Volume 9, Issue 6, June – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24JUN156
Liver Abscess Caused by Foreign Body
Dr. Deepak Kumar Nayak (Post Graduate Trainee);
Dr. L. K. Dash (Head of Department Professor);
Dr. Sandhya Shukla (Professor);
Dr. B. Samantaray (Associate Professor)
Department of General Medicine , Hi-Tech Medical College & Hospital Bhubaneswar, ODISHA , INDIA
Abstract:- A rare case of liver abscess due to secondary complains of pain in the right upper abdomen for 10 days,
bacterial infection due to foreign body penetration into which is dull aching in nature, radiates to right to shoulder
stomach wall reported in this case. Presented with less ,associated with nausea, dry cough most of time nocturnal
severe clinical features and non-specific features of acute with high grade fever, last for two to four hour, pain is more
abdomen .Liver abscess caused by foreign body is rare. marked & gradually increasing in severity when lying in
The contrast-enhanced CT (computed tomography)of right lateral position . Also marked weight loss , loss of
the abdomen and the minimally invasive abdominal appetite(unable to take full size meal as earlier) and malaise.
operation both played critical roles in the diagnosis and After careful & thorough history it came to know that he had
treatment of the case. The general population, who eaten fish with excessive alcohol in last marriage party .
mistakenly eat fish bones, should seek medical treatment
as soon as possible. Past Illness
No history of T2DM or Hypertension . No relevant
I. INTRODUCTION surgical history.
A liver abscess is defined as pus in liver that can Personal History
develop from injury to the liver or an intra-abdominal Tobbaco chewing for 20 years. Taking alcohol for
infection disseminated from the portal circulation.[1] These 10years . He belongs to average socio-economic status .
abscesses categorized into pyogenic(mostly polymicrobial, Married at age 27 yrs having 2 children. On Mixed Indian
but some common organisms such as E.coli, Klebsiella, Diet.His bladder and bowel habits are normal.
Streptococcus, Staphylococcus, and anaerobes) or amoebic(
mostly Entamoeba histolytica), in minority cases caused by General Examination–
parasites (hydatid cyst)and fungi. Location in liver ,around BP – 130/90 mmHg, Pulse 102/Min, Temp – 102 F,
50% of solitary liver abscesses occur in the right lobe of the SpO2- 98% at Room Air, Respiration Rate – 20/Min, GCS-
liver (becouse of more blood supply), less commonly in the 15/15(E4 V5 M6).
left liver lobe or caudate lobe. In rare cases foreign bodies
in the digestive tract generally caused by mistaken Patient is Conscious but Lethargic and irritated. Patient
consumption of different types of foreign bodies like fish has mild pallor with epigastric & right hypochondrium
bone ,chicken bone ,tooth picks ,safety pins and coins. fullness, tender Hepatomegaly. There are no features of
Those foreign bodies eliminated smoothly from digestive shifting dullness, engorged veins, oedema,
tract without any mal-adaptation normally. lymphadenopathy, clubbing ,raised JVP and cyanosis .
II. CASE REPORT Course In Hospitalization–
Patient was transferred to ward and treated with
A 53 year old male patient came to our Medicine OPD PRBC( packed red blood corpuscles) , Broad spectrum Anti-
with complains of – Biotics, anti-luminal, antipyretics and other Supportive
Fever for 1month drugs.
Loss of appetite 20 days.
Pain abdomen for 10 days Investigations
Laboratory investigation below showing anemia,
History of Present Illness leukocytosis, elevated alkaline phosphatase. Mostly
Patient was apparently alright 1 month back, to start improved after mangement.
