Download as pdf or txt
You might also like
- Guideline Watch 2021Document24 pagesGuideline Watch 2021Pedro NicolatoNo ratings yet
- Person-Centred Care and Naturopathy: Patient Beliefs and ValuesDocument15 pagesPerson-Centred Care and Naturopathy: Patient Beliefs and Valuesromantictroupe314No ratings yet
- Continuing EducationDocument9 pagesContinuing EducationAnitha sujithNo ratings yet
- Telaah Jurnal METPENDocument16 pagesTelaah Jurnal METPENaida fahleviNo ratings yet
- Health Care Provider and Patient Preparedness ForDocument10 pagesHealth Care Provider and Patient Preparedness ForTJ LapuzNo ratings yet
- BJGPO.2023.0179.fullDocument23 pagesBJGPO.2023.0179.fullRISHIKA GUPTANo ratings yet
- Velasquezreyes 2017Document11 pagesVelasquezreyes 2017Margarida ReisNo ratings yet
- Atow 502 00Document9 pagesAtow 502 00hnzzn2bymdNo ratings yet
- Positive Effect of Care Bundles On Patients With Central Venous Catheter Insertions at A Tertiary Hospital in Beijing, ChinaDocument10 pagesPositive Effect of Care Bundles On Patients With Central Venous Catheter Insertions at A Tertiary Hospital in Beijing, ChinaElfina NataliaNo ratings yet
- s13643 022 02135 8 PDFDocument9 pagess13643 022 02135 8 PDFdeaalifiahNo ratings yet
- Clinical Research and Medical CareDocument7 pagesClinical Research and Medical CareNino MdinaradzeNo ratings yet
- Journal Pone 0294218Document10 pagesJournal Pone 0294218bronson.harryNo ratings yet
- Nurse-Led Adherence Support in Hypertension: A Randomized Controlled TrialDocument8 pagesNurse-Led Adherence Support in Hypertension: A Randomized Controlled TrialIndah SundariNo ratings yet
- Strategies To Prevent Central Line Associated Bloodstream Infections in Acute Care Hospitals 2022 UpdateDocument17 pagesStrategies To Prevent Central Line Associated Bloodstream Infections in Acute Care Hospitals 2022 Updatealejandro montesNo ratings yet
- ArticleDocument9 pagesArticleAna Lazar IvanNo ratings yet
- Hospital-Based ACT Intervention To Improve Retention in Care For Persons With HIV - 2021Document18 pagesHospital-Based ACT Intervention To Improve Retention in Care For Persons With HIV - 2021Ashik RahamanNo ratings yet
- The Integral Role of The Clinical Pharmacist Practitioner in Primary CareDocument5 pagesThe Integral Role of The Clinical Pharmacist Practitioner in Primary CareRirin AptNo ratings yet
- Self-Management Interventions For Chronic Kidney Disease: A Systematic Review and Meta-AnalysisDocument13 pagesSelf-Management Interventions For Chronic Kidney Disease: A Systematic Review and Meta-AnalysisKikimariaNo ratings yet
- Improving End of Life CareDocument9 pagesImproving End of Life CareM_LXNo ratings yet
- Woolf. 1999. Potential Benefits, Limitations, and Harms of Clinical GuidelinesDocument4 pagesWoolf. 1999. Potential Benefits, Limitations, and Harms of Clinical Guidelinestonghieu96No ratings yet
- Phytotherapy and Nutritional Supplements On Breast CancerDocument42 pagesPhytotherapy and Nutritional Supplements On Breast CancerGabrielAbarcaNo ratings yet
- Development of A Clinical Practice Guideline For PDocument11 pagesDevelopment of A Clinical Practice Guideline For P5mcj2yjmqpNo ratings yet
- Freidin, O'Hare, Wong - 2019 - Person-Centered Care For Older Adults With Kidney Disease Core Curriculum 2019Document10 pagesFreidin, O'Hare, Wong - 2019 - Person-Centered Care For Older Adults With Kidney Disease Core Curriculum 2019Ro RojasNo ratings yet
- Laude 2020Document9 pagesLaude 2020Heryanti PusparisaNo ratings yet
- Bahan 2-DikonversiDocument11 pagesBahan 2-DikonversiMaya ismayaNo ratings yet
- Towards Patient-Centered Care For People Living With Kidney DiseaseDocument8 pagesTowards Patient-Centered Care For People Living With Kidney DiseaseEva RetniNo ratings yet
- NAv y No Asociada SHEA 2022Document27 pagesNAv y No Asociada SHEA 2022link0105No ratings yet
- Discharge Planning For Acute Coronary Syndrome Patients in A Tertiary Hospital: A Best Practice Implementation ProjectDocument17 pagesDischarge Planning For Acute Coronary Syndrome Patients in A Tertiary Hospital: A Best Practice Implementation ProjectMukhlis HasNo ratings yet
