
Mardis Et Al., 2009
Mardis Et Al., 2009
You might also like
- Pedigree Chart WorksheetDocument72 pagesPedigree Chart Worksheetapi-3075658820% (1)
- Genome Sequencing As An Alternative To Cytogenetic Analysis in Myeloid CancersDocument12 pagesGenome Sequencing As An Alternative To Cytogenetic Analysis in Myeloid CancersJck YyNo ratings yet
- Age-Related Clonal HematopoiesisDocument11 pagesAge-Related Clonal HematopoiesisgiulioNo ratings yet
- 2013 Clinical WES Nejmoa1306555Document10 pages2013 Clinical WES Nejmoa1306555MCuk2606No ratings yet
- SF3B1 and Other Novel Cancer Genes: in Chronic Lymphocytic LeukemiaDocument10 pagesSF3B1 and Other Novel Cancer Genes: in Chronic Lymphocytic LeukemiaRafael ColinaNo ratings yet
- Cancer Research Review PDFDocument57 pagesCancer Research Review PDFCiocan AlexandraNo ratings yet
- Mesenchymal Stem Cells Literature ReviewDocument9 pagesMesenchymal Stem Cells Literature ReviewafdtygyhkNo ratings yet
- Detection of Mutations in EGFR in Circulating Lung-Cancer Cells.Document12 pagesDetection of Mutations in EGFR in Circulating Lung-Cancer Cells.Joonseok ParkNo ratings yet
- Variant of TYR and Autoimmunity Susceptibility Loci in Generalized VitiligoDocument12 pagesVariant of TYR and Autoimmunity Susceptibility Loci in Generalized VitiligoIvo AfianiNo ratings yet
- A Switch in Time Through Genes Aligned Unraveling The Geno - 2020 - Cell StemDocument3 pagesA Switch in Time Through Genes Aligned Unraveling The Geno - 2020 - Cell StemBandar Ternama XBNo ratings yet
- Aula LogisticaDocument64 pagesAula LogisticaglaucomassotoNo ratings yet
- Chromosomal Microarray Versus Karyotyping For Prenatal Diagnosis - 2012Document10 pagesChromosomal Microarray Versus Karyotyping For Prenatal Diagnosis - 2012George CarvalhoNo ratings yet
- Libro de InmunohematologiaDocument44 pagesLibro de InmunohematologiaMijael Edgar Guadalupe MagnoNo ratings yet
- Postdoc Position in David Chen Lab at City of HopeDocument2 pagesPostdoc Position in David Chen Lab at City of HopeAdolfo De La Rosa JrNo ratings yet
- Radiation-Induced Bystander Effects - Implications For Cancer - Mothersill and Seymour, 2004Document8 pagesRadiation-Induced Bystander Effects - Implications For Cancer - Mothersill and Seymour, 2004Isabella LiedtkeNo ratings yet
- CMT WEGS Nejmoa0908094Document11 pagesCMT WEGS Nejmoa0908094MCuk2606No ratings yet
- Wyandt2017 Book HumanChromosomeVariationHeteroDocument500 pagesWyandt2017 Book HumanChromosomeVariationHeteroRicardo OlguinNo ratings yet
- Lapun: ImashukuDocument2 pagesLapun: ImashukuApsopela SandiveraNo ratings yet
- This Content Downloaded From 88.231.62.252 On Tue, 25 Apr 2023 09:08:44 UTCDocument8 pagesThis Content Downloaded From 88.231.62.252 On Tue, 25 Apr 2023 09:08:44 UTCMaman AhmadNo ratings yet
- Stem Cell Cancer: By: Monali.R.Bhakta Sem: 8 Roll No: 86Document13 pagesStem Cell Cancer: By: Monali.R.Bhakta Sem: 8 Roll No: 86coolharsh111No ratings yet
- References: Department of Pharmaceutical Sciences, Kumaun UniversityDocument3 pagesReferences: Department of Pharmaceutical Sciences, Kumaun Universityhemajoshi4517No ratings yet
- Zheng Hong 郑 红 Department of Medical Genetics & Cell BiologyDocument63 pagesZheng Hong 郑 红 Department of Medical Genetics & Cell BiologyinakiNo ratings yet
- BloodDocument145 pagesBloodRanintha Surbakti100% (2)
- Stem Cells and Cancer Stem Cells, Volume 3 - Stem Cells and Cancer Stem Cells, Therapeutic Applications in Disease and Injury - Volume 3Document426 pagesStem Cells and Cancer Stem Cells, Volume 3 - Stem Cells and Cancer Stem Cells, Therapeutic Applications in Disease and Injury - Volume 3Artan100% (1)
- Tumor Cell Intrinsic FactorsDocument24 pagesTumor Cell Intrinsic FactorsBanh Ti HonNo ratings yet
- Lee Eun JooDocument344 pagesLee Eun JooDana GoldoniNo ratings yet
- Lehmann Werman 2016Document9 pagesLehmann Werman 2016Felipe MNo ratings yet
- Nej Mo A 1516767Document11 pagesNej Mo A 1516767mayrapp16No ratings yet
- NEJMoa 1700554Document9 pagesNEJMoa 1700554Titi OrellanaNo ratings yet
- Wallace 20131Document48 pagesWallace 20131DCPNo ratings yet
- Glioblastoma Cells Through An ERK-dependent Pathway, Oncol. Rep., 28: 41-48Document1 pageGlioblastoma Cells Through An ERK-dependent Pathway, Oncol. Rep., 28: 41-48ilssNo ratings yet
- NCI60 Target RefsDocument6 pagesNCI60 Target RefsDioxelis LópezNo ratings yet
- NIH Public AccessDocument20 pagesNIH Public Accessaaasim93No ratings yet
- ReferencesDocument4 pagesReferencesfidabimeeNo ratings yet
- Integrative Multi-Omic Cancer Profiling Reveals DNA Methylation Patterns Associated With Therapeutic Vulnerability and Cell-Of-OriginDocument42 pagesIntegrative Multi-Omic Cancer Profiling Reveals DNA Methylation Patterns Associated With Therapeutic Vulnerability and Cell-Of-Origin戴义宾No ratings yet
- Stem Cell ReportDocument2 pagesStem Cell Reporttaleenwas2No ratings yet
- Oncogenic CSF3R Mutations in Chronic Neutrophilic Leukemia and Atypical CMLDocument1 pageOncogenic CSF3R Mutations in Chronic Neutrophilic Leukemia and Atypical CMLSav GaNo ratings yet
- XMRK in MedakaDocument4 pagesXMRK in Medakaxiaozi92No ratings yet
- Melanoma With Striking Adenocarcinomatous DifferentiationHUMANSDocument11 pagesMelanoma With Striking Adenocarcinomatous DifferentiationHUMANSgranulomatous pneumoniaNo ratings yet
- Germline Mutations in Predisposition Genes in Pediatric CancerDocument11 pagesGermline Mutations in Predisposition Genes in Pediatric CancerGuadalupeA.OsorioNo ratings yet
- (2983) of Double Esterase in Bone Marrow Cells of Patients WithDocument2 pages(2983) of Double Esterase in Bone Marrow Cells of Patients WithApsopela SandiveraNo ratings yet