with he developed intermittent high grade fever, highest
recorded temperature is 104ºF most of time in evening after
dinner. Fever is associated with chills and rigor, subsides
only after taking antipyretic & cold sponging. He also
IJISRT24JUN156 www.ijisrt.com 1041
Volume 9, Issue 6, June – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24JUN156
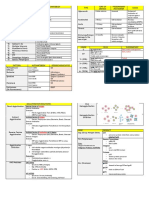
Table 1 Investigations
PARAMETERS ADMISSION DAY DAY 3 OF POST -OP ON DISCHARGE
HOSPITALIZATION SURGERY
TLC 99610/UL 89640/UL 41790/UL 31760/UL
RBC COUNT - 2.37million/cumm 2.94million/cumm 2.89million/cumm 3.89million/cumm
HB% 6.7 gm% 10.2 gm% 9.1gm% 13.9gm%
PCV 25.9 vol% 24.7 vol% 23.7 vol% 24.7 vol%
MCV 115.6 fl 94.9fl 83.7.9fl 83.7.9fl
TPC 173000 189000 260000 260000
RDW-SD 56.7 fl 55.9fl 54.9fl 57.9fl
NEUTROPHIL 84.4% 78.4% 75.4% 71.4%
LYMPHOCYTE 30.7% 32.3% 12.3% 9.3%
MONOCYTES 4.0% 2.9% 3.9% 2.9%
EOSINOPHILS 0.5% 0.3% 0.1% 0.0%
BASOPHILS 0.4% 0.3% 0.3% 0.1%
CRP 50.5 mg/dl 50.5 mg/dl 30.9mg/dl 10.5 mg/dl
ESR 140 28
S. IRON 133 microgram/dl
LDH 2412 IU/L
UREA 19 mg/dl
CREATININE 1.11 mg/dl
SODIUM 135.7 mmol/l
POTASSIUM 4.59 mmol/l
URIC ACID 5.1 mg/dl
CHLORIDE 105 mmol/L
CALCIUM 7.0 mg/dl
PHOSPHORUS 3.9 mg/dl
TOTAL 0.58 mg/dl 0.38 mg/dl
BILIRUBIN
DIRECT 0.86 mg/dl 0.51 mg/dl
BILIRUBIN
ALT 43.7 U/L 40.7 U/L
AST 50.6 U/L 54.6 U/L
ALP 135 U/L 115 U/L
TOTAL PROTEIN 6.9 gm/dl 5.9 gm/dl
ALBUMIN 3.2 gm/dl 3.1 gm/dl
GLOBULIN 3.7 gm/dl 3.6 gm/dl
A/G RATIO 0.86 0.86
T3 1.39
T4 9.7
TSH 1.663
PT 13.5 sec 13.6 Sec 13.86 Sec
INR 1.93 1.86 1.76
APTT 31.8 32.3 31.8
Hepatitis & HIV Panel – Negative.
USG Abdomen – liver abscess in left lobe , mild Hepatomegaly.
CHEST X-RAY – RIGHT HEMI-DIAPHRAGM
CECT ABDOMEN – multiple inter-communicating liver abscess in segment
II & III, thin curvilinear foreign body in left sub-hepatic region abutting
antro-pyloric region of stomach with other end in segment III.
IJISRT24JUN156 www.ijisrt.com 1042
Volume 9, Issue 6, June – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24JUN156
X-Ray Chest PA View
Below Figure 1- X-ray chest postero anterior view below showing right hemi-diaphragm in suspicious about liver
pathology.
Fig-1 X-Ray Chest PA View
Fig 2 CECT Abdomen
Above Figure 2- Contrast enhanced CT (computed III. TREATMENT / MANAGEMENT
tomography)scan showing multiple inter-communicating
liver abscess in segment II & III, thin curvilinear foreign Managed with Empirical antibiotic for coverage of
body in left sub-hepatic region abutting antro-pyloric region anaerobes, entamoeba histolytica ,entero-bacteriaceae,
of stomach with other end in segment III. streptococci & enterococci. Such antibiotic regimens include
IJISRT24JUN156 www.ijisrt.com 1043
Volume 9, Issue 6, June – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24JUN156
Beta-Lactamase inhibitor with metronidazole ,the fever get Exploratory Laparotomy
decreased. Below figure 3 showing hepatic resection of lobe (seg
II & III ) with liver abscess drainage & foreign body ( two
fish bone length 3.2 & 1.8 cm ) extracted and repair of
gastric perforation at antro-pyloric region of stomach.
