
Chrepa Et Al 2023 Cannabidiol As An Alternative Analgesic For Acute Dental Pain
Chrepa Et Al 2023 Cannabidiol As An Alternative Analgesic For Acute Dental Pain
You might also like
- NHS Standard Application FormDocument17 pagesNHS Standard Application FormDanielaNo ratings yet
- DK Publishing - Neal's Yard Remedies Complete Massage - All The Techniques, Disciplines, and Skills You Need To Massage For Wellness (2019, DK) PDFDocument248 pagesDK Publishing - Neal's Yard Remedies Complete Massage - All The Techniques, Disciplines, and Skills You Need To Massage For Wellness (2019, DK) PDFSolveig100% (2)
- NP 5Document6 pagesNP 5Ana Blesilda Cachola100% (1)
- An Evaluation of The Feasibility, Acceptability, and Preliminary Efficacy of Cognitive-Behavioral Therapy For Opioid Use Disorder and Chronic PainDocument20 pagesAn Evaluation of The Feasibility, Acceptability, and Preliminary Efficacy of Cognitive-Behavioral Therapy For Opioid Use Disorder and Chronic PainMario LopesNo ratings yet
- JConservDent224356-759521 210552Document6 pagesJConservDent224356-759521 210552Shwetank ShrivastavaNo ratings yet
- Betametasona PostDocument6 pagesBetametasona PostTATIANA BARRIOS ESCORCIANo ratings yet
- Antibiotic and Analgesic Prescription Patterns Among Dentists or Management of Dental Pain and Infection During Endodontic TreatmentDocument7 pagesAntibiotic and Analgesic Prescription Patterns Among Dentists or Management of Dental Pain and Infection During Endodontic TreatmentAhmed Abdulleh Al Hada'aNo ratings yet
- Jama Sandhu 2023 Oi 230045 1684251840.4758Document12 pagesJama Sandhu 2023 Oi 230045 1684251840.4758Byanca AlvesNo ratings yet
- Managing Acute Dental Pain Without CodeineDocument1 pageManaging Acute Dental Pain Without CodeineSejal MishraNo ratings yet
- 2017 JADAGoodchildand Donaldson New Sedationand General Anesthesia GuidelinesDocument6 pages2017 JADAGoodchildand Donaldson New Sedationand General Anesthesia GuidelinesGabriel SchonvandtNo ratings yet
- 1692 4803 1 PBDocument5 pages1692 4803 1 PBDinda DeliaNo ratings yet
- Article History: A, B A C D e B, F BDocument13 pagesArticle History: A, B A C D e B, F BNataliaNo ratings yet
- Local Anesthetic Literature ReviewDocument6 pagesLocal Anesthetic Literature Reviewapi-703336450No ratings yet
- Agga Rwal 2021Document11 pagesAgga Rwal 2021respaldonatie4No ratings yet
- The Open Dentistry Journal: Methodologies in Orthodontic Pain Management: A ReviewDocument6 pagesThe Open Dentistry Journal: Methodologies in Orthodontic Pain Management: A Reviewnevin santhoshNo ratings yet
- Angle 2019 Effectiveness of Verbal Behavior Modification and Acetaminophen OnDocument7 pagesAngle 2019 Effectiveness of Verbal Behavior Modification and Acetaminophen OnTarif HamshoNo ratings yet
- APJCP Volume21 Issue7 Pages1851-1866 RemovedDocument8 pagesAPJCP Volume21 Issue7 Pages1851-1866 RemovednorbertwuNo ratings yet
- Effect of Long Acting Local Anesthetic On PostoperDocument4 pagesEffect of Long Acting Local Anesthetic On PostoperJavier Farias VeraNo ratings yet
- Hypnotherapy For The Treatment of Persistent Pain: A Literature ReviewDocument5 pagesHypnotherapy For The Treatment of Persistent Pain: A Literature ReviewAhmad SyaripudinNo ratings yet