- JurnalDocument3 pagesJurnalnurlaras201102No ratings yet
- Genomic Instability in CancerDocument17 pagesGenomic Instability in Cancerhibahussain74305No ratings yet
- Colorectal Cancer in StoolDocument8 pagesColorectal Cancer in StoolAnmol KumarNo ratings yet
- Ata Ur Rehman: Research Proposal For PHD AdmissionDocument5 pagesAta Ur Rehman: Research Proposal For PHD AdmissionSajjad AliNo ratings yet
- The Cell Biological Basis of Cancer - ThesisDocument50 pagesThe Cell Biological Basis of Cancer - ThesisRamesh MahakurNo ratings yet
- Thorsson 2018 Immune Landscape of CancerDocument34 pagesThorsson 2018 Immune Landscape of Cancershivi misraNo ratings yet
- Cancer EpigeneticsDocument18 pagesCancer EpigeneticsIrfan AlviNo ratings yet
- JurnalDocument5 pagesJurnalNers A 2016No ratings yet
- Corrections: Neuroscience. Cell BiologyDocument8 pagesCorrections: Neuroscience. Cell BiologySammer BurgosNo ratings yet
- The Disruption of Profiling of Serotonergic Neurons, Results in Autism-Related BehaviorsDocument22 pagesThe Disruption of Profiling of Serotonergic Neurons, Results in Autism-Related BehaviorsAngelinni Taglioni StangeNo ratings yet
- GenomiclibraryDocument2 pagesGenomiclibraryJonathan AlanizNo ratings yet
- Microenvironment Drives Cell State, Plasticity, and Drug Response in Pancreatic CancerDocument46 pagesMicroenvironment Drives Cell State, Plasticity, and Drug Response in Pancreatic Cancerka1400ra-sNo ratings yet
- Guangbin Luo-Curriculum VitaeDocument6 pagesGuangbin Luo-Curriculum Vitaeluol35No ratings yet
- This Content Downloaded From 120.126.70.24 On Wed, 29 Mar 2023 11:59:10 UTCDocument8 pagesThis Content Downloaded From 120.126.70.24 On Wed, 29 Mar 2023 11:59:10 UTCmarcia suNo ratings yet
- Phipps Solitary Fibrous Tumors of The Pleura Results of Surgical Treatment 2009Document13 pagesPhipps Solitary Fibrous Tumors of The Pleura Results of Surgical Treatment 2009JZNo ratings yet
- Lynch SyndromeDocument6 pagesLynch SyndromeduminduNo ratings yet
- 2002 DavidsonDocument5 pages2002 DavidsonBianca PapadopolNo ratings yet
- Majalah Kedokteran Atmajaya, 2 (2) : Halaman 85-96: WWW - LeukemiaDocument0 pagesMajalah Kedokteran Atmajaya, 2 (2) : Halaman 85-96: WWW - LeukemiaHasan Ibn MutholibNo ratings yet
- Daftar PustakaDocument6 pagesDaftar PustakaMerliana DebyantiNo ratings yet
- The Bethesda System for Reporting Thyroid Cytopathology: Definitions, Criteria and Explanatory NotesFrom EverandThe Bethesda System for Reporting Thyroid Cytopathology: Definitions, Criteria and Explanatory NotesNo ratings yet
- Population-Based Incremental LearningDocument3 pagesPopulation-Based Incremental Learningemma698No ratings yet
- Brosur KIT HPV DNADocument2 pagesBrosur KIT HPV DNARonna EfriyanaNo ratings yet
- Cloning Dolly & MicromanipulationDocument29 pagesCloning Dolly & Micromanipulationnitinyadav16No ratings yet
- Meiosis LabDocument9 pagesMeiosis Labpeter103958No ratings yet
- 13-1: The Genetic Material: Frederick Griffith's Experiment - TransformationDocument7 pages13-1: The Genetic Material: Frederick Griffith's Experiment - Transformationapi-233187566No ratings yet
- Chapter 8.4-8.7 Study GuideDocument5 pagesChapter 8.4-8.7 Study GuideHomerNo ratings yet
- PGT & TGT (Biology) SyllabusDocument7 pagesPGT & TGT (Biology) SyllabusNikkisonuNo ratings yet
- Ronda2019 SupDocument31 pagesRonda2019 SupEmna BouhajjaNo ratings yet
- Trancriptome and Proteome AnalysisDocument68 pagesTrancriptome and Proteome AnalysisNeeru RedhuNo ratings yet
- Flowering Pathway in Arabidopsis-CouplandDocument3 pagesFlowering Pathway in Arabidopsis-CouplandJay Prakash MauryaNo ratings yet
- 2023 Article 1738Document19 pages2023 Article 1738Murillo Pyaia Alves PaixãoNo ratings yet
- RESEARCH PaperDocument6 pagesRESEARCH PaperLlana ToribioNo ratings yet
- Grade 12 Biology Mechanisms of InheritanceDocument22 pagesGrade 12 Biology Mechanisms of Inheritanceapi-635512040No ratings yet
- Molecular Markers and Their Applicationsin CattleDocument5 pagesMolecular Markers and Their Applicationsin CattleDEEPANKER BISHTNo ratings yet
- CSI Wildlife: Analyzing Genetic EvidenceDocument4 pagesCSI Wildlife: Analyzing Genetic EvidenceInsaf MNo ratings yet
- La Biología de La Cromatina Complejos de Remodelación: FurtherDocument24 pagesLa Biología de La Cromatina Complejos de Remodelación: FurtherVíc AltamarNo ratings yet
- ATP 2023-24 GR 12 Life SciDocument4 pagesATP 2023-24 GR 12 Life SciPfarelo TshidzumbaNo ratings yet
- hssb0800t StudygdbDocument17 pageshssb0800t StudygdbyawahabNo ratings yet
- Liu2011 PDFDocument6 pagesLiu2011 PDFAnonymous cUzAJWocPCNo ratings yet
- Meiosis: Chromatids (The Two Halves of A Duplicated Chromosome), As inDocument29 pagesMeiosis: Chromatids (The Two Halves of A Duplicated Chromosome), As inyamamaNo ratings yet
- CITOSISDocument3 pagesCITOSISKylliíanNo ratings yet
- Types of MutationsDocument43 pagesTypes of MutationsElyNo ratings yet
- Molecular Cell Biology (Chapter 25 - Cancer)Document42 pagesMolecular Cell Biology (Chapter 25 - Cancer)qwertyNo ratings yet
- Articulo MacacosDocument15 pagesArticulo MacacosAdolfo Mora SanchezNo ratings yet
- 15.1 History of Evolutionary ThoughtDocument11 pages15.1 History of Evolutionary ThoughtlutimoNo ratings yet
- Mutation and Sickle CellDocument16 pagesMutation and Sickle Cellapi-309893409No ratings yet
- Biotechnology and Its Applications: Pre-Medical: Biology AllenDocument5 pagesBiotechnology and Its Applications: Pre-Medical: Biology AllenJK JHANo ratings yet
- ARECA ThesisDocument32 pagesARECA ThesisMdkhurshed AlamNo ratings yet
- Biotechnology SyllabusDocument111 pagesBiotechnology SyllabusSatyam SinghNo ratings yet

























































































