Placebo As Add - 2020 - Journal of THBruno MañonNo ratings yet
- Methods: Brief CommunicationDocument4 pagesMethods: Brief CommunicationKamila FunayamaNo ratings yet
- PIIS0954611118301215Document9 pagesPIIS0954611118301215TheRainMelodyNo ratings yet
- Rheumatology Kev006 FullDocument7 pagesRheumatology Kev006 FullMajito DondioNo ratings yet
- New England Journal Medicine: The ofDocument11 pagesNew England Journal Medicine: The ofsufaNo ratings yet
- Articles: BackgroundDocument10 pagesArticles: BackgroundTatanNo ratings yet
- Withdrawal of Inhaled GlucocorticoidsDocument10 pagesWithdrawal of Inhaled GlucocorticoidsAndi MarwansyahNo ratings yet
- PIIS2213260017304745Document10 pagesPIIS2213260017304745Juan Pablo CasanovaNo ratings yet
- Moxifloxaxin For CAPDocument9 pagesMoxifloxaxin For CAPmateri posNo ratings yet
- Traa 144Document9 pagesTraa 144RashifNo ratings yet
- 1 s2.0 S0140673623020330 Main 2Document12 pages1 s2.0 S0140673623020330 Main 2Uriel EnriquezNo ratings yet
- Beclometasone-Formoterol As Maintenance and Reliever Treatment in Patients With Asthma: A Double-Blind, Randomised Controlled TrialDocument9 pagesBeclometasone-Formoterol As Maintenance and Reliever Treatment in Patients With Asthma: A Double-Blind, Randomised Controlled TrialArief WibowoNo ratings yet
- Effectiveness of 3 Generation Cephalosporin Compare To 3 Generation Cephalosporin - Macrolides For Community Acquired Pneumonia PatientsDocument10 pagesEffectiveness of 3 Generation Cephalosporin Compare To 3 Generation Cephalosporin - Macrolides For Community Acquired Pneumonia PatientslalaNo ratings yet
- AntibioticsDocument10 pagesAntibioticsosamayasser82No ratings yet
- GJHS 5 150Document5 pagesGJHS 5 150Wisnu Aditya WardanaNo ratings yet
- PIIS2213260023004186Document11 pagesPIIS2213260023004186teresa mendozaNo ratings yet
- High-Dosage Betahistine Dihydrochloride Between 28Document4 pagesHigh-Dosage Betahistine Dihydrochloride Between 28smdj1975No ratings yet
- Haloperidol RX Delirium Metaanalysis July 2023Document9 pagesHaloperidol RX Delirium Metaanalysis July 2023Jonty ArputhemNo ratings yet
- ARDS Meduri JAMA 1998Document8 pagesARDS Meduri JAMA 1998Rivaneide AmorimNo ratings yet
- A Randomized Controlled Trial Comparing Ketorolac and Triamcinolone Injections in Adults With Trigger DigitsDocument6 pagesA Randomized Controlled Trial Comparing Ketorolac and Triamcinolone Injections in Adults With Trigger DigitsRazan FSHLNo ratings yet
- Original ContributionsDocument6 pagesOriginal ContributionsJennSweeNo ratings yet
- Antacid Therapy and Disease Progression in Patients With Idiopathic Pulmonary Fibrosis Who Received PirfenidoneDocument9 pagesAntacid Therapy and Disease Progression in Patients With Idiopathic Pulmonary Fibrosis Who Received PirfenidoneAquiles CastroNo ratings yet
- Top Trials in Gastroenterology & HepatologyFrom EverandTop Trials in Gastroenterology & HepatologyRating: 4.5 out of 5 stars4.5/5 (7)
- Lab Dept/Section: Microbiology/Virology Test Name: Sputum Culture and Gram StainDocument4 pagesLab Dept/Section: Microbiology/Virology Test Name: Sputum Culture and Gram StainAdn crnNo ratings yet
- Broilers &layers Yaras MaccharlesDocument38 pagesBroilers &layers Yaras MaccharlesNyasha VincentNo ratings yet