- European Journal of Pain - 2019 - Aggarwal - The Effectiveness of Self Management Interventions in Adults With ChronicDocument17 pagesEuropean Journal of Pain - 2019 - Aggarwal - The Effectiveness of Self Management Interventions in Adults With ChronicNatalie JaraNo ratings yet
- Comparative Study To Evaluate The Effectiveness of Aloe Vera and Metronidazole in Adjunct To Scaling and Root Planing in Periodontitis PatientsDocument4 pagesComparative Study To Evaluate The Effectiveness of Aloe Vera and Metronidazole in Adjunct To Scaling and Root Planing in Periodontitis Patientsnaimatus225No ratings yet
- Effect of Transcodent Painless Needles On Injection PainDocument6 pagesEffect of Transcodent Painless Needles On Injection Painmohammadreza hajialiNo ratings yet
- Research PosterDocument1 pageResearch Posterapi-539065201No ratings yet
- Manual Therapy in The Treatment of Myofascial Pain Related To Temporomandibular Disorders: A Systematic ReviewDocument11 pagesManual Therapy in The Treatment of Myofascial Pain Related To Temporomandibular Disorders: A Systematic ReviewJardiel JimenezNo ratings yet
- Cannabidiol Treatment in Hand Osteoarthritis And.26Document9 pagesCannabidiol Treatment in Hand Osteoarthritis And.26Róbson BatistaNo ratings yet
- Jurnal 1Document16 pagesJurnal 1Made WindaNo ratings yet
- Research Paper Final Group 7Document17 pagesResearch Paper Final Group 7api-738778945No ratings yet
- Research Paper Final DraftDocument17 pagesResearch Paper Final Draftapi-740628337No ratings yet
- Jama Krebs 2018 Oi 180013Document11 pagesJama Krebs 2018 Oi 180013Yeison UrregoNo ratings yet
- Effects of Short-Wave Therapy in Patients With Knee Osteoarthritis: A Systematic Review and Meta-AnalysisDocument12 pagesEffects of Short-Wave Therapy in Patients With Knee Osteoarthritis: A Systematic Review and Meta-AnalysisIvone Cruzado UrcoNo ratings yet
- 利用纳米技术通过新型无药局部止痛贴片改善疼痛和功能Document20 pages利用纳米技术通过新型无药局部止痛贴片改善疼痛和功能shexinyejianNo ratings yet
- The Argument For Enhanced Use of Complementary and Alternative Therapies in Chronic Pain ManagementDocument4 pagesThe Argument For Enhanced Use of Complementary and Alternative Therapies in Chronic Pain ManagementquadrospauloNo ratings yet
- Cannabinoids Medical PDFDocument18 pagesCannabinoids Medical PDFmgarbini8361No ratings yet
- Regional Anesthetic Blocks For Donor SiteDocument10 pagesRegional Anesthetic Blocks For Donor SiteLuana SakamotoNo ratings yet
- Efficacy Tolerability and Safety of Nonph Therapies For Chronic Pain CAMDocument15 pagesEfficacy Tolerability and Safety of Nonph Therapies For Chronic Pain CAMMiguel TrillosNo ratings yet
- Effect of Occlusal Reduction On Postoperative PainDocument4 pagesEffect of Occlusal Reduction On Postoperative PainMihaela TuculinaNo ratings yet
- Revisão Integrativa Sobre Dor Cronica e TCC Knoerl2015Document33 pagesRevisão Integrativa Sobre Dor Cronica e TCC Knoerl2015RafaelNo ratings yet
- Austin Journal of Orthopedics & RheumatologyDocument6 pagesAustin Journal of Orthopedics & RheumatologyAustin Publishing GroupNo ratings yet
- Cureus 0014 00000026489Document14 pagesCureus 0014 00000026489Cristhian UnigarroNo ratings yet
- Jurnal Asli JR IKGMP - Daniella Lunetta S M - 220160100111022Document7 pagesJurnal Asli JR IKGMP - Daniella Lunetta S M - 220160100111022DaniellaNo ratings yet