The n e w e ng l a n d j o u r na l of m e dic i n e
original article
Recurring Mutations Found by Sequencing
an Acute Myeloid Leukemia Genome
Elaine R. Mardis, Ph.D., Li Ding, Ph.D., David J. Dooling, Ph.D.,
David E. Larson, Ph.D., Michael D. McLellan, B.S., Ken Chen, Ph.D.,
Daniel C. Koboldt, M.S., Robert S. Fulton, M.S., Kim D. Delehaunty, B.A.,
Sean D. McGrath, M.S., Lucinda A. Fulton, M.S., Devin P. Locke, Ph.D.,
Vincent J. Magrini, Ph.D., Rachel M. Abbott, B.S., Tammi L. Vickery, B.S.,
Jerry S. Reed, M.S., Jody S. Robinson, M.S., Todd Wylie, B.S., Scott M. Smith,
Lynn Carmichael, B.S., James M. Eldred, Christopher C. Harris, B.S.,
Jason Walker, B.A., B.S., Joshua B. Peck, M.B.A., Feiyu Du, M.S.,
Adam F. Dukes, B.A., Gabriel E. Sanderson, B.S., Anthony M. Brummett,
Eric Clark, Joshua F. McMichael, B.S., Rick J. Meyer, M.S.,
Jonathan K. Schindler, B.S., B.A., Craig S. Pohl, M.S., John W. Wallis, Ph.D.,
Xiaoqi Shi, M.S., Ling Lin, M.S., Heather Schmidt, B.S., Yuzhu Tang, M.D.,
Carrie Haipek, M.S., Madeline E. Wiechert, M.S., Jolynda V. Ivy, M.B.A.,
Joelle Kalicki, B.S., Glendoria Elliott, Rhonda E. Ries, M.A.,
Jacqueline E. Payton, M.D., Ph.D., Peter Westervelt, M.D., Ph.D.,
Michael H. Tomasson, M.D., Mark A. Watson, M.D., Ph.D., Jack Baty, B.A.,
Sharon Heath, William D. Shannon, Ph.D., Rakesh Nagarajan, M.D., Ph.D.,
Daniel C. Link, M.D., Matthew J. Walter, M.D., Timothy A. Graubert, M.D.,
John F. DiPersio, M.D., Ph.D., Richard K. Wilson, Ph.D., and Timothy J. Ley, M.D.
A bs t r ac t
Background
From the Departments of Genetics (E.R.M., The full complement of DNA mutations that are responsible for the pathogenesis of
L.D., V.J.M., R.K.W., T.J.L.), Medicine acute myeloid leukemia (AML) is not yet known.
(R.E.R., P.W., M.H.T., S.H., W.D.S., D.C.L.,
M.J.W., T.A.G., J.F.D., T.J.L.), and Pathology Methods
and Immunology (J.E.P., M.A.W., R.N.); We used massively parallel DNA sequencing to obtain a very high level of coverage
the Genome Center (E.R.M., L.D., D.J.D.,
D.E.L., M.D.M., K.C., D.C.K., R.S.F., K.D.D.,
(approximately 98%) of a primary, cytogenetically normal, de novo genome for AML
S.D.M., L.A.F., D.P.L., V.J.M., R.M.A., with minimal maturation (AML-M1) and a matched normal skin genome.
T.L.V., J.S. Reed, J.S. Robinson, T.W., S.M.S., Results
L.C., J.M.E., C.C.H., J.W., J.B.P., F.D.,
A.F.D., G.E.S., A.M.B., E.C., J.F.M., R.J.M., We identified 12 acquired (somatic) mutations within the coding sequences of genes
J.K.S., C.S.P., J.W.W., X.S., L.L., H.S., Y.T., and 52 somatic point mutations in conserved or regulatory portions of the genome.
C.H., M.E.W., J.V.I., J.K., G.E., M.A.W., All mutations appeared to be heterozygous and present in nearly all cells in the
R.K.W., T.J.L.); Siteman Cancer Center
(P.W., M.H.T., M.A.W., S.H., W.D.S., R.N., tumor sample. Four of the 64 mutations occurred in at least 1 additional AML
D.C.L., M.J.W., T.A.G., J.F.D., R.K.W., T.J.L.); sample in 188 samples that were tested. Mutations in NRAS and NPM1 had been
and the Division of Biostatistics (J.B.) — identified previously in patients with AML, but two other mutations had not been
all at Washington University, St. Louis. Ad-
dress reprint requests to Dr. Ley at Wash-
identified. One of these mutations, in the IDH1 gene, was present in 15 of 187 ad-
ington University, 660 S. Euclid Ave., ditional AML genomes tested and was strongly associated with normal cytogenetic
Campus Box 8007, St. Louis, MO 63110, status; it was present in 13 of 80 cytogenetically normal samples (16%). The other
or at timley@wustl.edu.
was a nongenic mutation in a genomic region with regulatory potential and conser-
This article (10.1056/NEJMoa0903840) was vation in higher mammals; we detected it in one additional AML tumor. The AML
published on August 5, 2009, at NEJM.org. genome that we sequenced contains approximately 750 point mutations, of which
only a small fraction are likely to be relevant to pathogenesis.
N Engl J Med 2009;361:1058-66.
Copyright © 2009 Massachusetts Medical Society. Conclusions
By comparing the sequences of tumor and skin genomes of a patient with AML-M1,
we have identified recurring mutations that may be relevant for pathogenesis.
1058 n engl j med 361;11 nejm.org september 10, 2009
The New England Journal of Medicine
Downloaded from nejm.org at TEXAS STATE UNIV on May 17, 2013. For personal use only. No other uses without permission.
Copyright © 2009 Massachusetts Medical Society. All rights reserved.
Recurring Mutations Found by Sequencing an AML Genome
A
cute myeloid leukemia (AML) is a identification of sequence variants, validation of
clonal hematopoietic disease caused by variants and determination of the prevalence of
both inherited and acquired genetic alter variants in the index AML tumor, and screening
ations.1-3 Current AML classification and prog- of additional AML samples are provided in the
nostic systems incorporate genetic information Supplementary Appendix, available with the full
but are limited to known abnormalities that have text of this article at NEJM.org. All the high-
previously been identified with the use of cytoge- quality single-nucleotide variants (SNVs) that were
netics, array comparative genomic hybridization found in tumor and skin samples from this pa-
(CGH), gene-expression profiling, and the rese- tient are available in the database of genotypes
quencing of candidate genes (see the Glossary). and phenotypes (dbGaP) of the National Center
The karyotyping of AML cells remains the for Biotechnology Information (accession number,
most powerful predictor of the outcome in pa- phs000159.v1.p1).
