Download as pdf or txt
You might also like
- Unexpected Joy at Dawn - Docx AnalysisDocument8 pagesUnexpected Joy at Dawn - Docx AnalysisBasil Ekwenye100% (1)
- General Work PermitDocument1 pageGeneral Work PermitJohn Shane100% (5)
- Del Rosario, A - Section B - Exelcise 4Document14 pagesDel Rosario, A - Section B - Exelcise 4ariane galeno100% (1)
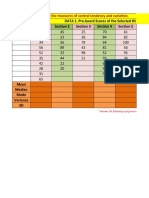
- DATA 1. Pre-Board Scores of The Selected BS Education Students (Per Section) Section 1 Section 2 Section 3 Section 4 Section 5Document10 pagesDATA 1. Pre-Board Scores of The Selected BS Education Students (Per Section) Section 1 Section 2 Section 3 Section 4 Section 5ariane galeno100% (1)
- (Smtebooks - Eu) Coffee Break Python 1st Edition PDFDocument196 pages(Smtebooks - Eu) Coffee Break Python 1st Edition PDFsener.asli100% (9)
- Lionet Lovey: Pattern by Mila Kralina (Ds - Mouse)Document9 pagesLionet Lovey: Pattern by Mila Kralina (Ds - Mouse)Fátima Hunter100% (3)
- JEADV 2022 1782 - Proof - Hi 1Document10 pagesJEADV 2022 1782 - Proof - Hi 1Daniel RodriguezNo ratings yet
- UCU 2105 Fundamentals of Ict Year II Semester IIDocument13 pagesUCU 2105 Fundamentals of Ict Year II Semester IIwawire.14419No ratings yet
- UnknownDocument89 pagesUnknownunggarapunja12No ratings yet
- Tunel staining 量化方法Document22 pagesTunel staining 量化方法ajNo ratings yet
- Biostat Lab Midterm Exam-LUMOSADDocument8 pagesBiostat Lab Midterm Exam-LUMOSADquirenicoleNo ratings yet
- QuestionsDocument2 pagesQuestionsAmaad KhalilNo ratings yet
- Bjo 2023 323884 - Proof - Hi 2Document37 pagesBjo 2023 323884 - Proof - Hi 2Agus LammogliaNo ratings yet
- Traffic Engineering Lab Exercise Report 1&2 Department of Civil Engineering Name:Mekuanint Getnet Entry No: 2018cep2086Document18 pagesTraffic Engineering Lab Exercise Report 1&2 Department of Civil Engineering Name:Mekuanint Getnet Entry No: 2018cep2086Siva EsarapuNo ratings yet
- Anthropometric Profile of Powerlifters: Differences As A Function of Bodyweight Class and Competitive SuccessDocument37 pagesAnthropometric Profile of Powerlifters: Differences As A Function of Bodyweight Class and Competitive Successlucas AyalaNo ratings yet
- Midterm Examination MGT 600 - Statistical Analysis in MGT and EducationDocument3 pagesMidterm Examination MGT 600 - Statistical Analysis in MGT and EducationDona kaitemNo ratings yet
- 2808 Bio Answer KeyDocument1 page2808 Bio Answer KeySohil SharmaNo ratings yet
- Freq. Dist.Document40 pagesFreq. Dist.Web Developer OfficialsNo ratings yet
- 2018 Basal Cell Carcinoma - Part 1Document63 pages2018 Basal Cell Carcinoma - Part 1pablopabloortizortizNo ratings yet
- 2223 g7 Test Results BiagtanDocument29 pages2223 g7 Test Results BiagtanLanna CariñoNo ratings yet
- Statistical Analysis (FINALS Activity)Document3 pagesStatistical Analysis (FINALS Activity)Liel JordNo ratings yet
- Ugc Key 2014Document3 pagesUgc Key 2014Tirumalarao PechettyNo ratings yet
- Statexer#5Document6 pagesStatexer#5Ghost31No ratings yet
- Student - Exam Seating ArrangementDocument7 pagesStudent - Exam Seating Arrangementjslvrz1203No ratings yet
- Analisis Headcount T1-T3Document4 pagesAnalisis Headcount T1-T3David HarrisonNo ratings yet
- Atomic Energy Central School, Indore: Organic Chemistry-Work sheet-IUPAC 1 14Document4 pagesAtomic Energy Central School, Indore: Organic Chemistry-Work sheet-IUPAC 1 14Manoj Kumar SinghNo ratings yet
- QUIZ No.2Document4 pagesQUIZ No.2ariansofia1031No ratings yet
- MutuDocument5 pagesMutudhitadhitNo ratings yet
- 058 - 201983009 - Johan W. LeperteryDocument3 pages058 - 201983009 - Johan W. LeperteryRafael David MaitimuNo ratings yet