- The Effect of High-Intensity Versus Low-Level Laser Therapy in The Management of Plantar Fasciitis: Randomized Participant Blind Controlled TrialDocument11 pagesThe Effect of High-Intensity Versus Low-Level Laser Therapy in The Management of Plantar Fasciitis: Randomized Participant Blind Controlled TrialFaeyz OrabiNo ratings yet
- Fphar 11 00561Document7 pagesFphar 11 00561Brayan PazmiñoNo ratings yet
- Opioid-Induced Constipation: Advances and Clinical Guidance: Alfred D. Nelson and Michael CamilleriDocument14 pagesOpioid-Induced Constipation: Advances and Clinical Guidance: Alfred D. Nelson and Michael Camillerifebyan yohanesNo ratings yet
- Frontiers Frvir-04-1195196 07252023Document12 pagesFrontiers Frvir-04-1195196 07252023Robert CarrilloNo ratings yet
- Jurnal LV Ipd 11Document8 pagesJurnal LV Ipd 11Dudeperfect666No ratings yet
- Submucosal Diclofenac for Acute Postoperative Pain in Third Molar Surgery A Randomized, Controlled Clinical Trial.Document7 pagesSubmucosal Diclofenac for Acute Postoperative Pain in Third Molar Surgery A Randomized, Controlled Clinical Trial.Tatiana ChambaNo ratings yet
- Endo EngDocument8 pagesEndo EngandreeaNo ratings yet
- Opioids For Chronic Pain ManagementDocument45 pagesOpioids For Chronic Pain ManagementaartiNo ratings yet
- Clinical Data For Use of Cannabis A ReviewDocument35 pagesClinical Data For Use of Cannabis A ReviewCarlos Ferrete JuniorNo ratings yet
- Medical Marijuana: Do The Benefits Outweigh The Risks?: Current Psychiatry January 2018Document9 pagesMedical Marijuana: Do The Benefits Outweigh The Risks?: Current Psychiatry January 2018chuli chwaNo ratings yet
- European Journal of Pain - 2022 - Bialas - Long Te - 240229 - 120410Document13 pagesEuropean Journal of Pain - 2022 - Bialas - Long Te - 240229 - 120410d.catoNo ratings yet
- Policy On Pediatric Dental Pain ManagementDocument3 pagesPolicy On Pediatric Dental Pain ManagementمعتزباللهNo ratings yet
- Biodanza Reduces Acute Pain Severity in Women With Fibromyalgia (2017)Document10 pagesBiodanza Reduces Acute Pain Severity in Women With Fibromyalgia (2017)ermesNo ratings yet
- Painreports 2 E589Document7 pagesPainreports 2 E589goliath.chad2000No ratings yet
- Intravitreal InjectionDocument8 pagesIntravitreal InjectionSesria Nasution100% (1)
- Changes in Symptoms of Anxiety, Depression, and PTSD in An RCT-study of Dentist-Administered Treatment of Dental AnxietyDocument11 pagesChanges in Symptoms of Anxiety, Depression, and PTSD in An RCT-study of Dentist-Administered Treatment of Dental AnxietyMaria GuzuNo ratings yet
- Pharmacology Literature ReviewDocument6 pagesPharmacology Literature Reviewapi-703889166No ratings yet
- Comparison of Short-Term Oral Impacts Experienced by Patients Treated With Invisalign or Conventional Fixed Orthodontic AppliancesDocument7 pagesComparison of Short-Term Oral Impacts Experienced by Patients Treated With Invisalign or Conventional Fixed Orthodontic AppliancesGery KrismawanNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument7 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Tetrahydrocannabinol (THC), Cannabidiol (CBD), and Other Similar Compounds (Medlineplus, 2020) - According ToDocument5 pagesTetrahydrocannabinol (THC), Cannabidiol (CBD), and Other Similar Compounds (Medlineplus, 2020) - According ToJade PimentelNo ratings yet
- ArthritisDocument9 pagesArthritisBharath BeeNo ratings yet