tients with AML and is routinely used by clini
cians.4,5 As an adjunct to cytogenetic studies, R e sult s
small subcytogenetic amplifications and dele-
tions can be identified with the use of genomic Case Report
methods, such as single-nucleotide-polymorphism A previously healthy 38-year-old man of European
(SNP) array and array CGH platforms (see the ancestry presented with fatigue and a cough. The
Glossary). However, these techniques remain in- white-cell count was 39,800 cells per cubic milli-
vestigational, and studies6-9 suggest that there meter, with 97% blasts; the hemoglobin level was
are few recurrent acquired copy-number altera- 8.9 g per deciliter, and the platelet count was
tions in each AML genome. Gene-expression 35,000 per cubic millimeter. A bone marrow ex-
profiling has identified patients with known amination revealed 90% cellularity and 86% my-
chromosomal lesions and genetic mutations and eloperoxidase-positive blasts (Fig. 1 in the Supple-
subgroups of patients with normal cytogenetic mentary Appendix). Routine cytogenetic analysis
profiles who have variable clinical outcomes.10,11 of bone marrow samples revealed a normal 46,XY
Expression profiling has yielded single-gene pre- karyotype. There was no family history of leuke-
dictors of outcome that are currently being mia. The patient’s mother had received the diag-
evaluated for clinical use.12-16 Candidate-gene re- nosis of breast cancer at the age of 60 years and
sequencing studies have also identified recurrent of non-Hodgkin’s lymphoma at the age of 63
mutations in several genes — for example, genes years; her half-sister had received the diagnosis
encoding FMS-related tyrosine kinase 3 (FLT3) of breast cancer at the age of 50 years.
and nucleophosmin 1 (NPM1) — that can help to Samples of the patient’s bone marrow and
stratify patients with normal cytogenetic pro- skin were banked for whole-genome sequencing
files according to risk and to identify patients under a protocol approved by the institutional re-
for targeted therapy (e.g., those with mutated view board at Washington University. The patient
FLT3).3,12,17 However, the revised classification provided written informed consent.
systems are imperfect, suggesting that impor- The patient was treated initially with a 7-day
tant genetic factors for the pathogenesis of AML course of infusional cytarabine and with a 3-day
remain to be discovered. course of daunorubicin. Within 5 weeks, he had
We have previously described the sequence of complete morphologic remission and recovery of
an entire AML genome from a patient who had white-cell and platelet counts. The patient subse-
AML with minimal maturation (AML-M1) and a quently received consolidation therapy with four
normal cytogenetic profile.18 Here we describe the cycles of high-dose cytarabine without any fur-
genome sequence of another such tumor and re- ther antileukemic therapy. He remained in com-
curring mutations in additional AML tumors. plete remission 3 years later.
Me thods Characterization of the Tumor Genome
DNA samples from the patient’s bone marrow
Details regarding the methods for library produc- sample at the time of initial presentation and a
tion, DNA sequencing with the Illumina Genome normal skin-biopsy specimen obtained after the
Analyzer II,19 evaluation of sequence coverage, patient’s disease was in remission were labeled
n engl j med 361;11 nejm.org september 10, 2009 1059
The New England Journal of Medicine
Downloaded from nejm.org at TEXAS STATE UNIV on May 17, 2013. For personal use only. No other uses without permission.
Copyright © 2009 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
Glossary
Build 36 of the human reference genome: The most current version of the assembled human genome reference sequence,
available online at the National Center for Biotechnology Information (www.ncbi.nlm.nih.gov/).
Comparative genomic hybridization (CGH): A comparison of DNA abundance, throughout the genome, between two DNA
samples to identify regions where DNA copies have been gained or lost.
dbSNP: A publicly available database of known DNA variants, housed at the National Center for Biotechnology Informa
tion (www.ncbi.nlm.nih.gov/SNP).
Diploid coverage: A metric used in whole-genome sequencing studies to describe the likelihood of detecting both alleles
at any given nucleotide position in a genome.
Genic: Regions of the genome that contain genes, including their exons and introns.
Haploid coverage: A metric used in whole-genome sequencing studies to describe detection of each nucleotide posi-
tion in a genome for at least one allele; “1× coverage” is equivalent to the size of the genome (e.g., approximately
3 billion base pairs for the human genome).
Next-generation sequencing: A variety of new techniques that have in common the generation of DNA sequence from
single molecules of DNA, rather than pools of DNA templates; hundreds of millions of DNA fragments can be se-
quenced at the same time on a single platform (massively parallel sequencing).
Paired-end reads: DNA sequences that are produced on next-generation sequencing platforms by sequencing both ends
of DNA fragments, resulting in higher confidence in assigning the sequence a position in the reference genome
and allowing the detection of structural variations.
Partial uniparental disomy: An acquired somatic recombination event that causes the duplication of a part of a chromo-
some from one parent, resulting in a “copy-number neutral” loss of heterozygosity for a chromosomal segment.
Resequencing: Obtaining the DNA sequence of additional members of a species for which a completed reference se-
quence is known and to which comparisons can be made.
Sequencing run: The sequence that is generated by a complete Illumina flow cell or a similar next-generation sequencing
platform; one sequencing run generates many billions of base pairs of sequence.
Single-nucleotide polymorphism (SNP): A position in the genome where some individuals in a population inherit a
change in a single nucleotide that differs from the reference genome.
Single-nucleotide variant (SNV): A difference in a DNA sequence of a sample at a single position in the genome, as
compared with the reference genome; each variant may represent either an inherited or an acquired change.
SNP array: A microarray-based assay system that allows for simultaneous measurement of nucleotide sequence and
abundance in a DNA sample at possibly hundreds of thousands of positions in the genome.
and genotyped with the use of the Affymetrix arrays, we confirmed the detection of both alleles
Genome-Wide Human SNP Array 6.0. The tumor of 98.5% of the approximately 45,000 high-qual-
genome had no detectable somatic copy-number ity heterozygous SNPs in the tumor sample and
alterations and no regions of partial uniparental 97.4% of the approximately 45,000 high-quality
disomy (Glossary, and Fig. 2 in the Supplemen- heterozygous SNPs in the skin sample.
tary Appendix). RNA that was derived from the A summary of the sequence differences be-
same bone marrow sample was analyzed with tween the patient’s tumor genome and National
the use of the Affymetrix GeneChip Human Ge- Center for Biotechnology Information build 36 of
nome U133 Plus 2.0 array, which revealed an ex- the human reference genome is shown in Figure 1
pression signature similar to that of many other (see the Glossary).20 We identified 3,872,936 SNVs
cytogenetically normal marrow samples from pa- in the tumor genome, of which 3,464,449 passed
tients with AML-M1 (Fig. 2 in the Supplementary a stringent calling filter. Of these SNVs, 3,377,680
Appendix). (97.5%) were detected in the skin genome, indi-
cating that they were inherited variants. Of the
Sequence Coverage and Potential Mutations 86,769 potentially novel somatic SNVs, 66,513 had
We sequenced 69.9 billion base pairs (23.3× hap- been described previously.
loid coverage) from DNA libraries that we gener- We binned the remaining 20,256 SNVs into
ated from the tumor sample and 63.9 billion base four tiers, which are detailed in the Supplemen-
pairs from libraries that we generated from the tary Appendix. Briefly, tier 1 contains all changes
normal skin sample (21.3× haploid coverage) in the amino acid coding regions of annotated
(Glossary and Table 1). Using Affymetrix 6.0 SNP exons, consensus splice-site regions, and RNA
1060 n engl j med 361;11 nejm.org september 10, 2009
The New England Journal of Medicine
Downloaded from nejm.org at TEXAS STATE UNIV on May 17, 2013. For personal use only. No other uses without permission.