- Surviving Sepsis: Going Beyond The Guidelines: Review Open AccessDocument6 pagesSurviving Sepsis: Going Beyond The Guidelines: Review Open AccessTasya Arsy LiyanaNo ratings yet
- MoroccanDocument8 pagesMoroccanWijdane El YoumniNo ratings yet
- Critical Care After Major Surgery A Systematic Review of Risk Factors Unplanned Admission - Onwochei UK 2020Document13 pagesCritical Care After Major Surgery A Systematic Review of Risk Factors Unplanned Admission - Onwochei UK 2020Fransisca Dewi KumalaNo ratings yet
- MousaDocument12 pagesMousaGiriNo ratings yet
- s12916 022 02508 9Document17 pagess12916 022 02508 9Akarapon SugandhanandaNo ratings yet
- Multicentre Analysis CancerDocument8 pagesMulticentre Analysis Cancersilvio da costa guerreiroNo ratings yet
- Acupuncture in Cancer Care Recommendations For SafDocument17 pagesAcupuncture in Cancer Care Recommendations For Safviventius yoshuaNo ratings yet
- Supportive Care: Integration of Patient-Centered Kidney Care To Manage Symptoms and Geriatric SyndromesDocument10 pagesSupportive Care: Integration of Patient-Centered Kidney Care To Manage Symptoms and Geriatric Syndromesyanuar esthoNo ratings yet
- Occurrence and Outcome of Delirium in Medical In-Patients: A Systematic Literature ReviewDocument15 pagesOccurrence and Outcome of Delirium in Medical In-Patients: A Systematic Literature ReviewJoao CabralNo ratings yet
- Effectiveness and Safety of Drugs For Obesity BMJDocument17 pagesEffectiveness and Safety of Drugs For Obesity BMJtheriversongsNo ratings yet
- Ojn2024145 11442219Document6 pagesOjn2024145 11442219AFURANTANo ratings yet
- Costs and Effectiveness of Pharmacist-Led Group Medical Visits For Type-2 Diabetes: A Multi-Center Randomized Controlled TrialDocument14 pagesCosts and Effectiveness of Pharmacist-Led Group Medical Visits For Type-2 Diabetes: A Multi-Center Randomized Controlled TrialLised MillanNo ratings yet
- Tpja31 2Document8 pagesTpja31 2Kirubel TesfayeNo ratings yet
- Self-Monitoring of Blood Pressure Among Women With Hypertensive Disorders of Pregnancy - A SYSTEMATIC REVIEWDocument16 pagesSelf-Monitoring of Blood Pressure Among Women With Hypertensive Disorders of Pregnancy - A SYSTEMATIC REVIEWWeslley FerreiraNo ratings yet
- Patient-Reported Outcome Measures and Health Informatics.: ArticleDocument24 pagesPatient-Reported Outcome Measures and Health Informatics.: ArticleValerie LascauxNo ratings yet
- Nejmoa 2303966Document11 pagesNejmoa 2303966Raul ForjanNo ratings yet
- 2 PBDocument19 pages2 PBPralhad TalavanekarNo ratings yet
- Tmi 13078Document10 pagesTmi 13078Husni FaridNo ratings yet
- Oncología IntegrativaDocument9 pagesOncología IntegrativaYuli MSNo ratings yet
- Clinical Effect of Catgut Implantation at AcupointsDocument8 pagesClinical Effect of Catgut Implantation at AcupointsJuan Pablo MejíaNo ratings yet
- 00014Document6 pages00014Paulo VictorNo ratings yet
- Ospital Ccreditation Reflection ON Health Care Quality ManagementDocument9 pagesOspital Ccreditation Reflection ON Health Care Quality ManagementKaran BabaNo ratings yet
- Conservative Management in CKDDocument11 pagesConservative Management in CKDSa7arNo ratings yet
- Asian Nursing ResearchDocument6 pagesAsian Nursing ResearchMohRozaniNo ratings yet
- 63 2023 Article 1028Document5 pages63 2023 Article 1028Ahmad FahroziNo ratings yet
- 2024 Article 1348Document13 pages2024 Article 1348MalfathbpNo ratings yet
- JurnalDocument9 pagesJurnalFitriatun NisaNo ratings yet
- Blood Borne Pathogens PolicyDocument8 pagesBlood Borne Pathogens PolicyChris KristoffersonNo ratings yet
- Knowledge, Attitude, Confidence, and Educational Needs of Palliative Care in Nurses Caring For Non-Cancer Patients: A Cross-Sectional, Descriptive StudyDocument14 pagesKnowledge, Attitude, Confidence, and Educational Needs of Palliative Care in Nurses Caring For Non-Cancer Patients: A Cross-Sectional, Descriptive StudyRahmanu ReztaputraNo ratings yet
- Review JurnalDocument23 pagesReview JurnalStela tumundoNo ratings yet
- 3474 J2e1xaDocument8 pages3474 J2e1xaArslan KhanNo ratings yet