- Symbiosis: Journal of Exercise, Sports & OrthopedicsDocument6 pagesSymbiosis: Journal of Exercise, Sports & OrthopedicsFerryGoNo ratings yet
- Jurnal Bahasa Inggris Pencegahan Infeksi Pada KateterDocument3 pagesJurnal Bahasa Inggris Pencegahan Infeksi Pada KateterArifNo ratings yet
- Pudendal Nerve BlockDocument3 pagesPudendal Nerve BlockLauraNo ratings yet
- Comparison of Open and Laproscopic Live Donor NephrectomyDocument7 pagesComparison of Open and Laproscopic Live Donor NephrectomyEhab Omar El HalawanyNo ratings yet
- JTDocument2 pagesJTAdade Solomon Yao-Say0% (1)
- Touch in CounselingDocument25 pagesTouch in Counselingnicolas.zollerNo ratings yet
- Stephen EDocument376 pagesStephen ESeba Lannoo100% (4)
- Nursing Care Plan FinalDocument16 pagesNursing Care Plan FinalErickson OcialNo ratings yet
- NCP (Fatigue)Document1 pageNCP (Fatigue)student_019100% (1)
- VIS Report FialDocument16 pagesVIS Report FialAyaz MahmoodNo ratings yet
- Monnal T75 EspecificacionesDocument9 pagesMonnal T75 EspecificacionesekawahonoNo ratings yet
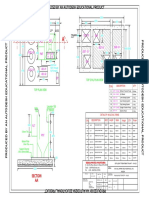
- Plan Layout For ETP - 10 KLD-ModelDocument1 pagePlan Layout For ETP - 10 KLD-Modellionisback100% (1)
- Hydrotherapy: A ReviewDocument5 pagesHydrotherapy: A ReviewAyu Wita DewiNo ratings yet
- Tugas Individu Ke 1 PDFDocument8 pagesTugas Individu Ke 1 PDFneli rahayuNo ratings yet
- Baru 414.2.full PDFDocument6 pagesBaru 414.2.full PDFIrmagian PaleonNo ratings yet
- MPR-MS (Muscle Spasm) - 1299Document1 pageMPR-MS (Muscle Spasm) - 1299DanielleNo ratings yet
- Coleus Forskohlii and Its Forskolin A ReviewDocument5 pagesColeus Forskohlii and Its Forskolin A ReviewESSENCE - International Journal for Environmental Rehabilitation and ConservaionNo ratings yet
- Vega Remediation Project: September 2020Document5 pagesVega Remediation Project: September 2020Stanescu BogdanNo ratings yet
- Commonrashes in Neonates201205suDocument6 pagesCommonrashes in Neonates201205suDanielcc LeeNo ratings yet
- Changes in The Abdominal Wall After Anterior, Posterior, and Combined Component SeparationDocument11 pagesChanges in The Abdominal Wall After Anterior, Posterior, and Combined Component SeparationsamuelNo ratings yet
- Office Policy UpdatedDocument7 pagesOffice Policy Updatedapi-362969960No ratings yet
- Bio FoldersDocument11 pagesBio Foldersgoksel3173No ratings yet
- Management of Rifampicin-Resistant TB Booklet 1219 v6Document120 pagesManagement of Rifampicin-Resistant TB Booklet 1219 v6DudungNo ratings yet
- Toronto Western Spasmodic Torticollis Rating Scale TWSTRSDocument3 pagesToronto Western Spasmodic Torticollis Rating Scale TWSTRSVioleta López Neciosup0% (1)
- Lesinurad For The Treatment of Hyperuricaemia in People With GoutDocument24 pagesLesinurad For The Treatment of Hyperuricaemia in People With GoutPharmaEducationNo ratings yet
- Buy Crystal Methamphetamine OnlineDocument7 pagesBuy Crystal Methamphetamine Onlinezoe saldana100% (1)
- Orthodontic Treatment of Mandibular Anterior Crowding: Key Words: Crowding, Malocclusion, Labial FlaringDocument4 pagesOrthodontic Treatment of Mandibular Anterior Crowding: Key Words: Crowding, Malocclusion, Labial FlaringDunia Medisku OnlineShopNo ratings yet
- Perbedaan Penanganan Antara Laparoskopi Vs Open Repair Pada Perforasi GasterDocument7 pagesPerbedaan Penanganan Antara Laparoskopi Vs Open Repair Pada Perforasi GasterAfiani JannahNo ratings yet
























































