Copyright © 2009 Massachusetts Medical Society. All rights reserved.
Recurring Mutations Found by Sequencing an AML Genome
genes (including microRNA genes). Tier 2 con-
Table 1. Sequence Coverage for Tumor and Skin Genomes.*
tains changes in highly conserved regions of the
genome or regions that have regulatory poten- Variable Tumor Skin
tial. Tier 3 contains mutations in the nonrepeti- Sequencing runs — no.† 16.5 13.125
tive part of the genome that does not meet tier 2 Haploid coverage 23.3× 21.3×
criteria, and tier 4 contains mutations in the re- SNVs — no. 3,464,465 3,448,797
mainder of the genome. We tentatively identified
Concordance with dbSNP build 129 — 3,053,215 (88.1) 2,992,069 (86.8)
113 potential tier 1 mutations, 749 potential tier 2 no. (%)
mutations, 3188 potential tier 3 mutations, and
High-quality heterozygous SNPs
16,206 potential tier 4 mutations. For each of the
By array — no. 45,111 44,778
113 putative tier 1 variants, we amplified the
genomic region containing the mutation from By sequence — no. (% of array) 44,442 (98.5) 43,629 (97.4)
both tumor and skin, using a polymerase-chain- High-quality homozygous rare SNPs
reaction (PCR) assay, and performed Sanger se- By array — no. 28,295 27,735
quencing. Of the 101 variants that were called By sequence — no. (% of array) 28,252 (99.8) 27,685 (99.8)
with low confidence (the calling algorithm is
summarized in the Supplementary Appendix), * The term dbSNP denotes a National Center for Biotechnology Information
none were validated. Of the high-confidence vari- database of known DNA variants, SNP single-nucleotide polymorphism, and
SNV single-nucleotide variant.
ants, 10 of 12 were validated as somatic muta- † A single sequencing run uses all eight lanes of an Illumina flow cell (see the
tions. Similarly, we tested 178 low-confidence Glossary).
calls for tier 2, and only one was validated. In
contrast, 51 of 104 high-confidence tier 2 calls
were validated. We did not carry out validation affect the arginine residue at position 132, are
studies of variants in tiers 3 and 4. found in malignant gliomas but have not been
We also searched for somatic insertions and reported in patients with AML and are rare in
deletions (indels) using an algorithm described other tumor types.22-24 Variants of the nine other
in the Supplementary Appendix. We identified tier 1 genes are discussed in the Supplementary
142 potential somatic indels (28 deletions and 114 Appendix.
insertions). Of these variants, 119 failed valida- Each of the 10 point mutations was amplified
tion (i.e., they were falsely positive) in Sanger se- from tumor and skin samples by means of PCR,
quencing of the relevant PCR products, 21 were and the DNA species carrying the variant allele
validated but were present in both tumor and was assayed by sequencing the PCR products with
skin, and 2 were validated as somatic mutations. the use of the Illumina platform. The entire ex-
One was a 4-bp insertion in exon 12 of the NPM1 periment was replicated with amplified genomic
gene associated with aberrant cytoplasmic ex- DNA, with excellent concordance for all samples
pression of nucleophosmin (NPMc). This inser- (Fig. 3 in the Supplementary Appendix). The vari-
tion creates a frameshift mutation and a truncated ant allele frequencies of the two insertions were
protein that is known to have altered cellular determined by sequencing PCR products contain-
localization, as described previously.21 The second ing these mutations. The representation of all
mutation was a 3-bp insertion in the gene en- but two of the mutations — in chromosome 19
coding centrosomal protein 170kDa (CEP170) at open reading frame 62 (C19orf62), an unannotated
amino acid 177, predicted to result in the addi- gene of unknown function, and CEP170 — was
tion of a leucine residue at this position. approximately 50%, suggesting that all the mu-
tations were heterozygous and present in nearly
Tier 1 Mutations all the cells in the tumor sample (Fig. 2A). Ten of
The genes with tier 1 mutations and the conse- the 12 genes in tier 1 had probe sets on the Affy
quences of these mutations are summarized in metrix U133 Plus 2.0 array, and 9 of 10 were de-
Table 2, and in Table 1 in the Supplementary Ap- tectably expressed (Table 1). We also assayed ex-
pendix. Both the NPMc insertion and the NRAS pression of the 10 nonsynonymous mutant alleles
mutation have been described previously in AML by means of reverse-transcriptase PCR, using
genomes, and both are known to be relevant for amplicons designed to span introns, followed by
pathogenesis.3 Mutations in IDH1 (encoding isoc- sequencing and counting of the sequenced PCR
itrate dehydrogenase 1), which are predicted to products. Eight of the mutant alleles were detected
n engl j med 361;11 nejm.org september 10, 2009 1061
The New England Journal of Medicine
Downloaded from nejm.org at TEXAS STATE UNIV on May 17, 2013. For personal use only. No other uses without permission.
Copyright © 2009 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
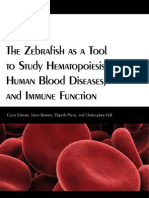
3,872,936 Tumor SNVs were detected
3,464,449 SNVs passed Maq software
SNP filter
3,377,680 SNVs were also
detected in skin
86,769 Had a somatic score above 15
66,513 Had been described
previously
20,256 Were novel potential somatic SNVs
113 Tier 1 SNVs 749 Tier 2 SNVs 3188 Tier 3 SNVs 16,206 Tier 4 SNVs
101 Were low 12 Were high 178 Were low 104 Were high 467 Were low 441 Were high 901 Were high
confidence confidence confidence confidence confidence but confidence confidence
not tested
0 Were validated 10 Were validated 1 Was validated 51 Were validated
somatic somatic somatic somatic
Figure 1. Flow Chart for Identification of Somatic Point Mutations in the Acute Myeloid Leukemia Genome.
Maq denotes Mapping and Assembly with Quality, SNP single-nucleotide
AUTHOR: Mardis polymorphism,
RETAKE and1st
SNV single-nucleotide variant.
ICM
FIGURE: 1 of 2 2nd
REG F
3rd
CASE Revised
EMail Line 4-C SIZE
at frequencies of 35 toEnon
85%.ARTIST:
However, ts for H/T
two of H/Ttionat 39p6
the 3′ end of intron 4 of C19orf62 caused
Combo
the mutations (in FREM2 and IMPG2) we did not exon 5 to be skipped (data not shown).
AUTHOR, PLEASE NOTE:
detect complementary DNA carrying the variant We then genotyped the tier 1 mutations in
Figure has been redrawn and type has been reset.
allele (although we easily detectedPlease the wild-type
check carefully. 187 additional samples from patients with AML
allele), even though each variant was present in whose clinical characteristics have been described
approximately 50% JOB: 360xx
of the tumor DNA. ISSUE: xx-xx-09
previously 26 (Table 2 in the Supplementary Appen-
The individual bases that were mutated were dix). The NPMc mutation was previously shown
highly conserved for 10 of the 12 variants, and all to be present in 43 of 180 samples (23.9%), and
but 1 were found in highly conserved regions of activating NRAS mutations were present in 17 of
the genome. The Sorting Intolerant from Tolerant 182 samples (9.3%).26 We observed mutations in
(SIFT) algorithm (which gauges the likely effect IDH1, which were predicted to cause substitution
of genic mutations on protein function) predicted of the arginine residue at position 132, in 16 of
that the mutations in NRAS, IDH1, IMPG2, and 188 samples: R132C in 8 samples, R132H in
ANKRD26 were deleterious.25 The splice-site muta- 7 samples, and R132S in 1 sample (Table 2 in the
1062 n engl j med 361;11 nejm.org september 10, 2009
The New England Journal of Medicine
Downloaded from nejm.org at TEXAS STATE UNIV on May 17, 2013. For personal use only. No other uses without permission.