Fig 3 Respected Part of Left Lateral Segment having Multiloculated Abscess & Two Fish Bone Length 3.2 & 1.8 cm
IV. DISCUSSION Perforation commonly seen in stomach lesser
curvature because of the anatomical acute angularity with
Bacterial liver abscesses are common clinical abscess most commonly developing in left hepatic lobe,
infectious disease of the liver and mostly presented with because of its proximity with stomach lesser curvature.
fever, chill, and pain abdomen. But some cases presented
with non-specific clinical features. Foreign body width larger than 2 to 2.5cm,can’t get
through the pylori and longer than 5 to 6cm,cannot pass
Liver abscess mainly caused by bacterial invasion through the duodenum preventing from being discharged
through three routes ( hepatic arteries, billiary tracts and out of digestive tract.
portal veins) . In comparison, the liver abscess that resulted
from the penetration of foreign bodies through the stomach The classic clinical features of hepatic abscess like fever,
wall after entering the digestive tracts is rarely seen in the abdominal pain, and jaundice is usually not seen, most
clinical practice. patients have vague symptoms such as anorexia, and
vomiting with leukocytosis, deranged liver function test,
Foreign bodies usually get impacted at the esophageal making the diagnosis more difficult without definitive
sphincters, pyloric canal, duodenum, ileocaecal valve, and history of fish bone ingestion.
anus due to extrinsic impression or anatomical narrowing.
Perforations are more common in the oesophagus causing Bacterial flora seen in the oral-cavity commonly found
pneumo-mediastinum, retropharyngeal abscess, mediastinal in abscess cultures.[2,5]
abscess, and bleeding.3 Normally, 80% to 90% of the
foreign bodies in the digestive tract can be eliminated by Small abscess (less than 5 cm) treated with antibiotics.
gastric acid, anti-bacterial gastric juice & inflamatory action Larger abscess(more than 5cm) with multi-loculations
without any mal-adaptation. Beyond the esophagus treated with surgery, draining of the abscess, and removal of
perforation and complications are rare. the foreign body.
However 1% of the fish bones are sufficiently large or V. CONCLUSION
hard (like fish spine bone)that cannot be digested by gastric
juice or pass through, due to pyloric stenosis or narrow In conclusion, Secondary liver abscess, unlike other
space, the sharp fish bone is most likely to penetrate the liver abscess, due to foreign body requires urgent
stomach wall due to the rapid contraction of the stomach reasonable and therapeutic regimen according to the
during peristalsis. medical history ,laboratory examination and imaging
manifestation.
IJISRT24JUN156 www.ijisrt.com 1044
Volume 9, Issue 6, June – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24JUN156
The patients with mistaken fish bone ingestion
complications presents with nonspecific features of acute
abdomen. The clinical diagnosis is difficult without a
definitive history of fish bone ingestion. The CT (computed
tomography) scan localize the ingested fish bone for proper
timely treatment and provide comprehensive evaluation of
the complications of fish bone ingestion including hepatic
abscess. [3,5]
REFERENCES
[1]. Mischnik A, Kern WV, Thimme R. [Pyogenic liver
abscess: Changes of Organisms and
[2]. Consequences for Diagnosis and Therapy]. Dtsch Med
Wochenschr. 2017 Jul;142(14):1067-1074.[PubMed:
28728202]
[3]. Czerwonko ME, Huespe P, Bertone S, Pellegrini P,
Mazza O, Pekolj J, de Santibañes E, Hyon SH, de
Santibañes M. Pyogenic liver abscess: current status
and predictive factors for recurrence and mortality of
first episodes. HPB (Oxford). 2016 Dec;18(12):1023-
1030. [PMC free article:PMC5144545] [PubMed:
27712972]
[4]. Goh BK, Tan YM, Lin SE, Chow PK, Cheah FK, Ooi
LL, et al. CT in the preoperative diagnosis of fish bone
perforation of the gastrointestinal tract. AJR Am J
Roentgenol 2006; 187: 710-144.