Download as pdf or txt
You might also like
- NHS Standard Application FormDocument17 pagesNHS Standard Application FormDanielaNo ratings yet
- DK Publishing - Neal's Yard Remedies Complete Massage - All The Techniques, Disciplines, and Skills You Need To Massage For Wellness (2019, DK) PDFDocument248 pagesDK Publishing - Neal's Yard Remedies Complete Massage - All The Techniques, Disciplines, and Skills You Need To Massage For Wellness (2019, DK) PDFSolveig100% (2)
- NP 5Document6 pagesNP 5Ana Blesilda Cachola100% (1)
- An Evaluation of The Feasibility, Acceptability, and Preliminary Efficacy of Cognitive-Behavioral Therapy For Opioid Use Disorder and Chronic PainDocument20 pagesAn Evaluation of The Feasibility, Acceptability, and Preliminary Efficacy of Cognitive-Behavioral Therapy For Opioid Use Disorder and Chronic PainMario LopesNo ratings yet
- JConservDent224356-759521 210552Document6 pagesJConservDent224356-759521 210552Shwetank ShrivastavaNo ratings yet
- Betametasona PostDocument6 pagesBetametasona PostTATIANA BARRIOS ESCORCIANo ratings yet
- Antibiotic and Analgesic Prescription Patterns Among Dentists or Management of Dental Pain and Infection During Endodontic TreatmentDocument7 pagesAntibiotic and Analgesic Prescription Patterns Among Dentists or Management of Dental Pain and Infection During Endodontic TreatmentAhmed Abdulleh Al Hada'aNo ratings yet
- Jama Sandhu 2023 Oi 230045 1684251840.4758Document12 pagesJama Sandhu 2023 Oi 230045 1684251840.4758Byanca AlvesNo ratings yet
- Managing Acute Dental Pain Without CodeineDocument1 pageManaging Acute Dental Pain Without CodeineSejal MishraNo ratings yet
- 2017 JADAGoodchildand Donaldson New Sedationand General Anesthesia GuidelinesDocument6 pages2017 JADAGoodchildand Donaldson New Sedationand General Anesthesia GuidelinesGabriel SchonvandtNo ratings yet
- 1692 4803 1 PBDocument5 pages1692 4803 1 PBDinda DeliaNo ratings yet
- Article History: A, B A C D e B, F BDocument13 pagesArticle History: A, B A C D e B, F BNataliaNo ratings yet
- Local Anesthetic Literature ReviewDocument6 pagesLocal Anesthetic Literature Reviewapi-703336450No ratings yet
- Agga Rwal 2021Document11 pagesAgga Rwal 2021respaldonatie4No ratings yet
- The Open Dentistry Journal: Methodologies in Orthodontic Pain Management: A ReviewDocument6 pagesThe Open Dentistry Journal: Methodologies in Orthodontic Pain Management: A Reviewnevin santhoshNo ratings yet
- Angle 2019 Effectiveness of Verbal Behavior Modification and Acetaminophen OnDocument7 pagesAngle 2019 Effectiveness of Verbal Behavior Modification and Acetaminophen OnTarif HamshoNo ratings yet
- APJCP Volume21 Issue7 Pages1851-1866 RemovedDocument8 pagesAPJCP Volume21 Issue7 Pages1851-1866 RemovednorbertwuNo ratings yet
- Effect of Long Acting Local Anesthetic On PostoperDocument4 pagesEffect of Long Acting Local Anesthetic On PostoperJavier Farias VeraNo ratings yet
- Hypnotherapy For The Treatment of Persistent Pain: A Literature ReviewDocument5 pagesHypnotherapy For The Treatment of Persistent Pain: A Literature ReviewAhmad SyaripudinNo ratings yet