Copyright © 2009 Massachusetts Medical Society. All rights reserved.
Recurring Mutations Found by Sequencing an AML Genome
Table 2. Tier 1 Mutations.*
Annotated Mutation SIFT Conservation Base Best
Gene Type Annotation Prediction Score Conservation Variant Frequency Probe†
Skin Tumor cDNA
%
CDC42 Missense S30L Tolerated 597 1 1.03 49.27 46.3 27,990
NRAS Missense G12D Deleterious 616 1 0.66 43.00 42.0 7,468
IDH1 Missense R132C Deleterious 445 1 0.81 46.06 63.9 11,400
IMPG2 Missense G834D Deleterious 472 0.018 0.67 46.22 0.4 NA
ANKRD26 Missense K1300N Deleterious 444 1 0.70 51.73 33.1 514
LTA4H Missense F107S Tolerated 539 0.946 0.68 45.28 47.9 12,138
FREM2 Missense Q2077E Tolerated 464 1 0.37 48.92 0‡ NA
C19orf62 Splice-site Exon 5-1 NA 444 1 0.27 38.71 38.8 5,021
SRRM1 Silent P691 NA 553 0.988 0.97 46.61 ND 12,858
PCDHA6 Silent A731 NA NS 0.423 0.66 49.75 ND Absent
CEP170 In-frame Codon 177 NA 513 1 0.28 28.57 52.0 15,298
insertion in-frame ins L
NPM1 Frame-shift W288fs NA 689 1 0 45.46 85.4 27,150
insertion
* The term cDNA denotes complementary DNA, ins L insertion of Leu, NA not available, ND not done, NS no score, and SIFT Sorting
Intolerant from Tolerant.
† The best probe refers to the signal value for the most highly expressed probe on the Affymetrix GeneChip Human Genome U133 Plus 2.0
array, transformed by statistical algorithms (MAS 5.0).
‡ The variant frequency was calculated from cDNA subclones.
Supplementary Appendix). The other nine muta- these tier 2 mutations had variant frequencies of
tions were not detected in the 187 additional approximately 98%, and all were located on chro-
samples. We detected no R172 mutations in IDH2 mosome X or Y. Because only a single copy of
in 188 samples (the sample from the index pa- these chromosomes was present in this male ge-
tient and the 187 additional samples), nor did we nome, the high representation of these three tier 2
observe additional mutations in any of the exons mutations was consistent with the finding that
of IDH1 or CDC42. an extremely high percentage of cells within the
A nonsynonymous acquired mutation (C328Y) bone marrow sample were part of the malignant
was found in the mitochondrial gene ND4, which clone. One mutation (chromosome 4 at position
encodes NADH dehydrogenase subunit 4, a part 128,102,994) had a variant read frequency of ap-
of complex 1 of the electron transport chain. proximately 78%, and we observed no somatic
Two of 93 additional AML samples also had non- microamplification or deletion near this variant.
synonymous mutations in this gene, but the im- Of the tier 2 mutations, 39 were present in approx-
portance of these mutations is not yet clear imately 50% of DNA species, and 9 were present
(Table 5 and the Results and Discussion section in approximately 40%. We genotyped the 52 tier 2
in the Supplementary Appendix). mutations in 187 additional AML samples and de-
tected the presence of just 1 of the mutations (on
Tier 2 Mutations chromosome 10) in 1 other AML sample, from a
We confirmed 52 mutations in tier 2. DNA seg- patient with myelomonocytic leukemia (AML-M4),
ments, each containing 1 of the 52 mutations, were which bore a translocation and did not have a
PCR-amplified from the tumor and skin samples paired normal sample (Table 2 in the Supplemen-
and sequenced to determine the proportion of DNA tary Appendix). The proportion of DNA species in
molecules carrying the mutation (Fig. 2B, and this sample that carried the mutation was 54%,
Table 4 in the Supplementary Appendix). Three of suggesting that it was heterozygous.
n engl j med 361;11 nejm.org september 10, 2009 1063
The New England Journal of Medicine
Downloaded from nejm.org at TEXAS STATE UNIV on May 17, 2013. For personal use only. No other uses without permission.
Copyright © 2009 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
detected only in patients with cytogenetic profiles
A Proportion of Variants
Tumor DNA Tumor cDNA Skin DNA
associated with intermediate risk (P<0.001).4,5
Although the patients who were analyzed in this
100
study were not treated with a single uniform pro-
tocol, outcome data were available for all 188 pa-
80
tients (Table 2 in the Supplementary Appendix).
IDH1 mutational status did not have independent
Variants (%)
60
prognostic value with respect to overall survival
40
in multivariate analysis; subgroup analysis showed
a possible adverse effect on overall survival among
20 patients with normal-karyotype AML and wild-
type NPM1, regardless of FLT3 status (Fig. 4 in
0 the Supplementary Appendix).
c
7 L
S 0L
2C
LT K13 D
FR 4H 00N
C1 Q2 S
rf6 7E
P1 P 1
96 183
35 6
73 7
69 7
29 0
2
H 2D
70 M1
60 ns
-
12 4
rs 888
rs 639
rs 615
64
2 107
4
e5
RA 3
rs 361
9o 07
AN PG R13
26 3
rs 77i
ID G1
N 42 S
02
60
D G8
Discussion
2
9
6
EM F
N
1
IM 1
KR 2
C
rs
CD
CE
Our findings support the use of an unbiased se-
quencing approach to discover previously unsus-
B Variant Frequency
pected, recurring mutations in a cancer genome.
100
Tumor With improved sequencing techniques, we covered
80
Skin this genome more completely than the first one
we sequenced (98% vs. 91% diploid coverage) and
used fewer sequencing runs (16.5 vs. 98), resulting
Variants (%)
60
in a dramatically reduced cost of data generation.
40 With better data quality and calling algorithms,
we reduced the 96% false positive frequency of
20 possible mutations for the first sequenced AML
genome to a frequency of 47% of the high-confi-
0 dence tier 1 and 2 mutations called in this genome.
Tier 1 Tier 2 Control SNPs
We predicted 1458 tumor-specific point mutations
Figure 2. Allele Frequency in Tumor DNA, Tumor Complementary DNA, with high confidence; we tested 116 of these with
and Skin DNA.ICM AUTHOR: Mardis RETAKE 1st validation sequencing and confirmed 61 of them
2nd
Panel A showsREG FIGURE: 2 of
theF percentage of 2variant alleles that were detected
3rd
in tumor (53%). Thus, this genome may contain approxi-
DNA, tumor complementary
CASE DNA (cDNA), and skin DNA for
Revised the 10 validated mately 750 somatic point mutations. We detected
nonsynonymous tier 1 somatic mutations Line in the4-Cindex patient.