[5]. de la Vega M, Rivero JC, Ruiz L, Suarez S. A fish
bone in the liver. Lancet 2001; 358: 982.
[6]. Bathla G, Teo LL, Dhanda S. Pictorial essay:
Complications of a swallowed fish bone. Indian J
Radiol Imaging 2011; 21: 63-68.
[7]. Masoodi I, Alsayari K, Al Mohaimeed K, Ahmad S,
Almtawa A, Alomair A, et al. Fish bone migration: an
unusual cause of liver abscess. BMJ Case Rep 2012;
pii: bcr0920114838.
[8]. Kessler AT, Kourtis AP. Images in clinical medicine.
Liver abscess due to Eikenella corrodens from a
fishbone. N Engl J Med 2001; 345: e5.
IJISRT24JUN156 www.ijisrt.com 1045
You might also like
- The Complete Family Guide To SchizophreniaDocument497 pagesThe Complete Family Guide To Schizophreniaaganayan100% (1)
- 03 PsoriasisDocument28 pages03 PsoriasisGlen Lester ChiongNo ratings yet
- Subclinical Hypothyroidism TDocument6 pagesSubclinical Hypothyroidism TAnisa Iswari Pombaile-NgurawanNo ratings yet
- Gastric UlcerDocument13 pagesGastric UlcerAnis IzzatiNo ratings yet
- Case 056: Common Bile Duct Stones (Choledocholithiasis)Document5 pagesCase 056: Common Bile Duct Stones (Choledocholithiasis)ZauzaNo ratings yet
- Ayurvedic Management of Ulcerative Colitis W.S.R To Grahni Dusti-A Case StudyDocument6 pagesAyurvedic Management of Ulcerative Colitis W.S.R To Grahni Dusti-A Case StudyDrHassan Ahmed ShaikhNo ratings yet
- Cheza May B. Baldado: Year and Section: BS Pharmacy III - ADocument3 pagesCheza May B. Baldado: Year and Section: BS Pharmacy III - AKathleen B BaldadoNo ratings yet
- Liver, Pancreas and Biliary Tract Problems: Case StudyDocument62 pagesLiver, Pancreas and Biliary Tract Problems: Case StudyElaine Frances IlloNo ratings yet
- Kasus - I Wayan Aryanta PutraDocument20 pagesKasus - I Wayan Aryanta PutraDiana BaagilNo ratings yet
- Case Study 39-Year-Old Women Diagnosed As Solitary Rectal Ulcer SyndromeDocument5 pagesCase Study 39-Year-Old Women Diagnosed As Solitary Rectal Ulcer SyndromeInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Appendicitis Hidden Under The Facade of Addison's Crisis: A Case ReportDocument2 pagesAppendicitis Hidden Under The Facade of Addison's Crisis: A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cholycystectomy FinalDocument53 pagesCholycystectomy FinalCharmie GandaNo ratings yet
- MR - 20 Okt TB Putus ObatDocument60 pagesMR - 20 Okt TB Putus ObatAnna LiveNo ratings yet
- Case1 - Pernicious AnemiaDocument35 pagesCase1 - Pernicious AnemiaRyan ArcuenoNo ratings yet
- Case Presentation On Chronic Liver Disease: Shreyas M Salimath Pharm D 2 Year REG NO. 21Q0172Document18 pagesCase Presentation On Chronic Liver Disease: Shreyas M Salimath Pharm D 2 Year REG NO. 21Q0172AmalinNo ratings yet
- AGE + DyselectrolytemiaDocument20 pagesAGE + DyselectrolytemiaMhd AloofNo ratings yet
- GE BasavaDocument21 pagesGE BasavaAmalin PrãdhãñNo ratings yet
- Latihan POMR: Dr. Venna Febrian KDocument39 pagesLatihan POMR: Dr. Venna Febrian KLoudry ElfaNo ratings yet
- NC Rara HemaDocument18 pagesNC Rara HemaDodi DiNo ratings yet
- Revised Janna Medical WardDocument5 pagesRevised Janna Medical Wardjanna mae patriarcaNo ratings yet
- Gross Painless Hematuria Bladder Irritability With Dysuria Frequency UrgencyDocument15 pagesGross Painless Hematuria Bladder Irritability With Dysuria Frequency UrgencyBrett FisherNo ratings yet
- Case Presentation RVFDocument15 pagesCase Presentation RVFMeena Koushal100% (1)
- Autoimmune Thyroid Disease CompleteDocument103 pagesAutoimmune Thyroid Disease Completeseun williamsNo ratings yet
- NC LidaDocument19 pagesNC LidaDodi DiNo ratings yet
- Ibdcase 180706145428 PDFDocument15 pagesIbdcase 180706145428 PDFakashNo ratings yet