- European Journal of Pain - 2019 - Aggarwal - The Effectiveness of Self Management Interventions in Adults With ChronicDocument17 pagesEuropean Journal of Pain - 2019 - Aggarwal - The Effectiveness of Self Management Interventions in Adults With ChronicNatalie JaraNo ratings yet
- Comparative Study To Evaluate The Effectiveness of Aloe Vera and Metronidazole in Adjunct To Scaling and Root Planing in Periodontitis PatientsDocument4 pagesComparative Study To Evaluate The Effectiveness of Aloe Vera and Metronidazole in Adjunct To Scaling and Root Planing in Periodontitis Patientsnaimatus225No ratings yet
- Effect of Transcodent Painless Needles On Injection PainDocument6 pagesEffect of Transcodent Painless Needles On Injection Painmohammadreza hajialiNo ratings yet
- Research PosterDocument1 pageResearch Posterapi-539065201No ratings yet
- Manual Therapy in The Treatment of Myofascial Pain Related To Temporomandibular Disorders: A Systematic ReviewDocument11 pagesManual Therapy in The Treatment of Myofascial Pain Related To Temporomandibular Disorders: A Systematic ReviewJardiel JimenezNo ratings yet
- Cannabidiol Treatment in Hand Osteoarthritis And.26Document9 pagesCannabidiol Treatment in Hand Osteoarthritis And.26Róbson BatistaNo ratings yet
- Jurnal 1Document16 pagesJurnal 1Made WindaNo ratings yet
- Research Paper Final Group 7Document17 pagesResearch Paper Final Group 7api-738778945No ratings yet
- Research Paper Final DraftDocument17 pagesResearch Paper Final Draftapi-740628337No ratings yet
- Jama Krebs 2018 Oi 180013Document11 pagesJama Krebs 2018 Oi 180013Yeison UrregoNo ratings yet
- Effects of Short-Wave Therapy in Patients With Knee Osteoarthritis: A Systematic Review and Meta-AnalysisDocument12 pagesEffects of Short-Wave Therapy in Patients With Knee Osteoarthritis: A Systematic Review and Meta-AnalysisIvone Cruzado UrcoNo ratings yet
- 利用纳米技术通过新型无药局部止痛贴片改善疼痛和功能Document20 pages利用纳米技术通过新型无药局部止痛贴片改善疼痛和功能shexinyejianNo ratings yet
- The Argument For Enhanced Use of Complementary and Alternative Therapies in Chronic Pain ManagementDocument4 pagesThe Argument For Enhanced Use of Complementary and Alternative Therapies in Chronic Pain ManagementquadrospauloNo ratings yet
- Cannabinoids Medical PDFDocument18 pagesCannabinoids Medical PDFmgarbini8361No ratings yet
- Regional Anesthetic Blocks For Donor SiteDocument10 pagesRegional Anesthetic Blocks For Donor SiteLuana SakamotoNo ratings yet
- Efficacy Tolerability and Safety of Nonph Therapies For Chronic Pain CAMDocument15 pagesEfficacy Tolerability and Safety of Nonph Therapies For Chronic Pain CAMMiguel TrillosNo ratings yet
- Effect of Occlusal Reduction On Postoperative PainDocument4 pagesEffect of Occlusal Reduction On Postoperative PainMihaela TuculinaNo ratings yet
- Revisão Integrativa Sobre Dor Cronica e TCC Knoerl2015Document33 pagesRevisão Integrativa Sobre Dor Cronica e TCC Knoerl2015RafaelNo ratings yet
- Austin Journal of Orthopedics & RheumatologyDocument6 pagesAustin Journal of Orthopedics & RheumatologyAustin Publishing GroupNo ratings yet
- Cureus 0014 00000026489Document14 pagesCureus 0014 00000026489Cristhian UnigarroNo ratings yet
- Jurnal Asli JR IKGMP - Daniella Lunetta S M - 220160100111022Document7 pagesJurnal Asli JR IKGMP - Daniella Lunetta S M - 220160100111022DaniellaNo ratings yet