- Advances in Managing Fistulizing Crohn’s Disease: A Multidisciplinary ApproachFrom EverandAdvances in Managing Fistulizing Crohn’s Disease: A Multidisciplinary ApproachNo ratings yet
- Palliativecarein Gynecologiconcology: Mary M. Mullen,, James C. Cripe,, Premal H. ThakerDocument19 pagesPalliativecarein Gynecologiconcology: Mary M. Mullen,, James C. Cripe,, Premal H. ThakerNita AgarwalNo ratings yet
- The Use of Multivariate Statistical Methods For Optimization of The Surface Water Quality Network Monitoring in The Paraopeba River Basin, BrazilDocument17 pagesThe Use of Multivariate Statistical Methods For Optimization of The Surface Water Quality Network Monitoring in The Paraopeba River Basin, BrazilAna Carolina NevesNo ratings yet
- CHN1 Worksheet1Document5 pagesCHN1 Worksheet1Chariza MayNo ratings yet
- Barangay Nutrition Profile or Situation Analysis 1Document2 pagesBarangay Nutrition Profile or Situation Analysis 1ann29No ratings yet
- Module 5 Lec 3Document17 pagesModule 5 Lec 3Shivang DhoundiyalNo ratings yet
- Zone 2 WorkshopDocument58 pagesZone 2 Workshoprehaangulati2009No ratings yet
- Learning Activity Sheet Quarter 2 - MELC 2: Discipline and Ideas in Applied Social SciencesDocument4 pagesLearning Activity Sheet Quarter 2 - MELC 2: Discipline and Ideas in Applied Social Sciencesgayle gallaza100% (1)
- Pengaruh Hemolisis Terhadap Nilai Trombosit Dengan Menggunakan Metode Direct CountingDocument6 pagesPengaruh Hemolisis Terhadap Nilai Trombosit Dengan Menggunakan Metode Direct CountingyudhaNo ratings yet
- PART-2017-551038V1 - MDR CodesDocument11 pagesPART-2017-551038V1 - MDR CodesFranciscoNo ratings yet
- A. B. C. D. A. B. C. D.: Thời gian làm bài: 60 phút, không kể thời gian phát đềDocument4 pagesA. B. C. D. A. B. C. D.: Thời gian làm bài: 60 phút, không kể thời gian phát đềTruong Thi Ha Trang 1KT-19No ratings yet
- The Fault in Our Stars-Extract 1-2 QuestionsDocument6 pagesThe Fault in Our Stars-Extract 1-2 QuestionsNathaly Yessenia Luque CruzNo ratings yet
- English 7 q1 m7 EditedDocument11 pagesEnglish 7 q1 m7 EditedShei La Ma RieNo ratings yet
- San Francisco Parish School: Pauna ST., Del Remedio, Cardona, RizalDocument1 pageSan Francisco Parish School: Pauna ST., Del Remedio, Cardona, RizalTek CasoneteNo ratings yet
- New Era of Filipino Youth VolunteerismDocument11 pagesNew Era of Filipino Youth VolunteerismArvhie Santos100% (1)
- Role of Saliva in Dental CariesDocument29 pagesRole of Saliva in Dental Carieskhush sidhu100% (1)
- Abdominal Acupuncture For DepressionDocument35 pagesAbdominal Acupuncture For DepressionAGNESE YOLOTZIN OLIVERA TORO REYESNo ratings yet
- Shampoo BarDocument1 pageShampoo BarrezaNo ratings yet
- Yokoyama Et Al. C-BED Hikikomori SupportDocument10 pagesYokoyama Et Al. C-BED Hikikomori SupportKayu LowNo ratings yet
- Topic 1.4 - User-Requirement and Perception of SpaceDocument8 pagesTopic 1.4 - User-Requirement and Perception of SpaceCarlo PascuaNo ratings yet
- ZEBRA Pen SDS R 301Document6 pagesZEBRA Pen SDS R 301chusqueteNo ratings yet
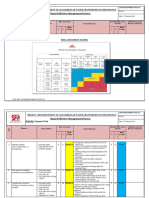
- RISK ASSESSMENT - Carpentry WorkDocument6 pagesRISK ASSESSMENT - Carpentry WorkbalajiNo ratings yet
- Learning Objective: Book 2 English For Professional NurseDocument3 pagesLearning Objective: Book 2 English For Professional NurseLestari RahayuNo ratings yet
- Els 205Document2 pagesEls 205KING JaMEsNo ratings yet
- Primary Health CareDocument17 pagesPrimary Health CareKevins ChepsirNo ratings yet
- 07 One Missing StrokeDocument10 pages07 One Missing StrokeMiura AngNo ratings yet
- Group Name 2 English ClubDocument10 pagesGroup Name 2 English ClubWill HensNo ratings yet
- Patient SatisfactionDocument6 pagesPatient SatisfactionDon Chiaw ManongdoNo ratings yet
- Vision: WWW - Visionias.inDocument18 pagesVision: WWW - Visionias.inamitNo ratings yet
- Topic 1. Parents Are Too Permissive With Their Children NowadaysDocument26 pagesTopic 1. Parents Are Too Permissive With Their Children NowadaysBùi Thanh Ngọc BíchNo ratings yet
- Sex Differences in Valgus Knee Angle During A Single-Leg Drop JumpDocument6 pagesSex Differences in Valgus Knee Angle During A Single-Leg Drop JumpfaridNo ratings yet