- AppendectomyDocument22 pagesAppendectomyTimothy WilliamsNo ratings yet
- AGE + DyselectrolytemialoofDocument20 pagesAGE + DyselectrolytemialoofMhd AloofNo ratings yet
- Morning ReportDocument27 pagesMorning ReportDody PrasetyaNo ratings yet
- Schiavo Et Al-2015-Clinical Case ReportsDocument5 pagesSchiavo Et Al-2015-Clinical Case ReportsvictorNo ratings yet
- MR Kasa Hydropneumothorax EditedDocument17 pagesMR Kasa Hydropneumothorax Editedazraeni_629166196No ratings yet
- c-7 Case PresentatonDocument11 pagesc-7 Case PresentatonRaja0% (1)
- Clinical Confrence: Hemato Onkologi Division (Death Case)Document26 pagesClinical Confrence: Hemato Onkologi Division (Death Case)Sukma SusantiNo ratings yet
- Hypertensive Coronary Artery Disease Post Coronary Artery Bypass Grafting - Critical CareDocument28 pagesHypertensive Coronary Artery Disease Post Coronary Artery Bypass Grafting - Critical CareAdolf Benedick Dacanay MalalaNo ratings yet
- TMP 15Document38 pagesTMP 15FrontiersNo ratings yet
- BA With UTIDocument20 pagesBA With UTIJyothsna JoyNo ratings yet
- Rahmatia Efusi PleuraDocument14 pagesRahmatia Efusi PleuraJuli2022 Semnol-SemsaNo ratings yet
- Case Presentation: Presented By: DR Osama Shabbir Supervised By: DR Pahlaj KolhiDocument34 pagesCase Presentation: Presented By: DR Osama Shabbir Supervised By: DR Pahlaj KolhimehwishNo ratings yet
- NC Haikal OleDocument22 pagesNC Haikal OleIla MumtazahNo ratings yet
- PancreatitisDocument59 pagesPancreatitisAarif RanaNo ratings yet
- GHHH HHHH HHHH K SssDocument4 pagesGHHH HHHH HHHH K SssgabriellcvieiraNo ratings yet
- 11-Surgery Intervention in GEH DisordersDocument55 pages11-Surgery Intervention in GEH DisordersnadiaNo ratings yet
- Acute Mushroom Poisoning. Facebook Saves Lifes!: Mihai Popescu, MD, PHDDocument60 pagesAcute Mushroom Poisoning. Facebook Saves Lifes!: Mihai Popescu, MD, PHDMihai PopescuNo ratings yet
- Peritonitis in PD PatientsDocument64 pagesPeritonitis in PD PatientsDaniel SitungkirNo ratings yet
- 2 AppendicitisDocument9 pages2 AppendicitisPavi MuruganathanNo ratings yet
- Non-Surgical Management of Perforated Jejunal DiverticulumDocument6 pagesNon-Surgical Management of Perforated Jejunal DiverticulumIJAR JOURNALNo ratings yet
- Grand Round Presentation 24-12-2016Document35 pagesGrand Round Presentation 24-12-2016Md.AlauddinNo ratings yet
- Complex Care Plan 1Document12 pagesComplex Care Plan 1api-496883420No ratings yet
- Case 2.24Document2 pagesCase 2.24nadiaNo ratings yet
- Case Report: Rapport de CasDocument6 pagesCase Report: Rapport de CasRayza LubisNo ratings yet
- NC FARHAN RESPI SalinanDocument21 pagesNC FARHAN RESPI SalinanRima KhairunnisaNo ratings yet
- NC Khaerunnisa-HemaDocument19 pagesNC Khaerunnisa-HemaDodi DiNo ratings yet
- Cirrhosis of LiverDocument22 pagesCirrhosis of LiverKrini Tandel50% (2)
- Clinical Conference 21 August 2022: Eria (New Case)Document16 pagesClinical Conference 21 August 2022: Eria (New Case)mujahidah nursinNo ratings yet
- PancreatitisDocument28 pagesPancreatitisFrench Pastolero-ManaloNo ratings yet
- Acute Pancreatitis NewDocument34 pagesAcute Pancreatitis NewDrscottmccallNo ratings yet
- The CaseDocument33 pagesThe CasemarunxNo ratings yet
- JSS College of Pharmacy, Ooty: Case Title - HyperuricemiaDocument7 pagesJSS College of Pharmacy, Ooty: Case Title - HyperuricemiaVineth MartinNo ratings yet
- NC - Muhammad RaditDocument18 pagesNC - Muhammad RaditDodi DiNo ratings yet
- Gilbert2021 Article A17-year-oldBoyWithProgressiveDocument2 pagesGilbert2021 Article A17-year-oldBoyWithProgressivefatinarmiantoNo ratings yet