SIZE For compari-
EMail
ARTIST: ts H/T H/T single-nucleotide
mutations in NRAS, NPMc, and IDH1 and a tier 2
son, variant allele
Enon frequencies are shown for six known 22p3 poly-
Combo
morphisms (SNPs). The patient was homozygous for the reference sequence mutation on chromosome 10 in more than one
AUTHOR, PLEASE
for the first two variants, heterozygous for theNOTE:
next two variants, and homozy AML genome, suggesting that these mutations
Figure has been redrawn and type has been reset.
gous for a rare SNP for the last twocheck
Please variants. Panel B shows variant allele
carefully. are not random and are probably important for
frequencies for all validated tier 1 and tier 2 mutations and the six control the pathogenesis of this tumor.
SNPs for tumor DNA and skin DNA.
JOB: 360xx ISSUE: xx-xx-09 We suggest that the 12 nonsynonymous mu-
tations are the most likely to be relevant for
Patients with the IDH1 Mutation pathogenesis, since they could potentially alter
Of the 16 patients who had AML with an IDH1 the function of expressed genes. Consistent with
R132 mutation, 13 had tumors with normal cyto- this idea and with the results of our previous
genetic profiles (of a total of 80 cytogenetically study18 is the finding that all these mutations
normal samples [16%]), 2 had trisomy 8, and were retained in the dominant clone. Surprisingly,
1 had trisomy 13. Ten of the 16 patients had AML- we found that virtually all the 52 tier 2 muta-
M1, three had AML with maturation (AML-M2), tions were also present in nearly every tumor cell
and three had AML-M4. The characteristics of in the sample, suggesting that they are also a
patients with and those without the IDH1 muta- part of the same dominant clone. However, one
tion are shown in Table 3, and in Tables 2 and 3 in cannot conclude that these mutations (or any of
the Supplementary Appendix. The mutation was the tier 3 or 4 mutations) are relevant for patho-
1064 n engl j med 361;11 nejm.org september 10, 2009
The New England Journal of Medicine
Downloaded from nejm.org at TEXAS STATE UNIV on May 17, 2013. For personal use only. No other uses without permission.
Copyright © 2009 Massachusetts Medical Society. All rights reserved.
Recurring Mutations Found by Sequencing an AML Genome
genesis simply because they are found at a high
Table 3. Characteristics of the Patients, According to IDH1 Genotype.*
frequency in the dominant clone. It is more likely
that most of these mutations are random, benign Without IDH1 With IDH1
sequence changes that existed in the hematopoi- Mutation Mutation
Variable (N = 172) (N = 16) P Value
etic cell that was transformed (i.e., they were
Age at study entry — yr 46.3±15.8 48.9±15.4 0.52†
preexisting and carried along as benign “passen-
gers,” irrelevant for pathogenesis). The finding Race — no. (%)‡ 0.88§
that the percentage of mutations found in each White 140 (81) 13 (81)
tier closely approximated the total amount of Black 14 (8) 1 (6)
DNA assayed in that tier supports this hypothe- Other 18 (10) 2 (12)
sis. Collectively, these data suggest that the vast Male sex — no. (%) 101 (59) 9 (56) 1.00§
majority of the mutations that we detected in this
Bone marrow blasts at diagnosis — % 69.3±18.1 76.7±16.4 0.12†
genome are random, background mutations in the
hematopoietic stem cell that was transformed.27 Cytogenetic profile — no. (%) 0.001§
Functional validation will be required to prove Normal 67 (39) 13 (81)
which mutations are truly important. Other 105 (61) 3 (19)
The best test of the relevance of individual Cytogenetic risk group — no./total no. (%)¶ 0.001§
mutations for pathogenesis (in the absence of Favorable 58/169 (34) 0/16
functional validation) is recurrence in other AML
Intermediate or normal 97/169 (57) 16/16 (100)
samples or other cancers. Of the 12 tier 1 muta-
Poor 14/169 (8) 0/16
tions, 3 (occurring in NPM1, NRAS, and IDH1)
were recurrent in patients with AML and there- AML-M3 subtype — no. (%) 40 (23) 0/16 0.03§
fore were likely to be important in the pathogen- Underwent transplantation — no. (%) 27 (16) 3 (19) 0.72§
esis of this tumor. R132 mutations in the IDH1 Mutation — no. (%)
gene had not previously been detected in the 45 NPM1 36 (21) 7 (44) 0.06§
patients with AML who were tested23 and are de- FLT3
tected only rarely in tumor types other than ma-
Internal tandem duplication 36 (21) 4 (25) 0.75§
lignant gliomas.22,24 The IDH1 R132H, C, and
D835 10 (6) 1 (6) 1.00§
S mutations dramatically reduce the catalytic ac-
tivity of the IDH1 enzyme; it has been suggested RAS 19 (11) 1 (6) 1.00§
that IDH1 is a tumor suppressor that is inacti-
* Plus–minus values are means ±SD. Percentages may not total 100 because of
vated by dominant mutations in R132.28 There rounding. AML-M3 denotes acute promyelocytic leukemia, FLT3 FMS-related
are significant differences, however, between the tyrosine kinase 3, and IDH1 isocitrate dehydrogenase 1.
IDH1 mutations found in gliomas and those in † The P value was calculated with the use of the two-sided t-test.
‡ Race was self-reported.
AML. We detected the R132C mutation in 8 of 16 § The P value was calculated with the use of Fisher’s exact test.
patients with AML who carried an IDH1 muta- ¶ The definitions for cytogenetic risk groups are from the Medical Research
tion (50%). In contrast, the mutation was report Council and the Cancer and Leukemia Group B.4,5 Adequate cytogenetic data
were not available for 3 of the 172 patients who did not have an IDH1 mutation.
ed in only 7 of 161 patients with gliomas (4%,
P<0.001 by Fisher’s exact test). The most com-
mon mutation in gliomas (R132H) was detected in most AML genomes is similar to the number
in 142 of 161 patients (88%) but in only 7 of 16 in the first 2 patients we studied (approximately
patients with AML (44%, P = 0.13). When the 750), the likelihood that 2 of 188 patients will
R132H mutation was overexpressed in a glioblas- carry an identical mutation at the same position
toma cell line, induction of messenger RNAs for in the genome is extremely small (1.1×10−9). This
several target genes of hypoxia-inducible factor suggests that the tier 2 somatic mutation at po-
1α (HIF1α) was detected (GLUT1, VEGF, and PGK1).28 sition 108,115,590 of chromosome 10 is unlikely
However, in 13 patients with AML — 5 with to be a random event. It falls in a conserved re-
R132H and 8 with R132C — there were no sig- gion with regulatory potential, and its detection
nificant alterations in the expression of any of in a second patient with AML suggests that this
these genes (Fig. 3 in the Supplementary Ap- region may contribute to pathogenesis through
pendix). a novel mechanism that remains to be defined.
Assuming that the number of point mutations Although the potential of next-generation se-
n engl j med 361;11 nejm.org september 10, 2009 1065
The New England Journal of Medicine
Downloaded from nejm.org at TEXAS STATE UNIV on May 17, 2013. For personal use only. No other uses without permission.