- Laporan Praktikum ErgonomiDocument12 pagesLaporan Praktikum ErgonomiErvan Budi SantosoNo ratings yet
- Newell and MacFarlaneDocument5 pagesNewell and MacFarlaneKuan Yau Hoong100% (1)
- (New) Answer Sheet TOEFLDocument8 pages(New) Answer Sheet TOEFLKresna FebriyantoNo ratings yet
- Data Eksekutif Pelayanan Rs Tahun 2009: Rsu. Woodward PaluDocument40 pagesData Eksekutif Pelayanan Rs Tahun 2009: Rsu. Woodward PalufrederickNo ratings yet
- DAVENPORT 2023 ERH-2022 - 0397.R2 - Proof - HiDocument32 pagesDAVENPORT 2023 ERH-2022 - 0397.R2 - Proof - HiTeresa RibaltaNo ratings yet
- 4 Restaurant ServiceDocument15 pages4 Restaurant ServiceAnish KarakNo ratings yet
- Journal Pre-Proof: Journal of The American Academy of DermatologyDocument47 pagesJournal Pre-Proof: Journal of The American Academy of DermatologyM CostantinoNo ratings yet
- PANGILINAN - Biostat MIDTERMDocument8 pagesPANGILINAN - Biostat MIDTERMMira Swan100% (2)
- 2 Helsinki Poster A4 - English - AW - No CropsDocument1 page2 Helsinki Poster A4 - English - AW - No CropsGiovannaNo ratings yet
- Stat 213 Summative Activity 2Document1 pageStat 213 Summative Activity 2gon beeNo ratings yet
- Q2 Math8Document2 pagesQ2 Math8Dhayane RedoquerioNo ratings yet
- BIBLIO DEMATEL NETWORK Using - Combined - Network-Based - ApproachesDocument28 pagesBIBLIO DEMATEL NETWORK Using - Combined - Network-Based - ApproachesEgoitz AstigarragaNo ratings yet
- Midterm Examination MGT 600 - Statistical Analysis in MGT and EducationDocument12 pagesMidterm Examination MGT 600 - Statistical Analysis in MGT and EducationJoseph Mark BaldomarNo ratings yet
- A. Frequency Distribution Table: R Highest Score - Lowest Score R 77 - 31Document3 pagesA. Frequency Distribution Table: R Highest Score - Lowest Score R 77 - 31Juvilyn ManualesNo ratings yet
- BSE181055-Assignment 3Document16 pagesBSE181055-Assignment 3Nabil MunirNo ratings yet
- COMSATS University Islamabad, Wah Campus Terminal Examinations Spring 2020Document6 pagesCOMSATS University Islamabad, Wah Campus Terminal Examinations Spring 2020JUNAID SIALNo ratings yet
- Helsinki Poster A3 English 05 No CropsDocument1 pageHelsinki Poster A3 English 05 No CropsBob MarlaNo ratings yet
- Test 4-8 HalochkaDocument10 pagesTest 4-8 HalochkaKateryna HalochkaNo ratings yet
- Chanakya 301Document1 pageChanakya 301billaaahmedddNo ratings yet
- Summary of Test Results in Grade KTO12 First Quarter Test Subject Teacher Section H.S L.S Range M PL MPS SD No. of CasesDocument6 pagesSummary of Test Results in Grade KTO12 First Quarter Test Subject Teacher Section H.S L.S Range M PL MPS SD No. of CasesRuVinDsbuEndIaNo ratings yet
- 2002 NBDE UnreleasedDocument34 pages2002 NBDE Unreleasedvipul51190No ratings yet
- First Quarter Item Analysis and MPS - T.L.E. (1) MCCCDocument10 pagesFirst Quarter Item Analysis and MPS - T.L.E. (1) MCCCFred FernandoNo ratings yet
- Suggested Homework As6eDocument1 pageSuggested Homework As6ewaleed albashaNo ratings yet
- Assignment II (Sta201)Document2 pagesAssignment II (Sta201)Adeoye Peter AdeolaNo ratings yet
- Bhuvaneshwari,, Gowthaman, Rajmohan)Document6 pagesBhuvaneshwari,, Gowthaman, Rajmohan)baskarNo ratings yet
- Final Exam StatisticsDocument1 pageFinal Exam Statisticsحيدر خالد خلفNo ratings yet
- 8group A (Endoscopic Sinus Surgery With Conventional Endoscopic Instruments)Document4 pages8group A (Endoscopic Sinus Surgery With Conventional Endoscopic Instruments)Waqas KhalilyNo ratings yet
- A New Method To Estimate Weibull Parameter For The Fatigue Life of Self Compacting Fibre Reinforced Concrete BeamsDocument6 pagesA New Method To Estimate Weibull Parameter For The Fatigue Life of Self Compacting Fibre Reinforced Concrete BeamsMr Polash100% (1)