- The Effect of High-Intensity Versus Low-Level Laser Therapy in The Management of Plantar Fasciitis: Randomized Participant Blind Controlled TrialDocument11 pagesThe Effect of High-Intensity Versus Low-Level Laser Therapy in The Management of Plantar Fasciitis: Randomized Participant Blind Controlled TrialFaeyz OrabiNo ratings yet
- Fphar 11 00561Document7 pagesFphar 11 00561Brayan PazmiñoNo ratings yet
- Opioid-Induced Constipation: Advances and Clinical Guidance: Alfred D. Nelson and Michael CamilleriDocument14 pagesOpioid-Induced Constipation: Advances and Clinical Guidance: Alfred D. Nelson and Michael Camillerifebyan yohanesNo ratings yet
- Frontiers Frvir-04-1195196 07252023Document12 pagesFrontiers Frvir-04-1195196 07252023Robert CarrilloNo ratings yet
- Jurnal LV Ipd 11Document8 pagesJurnal LV Ipd 11Dudeperfect666No ratings yet
- Submucosal Diclofenac for Acute Postoperative Pain in Third Molar Surgery A Randomized, Controlled Clinical Trial.Document7 pagesSubmucosal Diclofenac for Acute Postoperative Pain in Third Molar Surgery A Randomized, Controlled Clinical Trial.Tatiana ChambaNo ratings yet
- Endo EngDocument8 pagesEndo EngandreeaNo ratings yet
- Opioids For Chronic Pain ManagementDocument45 pagesOpioids For Chronic Pain ManagementaartiNo ratings yet
- Clinical Data For Use of Cannabis A ReviewDocument35 pagesClinical Data For Use of Cannabis A ReviewCarlos Ferrete JuniorNo ratings yet
- Medical Marijuana: Do The Benefits Outweigh The Risks?: Current Psychiatry January 2018Document9 pagesMedical Marijuana: Do The Benefits Outweigh The Risks?: Current Psychiatry January 2018chuli chwaNo ratings yet
- European Journal of Pain - 2022 - Bialas - Long Te - 240229 - 120410Document13 pagesEuropean Journal of Pain - 2022 - Bialas - Long Te - 240229 - 120410d.catoNo ratings yet
- Policy On Pediatric Dental Pain ManagementDocument3 pagesPolicy On Pediatric Dental Pain ManagementمعتزباللهNo ratings yet
- Biodanza Reduces Acute Pain Severity in Women With Fibromyalgia (2017)Document10 pagesBiodanza Reduces Acute Pain Severity in Women With Fibromyalgia (2017)ermesNo ratings yet
- Painreports 2 E589Document7 pagesPainreports 2 E589goliath.chad2000No ratings yet
- Intravitreal InjectionDocument8 pagesIntravitreal InjectionSesria Nasution100% (1)
- Changes in Symptoms of Anxiety, Depression, and PTSD in An RCT-study of Dentist-Administered Treatment of Dental AnxietyDocument11 pagesChanges in Symptoms of Anxiety, Depression, and PTSD in An RCT-study of Dentist-Administered Treatment of Dental AnxietyMaria GuzuNo ratings yet
- Pharmacology Literature ReviewDocument6 pagesPharmacology Literature Reviewapi-703889166No ratings yet
- Comparison of Short-Term Oral Impacts Experienced by Patients Treated With Invisalign or Conventional Fixed Orthodontic AppliancesDocument7 pagesComparison of Short-Term Oral Impacts Experienced by Patients Treated With Invisalign or Conventional Fixed Orthodontic AppliancesGery KrismawanNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument7 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Tetrahydrocannabinol (THC), Cannabidiol (CBD), and Other Similar Compounds (Medlineplus, 2020) - According ToDocument5 pagesTetrahydrocannabinol (THC), Cannabidiol (CBD), and Other Similar Compounds (Medlineplus, 2020) - According ToJade PimentelNo ratings yet
- ArthritisDocument9 pagesArthritisBharath BeeNo ratings yet