- Atlas of High-Resolution Manometry, Impedance, and pH MonitoringFrom EverandAtlas of High-Resolution Manometry, Impedance, and pH MonitoringNo ratings yet
- Fast Facts: Acute and Recurrent Pancreatitis: Using evidence to support treatmentFrom EverandFast Facts: Acute and Recurrent Pancreatitis: Using evidence to support treatmentNo ratings yet
- Visitor Perception Related to the Quality of Service in Todo Tourism VillageDocument10 pagesVisitor Perception Related to the Quality of Service in Todo Tourism VillageInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Quizlet's Usefulness for Vocabulary Learning: Perceptions of High-Level and Low-Level Chinese College EFL LearnersDocument5 pagesQuizlet's Usefulness for Vocabulary Learning: Perceptions of High-Level and Low-Level Chinese College EFL LearnersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Enhancing Estimating the Charge Level in Electric Vehicles: Leveraging Force Fluctuation and Regenerative Braking DataDocument6 pagesEnhancing Estimating the Charge Level in Electric Vehicles: Leveraging Force Fluctuation and Regenerative Braking DataInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Health Care - An Android Application Implementation and Analyzing user Experience Using PythonDocument7 pagesHealth Care - An Android Application Implementation and Analyzing user Experience Using PythonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Gravity Investigations Applied to the Geological Framework Study of the Mambasa Territory in Democratic Republic of CongoDocument9 pagesGravity Investigations Applied to the Geological Framework Study of the Mambasa Territory in Democratic Republic of CongoInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A New Model of Rating to Evaluate Start-ups in Emerging Indian MarketDocument7 pagesA New Model of Rating to Evaluate Start-ups in Emerging Indian MarketInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Intrusion Detection System with Ensemble Machine Learning Approaches using VotingClassifierDocument4 pagesIntrusion Detection System with Ensemble Machine Learning Approaches using VotingClassifierInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Proof of Concept Using BLE to Optimize Patients Turnaround Time (PTAT) in Health CareDocument14 pagesA Proof of Concept Using BLE to Optimize Patients Turnaround Time (PTAT) in Health CareInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Developing Digital Fluency in Early Education: Narratives of Elementary School TeachersDocument11 pagesDeveloping Digital Fluency in Early Education: Narratives of Elementary School TeachersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Optimizing Bio-Implant Materials for Femur Bone Replacement:A Multi-Criteria Analysis and Finite Element StudyDocument5 pagesOptimizing Bio-Implant Materials for Femur Bone Replacement:A Multi-Criteria Analysis and Finite Element StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Design and Implementation of Software-Defined ReceiverDocument8 pagesDesign and Implementation of Software-Defined ReceiverInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Naturopathic Approaches to Relieving Constipation: Effective Natural Treatments and TherapiesDocument10 pagesNaturopathic Approaches to Relieving Constipation: Effective Natural Treatments and TherapiesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Crop Monitoring System with Water Moisture Levels Using ControllerDocument8 pagesCrop Monitoring System with Water Moisture Levels Using ControllerInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Oral Anti-Diabetic