- Bernhard Et Al - 2023 - Leer Con y Sin ComasDocument32 pagesBernhard Et Al - 2023 - Leer Con y Sin ComasMicaela DiNo ratings yet
- Smart Efemena Edu 821 Research and Statistics Assignment 02 - 2020.11.30Document5 pagesSmart Efemena Edu 821 Research and Statistics Assignment 02 - 2020.11.30CelestineNo ratings yet
- Kunci Jawaban UKDI Clinic 2 Batch Feb 2016Document1 pageKunci Jawaban UKDI Clinic 2 Batch Feb 2016Kholisah MardiyahNo ratings yet
- SolutionDocument5 pagesSolutionPhi Vũ ĐăngNo ratings yet
- Dermatology Essentials 2Nd Edition Jean L Bolognia Full ChapterDocument51 pagesDermatology Essentials 2Nd Edition Jean L Bolognia Full Chaptermadge.ortiz938100% (6)
- Zingerman's Sep-Oct 2023 NewsletterDocument9 pagesZingerman's Sep-Oct 2023 NewsletterZingerman's Community of BusinessesNo ratings yet
- Die Bosch ABS The World's First System For Closed-Loop Control of Vehicle DynamicsDocument27 pagesDie Bosch ABS The World's First System For Closed-Loop Control of Vehicle DynamicsMamdouhAlhanafy100% (1)
- PO-Flat 201 PDFDocument12 pagesPO-Flat 201 PDFHusain MohammadNo ratings yet
- MCQ On Rural MarketingDocument28 pagesMCQ On Rural Marketingjaitripathi26No ratings yet
- Trainers Qualifications - Job Roles WiseDocument264 pagesTrainers Qualifications - Job Roles WiseJagdish RajanNo ratings yet
- Verbal and Nonverbal Communication and Their Functions-3 - Group 42 GE-PC - PURPOSIVE COMMUNICATIONDocument6 pagesVerbal and Nonverbal Communication and Their Functions-3 - Group 42 GE-PC - PURPOSIVE COMMUNICATIONLowell James TigueloNo ratings yet
- Dokumen 2Document1 pageDokumen 2Balamurugan HNo ratings yet
- LP 1 Music Q3Document4 pagesLP 1 Music Q3Hazel Rubas SamsonNo ratings yet
- SPHE1003Ax PDFDocument29 pagesSPHE1003Ax PDFGuillermito PelosiNo ratings yet
- (David de Las Morenas) The Book of Alpha - 30 RulesDocument151 pages(David de Las Morenas) The Book of Alpha - 30 RulesRd man80% (5)
- Perl BooksDocument3 pagesPerl Booksamar.ramdhave8199No ratings yet
- CS401 PPTDocument193 pagesCS401 PPTMuqadas ZahraNo ratings yet
- HUBBELL INC 10-K (Annual Reports) 2009-02-20Document90 pagesHUBBELL INC 10-K (Annual Reports) 2009-02-20http://secwatch.comNo ratings yet
- Data Sheet 6ED1052-1MD08-0BA0: DisplayDocument2 pagesData Sheet 6ED1052-1MD08-0BA0: DisplayessameldinNo ratings yet
- Case study-Connaught-PlaceDocument31 pagesCase study-Connaught-PlaceSwetha Ashok100% (2)
- Traditional Tamil CropsDocument4 pagesTraditional Tamil CropsRahul KumarNo ratings yet
- Lesson PlanDocument5 pagesLesson Planapi-239291032No ratings yet
- Glenda Gloria Media in The PhilippinesDocument6 pagesGlenda Gloria Media in The PhilippinesHappy Jayson Mondragon100% (1)
- SNR Supply DemandDocument10 pagesSNR Supply DemandFitzNo ratings yet
- The Official Bulletin: 2011 Q2 / No. 632Document30 pagesThe Official Bulletin: 2011 Q2 / No. 632IATSENo ratings yet
- Fort Dansborg DetailsDocument16 pagesFort Dansborg Detailsabdul rahmanNo ratings yet
- Key Issues ReflectionDocument7 pagesKey Issues ReflectionLee SuarezNo ratings yet
- C ContentsDocument3 pagesC Contentsearle akhilNo ratings yet
- Experiment - 1: Batch (Differential) Distillation: 1. ObjectiveDocument29 pagesExperiment - 1: Batch (Differential) Distillation: 1. ObjectiveSwayamjeet SwainNo ratings yet
- CIBIL Consent FormDocument4 pagesCIBIL Consent FormKuldeep BatraNo ratings yet
- Operator'S Manual: Crawler ExcavatorDocument322 pagesOperator'S Manual: Crawler ExcavatorAlain DefoeNo ratings yet