- Symbiosis: Journal of Exercise, Sports & OrthopedicsDocument6 pagesSymbiosis: Journal of Exercise, Sports & OrthopedicsFerryGoNo ratings yet
- Jurnal Bahasa Inggris Pencegahan Infeksi Pada KateterDocument3 pagesJurnal Bahasa Inggris Pencegahan Infeksi Pada KateterArifNo ratings yet
- Pudendal Nerve BlockDocument3 pagesPudendal Nerve BlockLauraNo ratings yet
- Comparison of Open and Laproscopic Live Donor NephrectomyDocument7 pagesComparison of Open and Laproscopic Live Donor NephrectomyEhab Omar El HalawanyNo ratings yet
- JTDocument2 pagesJTAdade Solomon Yao-Say0% (1)
- Touch in CounselingDocument25 pagesTouch in Counselingnicolas.zollerNo ratings yet
- Stephen EDocument376 pagesStephen ESeba Lannoo100% (4)
- Nursing Care Plan FinalDocument16 pagesNursing Care Plan FinalErickson OcialNo ratings yet
- NCP (Fatigue)Document1 pageNCP (Fatigue)student_019100% (1)
- VIS Report FialDocument16 pagesVIS Report FialAyaz MahmoodNo ratings yet
- Monnal T75 EspecificacionesDocument9 pagesMonnal T75 EspecificacionesekawahonoNo ratings yet
- Plan Layout For ETP - 10 KLD-ModelDocument1 pagePlan Layout For ETP - 10 KLD-Modellionisback100% (1)
- Hydrotherapy: A ReviewDocument5 pagesHydrotherapy: A ReviewAyu Wita DewiNo ratings yet
- Tugas Individu Ke 1 PDFDocument8 pagesTugas Individu Ke 1 PDFneli rahayuNo ratings yet
- Baru 414.2.full PDFDocument6 pagesBaru 414.2.full PDFIrmagian PaleonNo ratings yet
- MPR-MS (Muscle Spasm) - 1299Document1 pageMPR-MS (Muscle Spasm) - 1299DanielleNo ratings yet
- Coleus Forskohlii and Its Forskolin A ReviewDocument5 pagesColeus Forskohlii and Its Forskolin A ReviewESSENCE - International Journal for Environmental Rehabilitation and ConservaionNo ratings yet
- Vega Remediation Project: September 2020Document5 pagesVega Remediation Project: September 2020Stanescu BogdanNo ratings yet
- Commonrashes in Neonates201205suDocument6 pagesCommonrashes in Neonates201205suDanielcc LeeNo ratings yet
- Changes in The Abdominal Wall After Anterior, Posterior, and Combined Component SeparationDocument11 pagesChanges in The Abdominal Wall After Anterior, Posterior, and Combined Component SeparationsamuelNo ratings yet
- Office Policy UpdatedDocument7 pagesOffice Policy Updatedapi-362969960No ratings yet
- Bio FoldersDocument11 pagesBio Foldersgoksel3173No ratings yet
- Management of Rifampicin-Resistant TB Booklet 1219 v6Document120 pagesManagement of Rifampicin-Resistant TB Booklet 1219 v6DudungNo ratings yet
- Toronto Western Spasmodic Torticollis Rating Scale TWSTRSDocument3 pagesToronto Western Spasmodic Torticollis Rating Scale TWSTRSVioleta López Neciosup0% (1)
- Lesinurad For The Treatment of Hyperuricaemia in People With GoutDocument24 pagesLesinurad For The Treatment of Hyperuricaemia in People With GoutPharmaEducationNo ratings yet
- Buy Crystal Methamphetamine OnlineDocument7 pagesBuy Crystal Methamphetamine Onlinezoe saldana100% (1)
- Orthodontic Treatment of Mandibular Anterior Crowding: Key Words: Crowding, Malocclusion, Labial FlaringDocument4 pagesOrthodontic Treatment of Mandibular Anterior Crowding: Key Words: Crowding, Malocclusion, Labial FlaringDunia Medisku OnlineShopNo ratings yet
- Perbedaan Penanganan Antara Laparoskopi Vs Open Repair Pada Perforasi GasterDocument7 pagesPerbedaan Penanganan Antara Laparoskopi Vs Open Repair Pada Perforasi GasterAfiani JannahNo ratings yet