Semaglutide: A GLP-1 RA PeptideDocument11 pagesOral Anti-Diabetic Semaglutide: A GLP-1 RA PeptideInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Year Wise Analysis and Prediction of Gold RatesDocument8 pagesYear Wise Analysis and Prediction of Gold RatesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Government's Role in DMO-based Urban Tourism in Kayutangan area of Malang cityDocument8 pagesThe Government's Role in DMO-based Urban Tourism in Kayutangan area of Malang cityInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Fahfi/Mochaina Illegal Gambling Activities and its Average Turnover within Limpopo ProvinceDocument8 pagesFahfi/Mochaina Illegal Gambling Activities and its Average Turnover within Limpopo ProvinceInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Analysis of the Quality of Community Satisfaction in Public Services in Tanjungpinang Class I State Detention HouseDocument13 pagesAnalysis of the Quality of Community Satisfaction in Public Services in Tanjungpinang Class I State Detention HouseInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Inclusive Leadership in the South African Police Service (SAPS)Document26 pagesInclusive Leadership in the South African Police Service (SAPS)International Journal of Innovative Science and Research TechnologyNo ratings yet
- A Study to Assess the Effectiveness of Bronchial Hygiene Therapy (BHT) on Clinical Parameters among Mechanically Ventilated Patients in Selected Hospitals at ErodeDocument7 pagesA Study to Assess the Effectiveness of Bronchial Hygiene Therapy (BHT) on Clinical Parameters among Mechanically Ventilated Patients in Selected Hospitals at ErodeInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Effects of Nanoplastics on Human Health: A Comprehensive StudyDocument7 pagesEffects of Nanoplastics on Human Health: A Comprehensive StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Zilebesiran: The First siRNA Drug Therapy for HypertensionDocument5 pagesZilebesiran: The First siRNA Drug Therapy for HypertensionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Analysis of the Effectiveness of Based Public Services Information and Communication Technology (ICT)Document10 pagesAnalysis of the Effectiveness of Based Public Services Information and Communication Technology (ICT)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Income Diversification of Rural Households in Bangladesh (2022-23)Document5 pagesIncome Diversification of Rural Households in Bangladesh (2022-23)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Effectiveness of Organizing Crossing Transport Services in the Maritime Area of Riau Islands ProvinceDocument10 pagesEffectiveness of Organizing Crossing Transport Services in the Maritime Area of Riau Islands ProvinceInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Design and Analysis of Various Formwork SystemsDocument6 pagesDesign and Analysis of Various Formwork SystemsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Environmental Sanitation – A Therapy for Healthy Living for Sustainable Development. A Case Study of Argungu Township Kebbi State, North Western NigeriaDocument15 pagesEnvironmental Sanitation – A Therapy for Healthy Living for Sustainable Development. A Case Study of Argungu Township Kebbi State, North Western NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Association Between Gender and Depression Among College StudentsDocument4 pagesAssociation Between Gender and Depression Among College StudentsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Reintegration of Dairy in Daily American Diets: A