- Immunosuppressant DrugsDocument28 pagesImmunosuppressant DrugsimnasNo ratings yet
- Resistance Band Workout BookDocument160 pagesResistance Band Workout BookGOVARDHAN100% (3)
- 9 ItemDocument11 pages9 ItemNguyễn HP ThảoNo ratings yet
- Chapter 3-6 Biological HazardsDocument28 pagesChapter 3-6 Biological Hazards000No ratings yet
- Right Upper Quadrant Pain: William MiddletonDocument14 pagesRight Upper Quadrant Pain: William MiddletonAmalia Gh,No ratings yet
- Exploring The Impact of Neurodevelopmental Dis Orde Rs in Famili Es - PreprintDocument29 pagesExploring The Impact of Neurodevelopmental Dis Orde Rs in Famili Es - Preprintnathalia.freitasNo ratings yet
- Overview of CMAMDocument33 pagesOverview of CMAMMd Faruque Ahmad100% (1)
- OSHJ-CoP-16 First Aid at Work Version 1 EnglishDocument12 pagesOSHJ-CoP-16 First Aid at Work Version 1 EnglishsajinNo ratings yet
- Burns DressingDocument4 pagesBurns DressingBalaMuruganNo ratings yet
- 18 Diseases of Passion Fruit PDFDocument29 pages18 Diseases of Passion Fruit PDFmvbgarciaNo ratings yet
- OB-Reviewer With AlgorithmDocument29 pagesOB-Reviewer With Algorithmriczen mae vilaNo ratings yet
- Histamine H 2 Receptor Antagonists For DecreasingDocument10 pagesHistamine H 2 Receptor Antagonists For DecreasingYulian 53No ratings yet
- PATH - Bony Injuries (Fractures) (8p) PDFDocument8 pagesPATH - Bony Injuries (Fractures) (8p) PDFandreeaNo ratings yet
- #410 Heavy LiftDocument3 pages#410 Heavy LiftTolias EgwNo ratings yet
- Malawi Public Health ActDocument63 pagesMalawi Public Health ActKondwani AndreahNo ratings yet
- Research Paper About Effects of Air PollutionDocument7 pagesResearch Paper About Effects of Air Pollutionjtbowtgkf100% (1)
- Music: Dr. Vicente F. Gustilo Memorial National High School Mapeh 9 1 Quarter Summative AssessmentDocument5 pagesMusic: Dr. Vicente F. Gustilo Memorial National High School Mapeh 9 1 Quarter Summative AssessmentSirDadz BornalesNo ratings yet
- Effect of Lipid Based Nutrient Supplements On Micronutrie 2024 The AmericanDocument9 pagesEffect of Lipid Based Nutrient Supplements On Micronutrie 2024 The AmericanridhoNo ratings yet
- Assessment of Six Cardiovascular Risk Calculators...Document7 pagesAssessment of Six Cardiovascular Risk Calculators...Ale VillarNo ratings yet
- Pengetahuan Tentang Cacingan Dan Upaya Pencegahan Kecacingan Oleh: Ganda Sigalingging, Selli Dosriani Sitopu, Dita Wiranti DaeliDocument9 pagesPengetahuan Tentang Cacingan Dan Upaya Pencegahan Kecacingan Oleh: Ganda Sigalingging, Selli Dosriani Sitopu, Dita Wiranti DaeliMorida FanadierNo ratings yet
- Disorders of PerceptionDocument67 pagesDisorders of PerceptionPriyash JainNo ratings yet
- NCP2 - Active PhaseDocument14 pagesNCP2 - Active PhasepriyankaNo ratings yet
- Indian Bar Association: Most Urgent & Most SeriousDocument42 pagesIndian Bar Association: Most Urgent & Most SerioussatiishmiishraNo ratings yet
- Gallbladder Polyps - UpToDateDocument19 pagesGallbladder Polyps - UpToDateTrần Quốc KhánhNo ratings yet
- International Journal of Pediatric Research Ijpr 8 088Document6 pagesInternational Journal of Pediatric Research Ijpr 8 088desiNo ratings yet