Biochemical and Nutritional PerspectiveDocument1 pageReintegration of Dairy in Daily American Diets: A Biochemical and Nutritional PerspectiveInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Appraisal of Nursing Care Received and it’s Satisfaction: A Case Study of Admitted Patients in Afe Babalola Multisystem Hospital, Ado Ekiti, Ekiti StateDocument12 pagesAppraisal of Nursing Care Received and it’s Satisfaction: A Case Study of Admitted Patients in Afe Babalola Multisystem Hospital, Ado Ekiti, Ekiti StateInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- AAMA - Anatomy and Physiology QuestionsDocument11 pagesAAMA - Anatomy and Physiology QuestionsHUAWEI HUAWEINo ratings yet
- Whats Out Addis November Isuue PDFDocument27 pagesWhats Out Addis November Isuue PDFRahul PanditNo ratings yet
- Ozone As A Disinfecting Agent in The Reuse of WastewaterDocument9 pagesOzone As A Disinfecting Agent in The Reuse of WastewaterJoy Das MahapatraNo ratings yet
- Innovative Educational - Welfare SocietyDocument4 pagesInnovative Educational - Welfare SocietyAjay ChikersalNo ratings yet
- General Guidelines For Skin CareDocument4 pagesGeneral Guidelines For Skin CareDaesungNo ratings yet
- ISBB Wall Notes PDFDocument8 pagesISBB Wall Notes PDFLynx EemanNo ratings yet
- Sun Life Takaful - 16062022Document8 pagesSun Life Takaful - 16062022PUI MUN CHANGNo ratings yet
- Prayer Renouncing PrideDocument5 pagesPrayer Renouncing Pridemazzagra100% (1)
- Blondin-Brosseau Et Al 2021Document28 pagesBlondin-Brosseau Et Al 2021JefersonMatosdeColaresNo ratings yet
- Staphisagria: COMMON NAME: StavesacreDocument10 pagesStaphisagria: COMMON NAME: StavesacreAbhijeet SinghNo ratings yet
- ScabiesDocument9 pagesScabiesBhoomi GoyaniNo ratings yet
- Odisha List of Important Medicinal Plants and Their UsesDocument4 pagesOdisha List of Important Medicinal Plants and Their UseslakshmibavaNo ratings yet
- Stevens-Johnson Syndrome: Review of The Literature: Stitt CarolinaDocument4 pagesStevens-Johnson Syndrome: Review of The Literature: Stitt CarolinaNurul AfiahNo ratings yet
- AripiprazoleDocument2 pagesAripiprazoleKrisianne Mae Lorenzo FranciscoNo ratings yet
- Psychiatry: Psychology-Psychiatric Evaluation - 1 (Medical Transcription Sample Report)Document7 pagesPsychiatry: Psychology-Psychiatric Evaluation - 1 (Medical Transcription Sample Report)Nguyên VũNo ratings yet
- PREBOARD Nursing Practice 2Document13 pagesPREBOARD Nursing Practice 2Blaine ManiegoNo ratings yet
- Final Micro Module 1Document73 pagesFinal Micro Module 1Ahmed KerAtyNo ratings yet
- Mrcs Part-A Online Preparatory Course Mock Exam-1 Paper - 2Document26 pagesMrcs Part-A Online Preparatory Course Mock Exam-1 Paper - 2Rami RaedNo ratings yet
- For Anorexia NervosaDocument18 pagesFor Anorexia NervosaLADY JOWAHER ALLASNo ratings yet
- Nursing in Dermatovenereology. 1Document66 pagesNursing in Dermatovenereology. 1ABDALRAHMAN ABDALLAH KASEMNo ratings yet
- ca chủ tịch SchreberDocument4 pagesca chủ tịch SchreberAnh MinhNo ratings yet
- Nimesulide BrandsDocument1 pageNimesulide BrandsKimberly RiceNo ratings yet
- Acute CholecystitisDocument27 pagesAcute CholecystitisAleks MendozaNo ratings yet
- Animal Experiments in Medical MicrobiologyDocument70 pagesAnimal Experiments in Medical Microbiologyira_praharaj100% (3)
- OER - CNA Field Manual Revised 8-27-2014Document192 pagesOER - CNA Field Manual Revised 8-27-2014Regina PunNo ratings yet
- Drug StudyDocument2 pagesDrug StudycrisielabNo ratings yet
- Potential NCPDocument2 pagesPotential NCPKate WeyganNo ratings yet
- Drugs 2018 FebDocument143 pagesDrugs 2018 FebTuliNo ratings yet