Copyright © 2009 Massachusetts Medical Society. All rights reserved.
Recurring Mutations Found by Sequencing an AML Genome
quencing platforms for uncovering the genetic from Genzyme. No other potential conflict of interest relevant
to this article was reported.
rules of cancer is great, the sequencing of thou- We thank Jennifer Ivanovich for obtaining the detailed family
sands of additional cancer genomes will be re- histories of the patients; Nancy Reidelberger for administrative
quired to fully unravel this complex and hetero- support; Dr. Rob Culverhouse for statistical support; Todd Hepler,
William Schroeder, Justin Lolofie, Scott Abbott, Shawn Leonard,
geneous disease.29,30 Ken Swanson, Indraniel Das, and Michael Kiwala for their con-
tributions to the Laboratory Information Management System;
Supported by grants from the National Institutes of Health Gary Stiehr, Richard Wohlstadter, Matt Weil, and Kelly Fallon for
(PO1-CA101937, to Dr. Ley; and U54-HG003079, to Dr. Wilson) information-technology support; Drs. Clara Bloomfield, Michael
and the Barnes–Jewish Hospital Foundation (00335-0505-01, to Caligiuri, and James Vardiman for providing the AML samples
Dr. Ley). from the Cancer and Leukemia Group B Leukemia Bank; the
Dr. Westervelt reports receiving lecture fees from Celgene and nursing staff of the Siteman Cancer Center and Barnes–Jewish
Novartis; and Dr. DiPersio, receiving consulting and lecture fees Hospital; and all the patients who participated in the study.
References
1. Song WJ, Sullivan MG, Legare RD, et 10. Bullinger L, Döhner K, Bair E, et al. acute myeloid leukaemia genome. Nature
al. Haploinsufficiency of CBFA2 causes Use of gene-expression profiling to iden- 2008;456:66-72.
familial thrombocytopenia with propen- tify prognostic subclasses in adult acute 19. Bentley DR, Balasubramanian S, Swerd
sity to develop acute myelogenous leukae- myeloid leukemia. N Engl J Med 2004;350: low HP, et al. Accurate whole human ge-
mia. Nat Genet 1999;23:166-75. 1605-16. nome sequencing using reversible termi-
2. Owen C, Barnett M, Fitzgibbon J. Fa- 11. Valk PJ, Verhaak RG, Beijen MA, et al. nator chemistry. Nature 2008;456:53-9.
milial myelodysplasia and acute myeloid Prognostically useful gene-expression pro- 20. Li H, Ruan J, Durbin R. Mapping short
leukaemia — a review. Br J Haematol files in acute myeloid leukemia. N Engl J DNA sequencing reads and calling variants
2008;140:123-32. Med 2004;350:1617-28. using mapping quality scores. Genome
3. Schlenk RF, Döohner K, Krauter J, et 12. Baldus CD, Mrózek K, Marcucci G, Res 2008;18:1851-8.
al. Mutations and treatment outcome in Bloomfield CD. Clinical outcome of de 21. Falini B, Mecucci C, Tiacci E, et al.
cytogenetically normal acute myeloid leu- novo acute myeloid leukaemia patients Cytoplasmic nucleophosmin in acute myel-
kemia. N Engl J Med 2008;358:1909-18. with normal cytogenetics is affected ogenous leukemia with a normal karyo-
4. Byrd JC, Mrózek K, Dodge RK, et al. by molecular genetic alterations: a con- type. N Engl J Med 2005;352:254-66. [Er-
Pretreatment cytogenetic abnormalities cise review. Br J Haematol 2007;137:387- ratum, N Engl J Med 2005;352:740.]
are predictive of induction success, cumu- 400. 22. Bleeker FE, Lamba S, Leenstra S, et
lative incidence of relapse, and overall 13. Heuser M, Beutel G, Krauter J, et al. al. IDH1 mutations at residue p.R132
survival in adult patients with de novo High meningioma 1 (MN1) expression as (IDH1(R132)) occur frequently in high-
acute myeloid leukemia: results from Can- a predictor for poor outcome in acute my- grade gliomas but not in other solid tu-
cer and Leukemia Group B (CALGB 8461). eloid leukemia with normal cytogenetics. mors. Hum Mutat 2009;30:7-11.
Blood 2002;100:4325-36. Blood 2006;108:3898-905. 23. Yan H, Parsons DW, Jin G, et al. IDH1
5. Grimwade D, Walker H, Harrison G, 14. Langer C, Radmacher MD, Ruppert AS, and IDH2 mutations in gliomas. N Engl J
et al. The predictive value of hierarchical et al. High BAALC expression associates Med 2009;360:765-73.
cytogenetic classification in older adults with other molecular prognostic markers, 24. Kang MR, Kim MS, Oh JE, et al. Muta-
with acute myeloid leukemia (AML): analy- poor outcome, and a distinct gene-expres- tional analysis of IDH1 codon 132 in glio-
sis of 1065 patients entered into the United sion signature in cytogenetically normal blastomas and other common cancers.
Kingdom Medical Research Council AML11 patients younger than 60 years with acute Int J Cancer 2009;125:353-5.
trial. Blood 2001;98:1312-20. myeloid leukemia: a Cancer and Leukemia 25. Ng PC, Henikoff S. Accounting for hu-
6. Rücker FG, Bullinger L, Schwaenen C, Group B (CALGB) study. Blood 2008;111: man polymorphisms predicted to affect pro
et al. Disclosure of candidate genes in 5371-9. tein function. Genome Res 2002;12:436-46.
acute myeloid leukemia with complex 15. Lugthart S, van Drunen E, van Norden 26. Link DC, Kunter G, Kasai Y, et al. Dis-
karyotypes using microarray-based molec- Y, et al. High EVI1 levels predict adverse tinct patterns of mutations occurring in
ular characterization. J Clin Oncol 2006; outcome in acute myeloid leukemia: prev- de novo AML versus AML arising in the
24:3887-94. alence of EVI1 overexpression and chro- setting of severe congenital neutropenia.
7. Suela J, Alvarez S, Cifuentes F, et al. mosome 3q26 abnormalities underesti- Blood 2007;110:1648-55.
DNA profiling analysis of 100 consecutive mated. Blood 2008;111:4329-37. 27. Sjöblom T, Jones S, Wood LD, et al.
de novo acute myeloid leukemia cases re- 16. Marcucci G, Maharry K, Whitman SP, The consensus coding sequences of hu-
veals patterns of genomic instability that et al. High expression levels of the ETS- man breast and colorectal cancers. Science
affect all cytogenetic risk groups. Leuke- related gene, ERG, predict adverse out- 2006;314:268-74.
mia 2007;21:1224-31. come and improve molecular risk-based 28. Zhao S, Lin Y, Xu W, et al. Glioma-
8. Tyybäkinoja A, Elonen E, Piippo K, classification of cytogenetically normal derived mutations in IDH1 dominantly
Porkka K, Knuutila S. Oligonucleotide acute myeloid leukemia: a Cancer and Leu- inhibit IDH1 catalytic activity and induce
array-CGH reveals cryptic gene copy num- kemia Group B study. J Clin Oncol 2007; HIF-1alpha. Science 2009;324:261-5.
ber alterations in karyotypically normal 25:3337-43. 29. Dulbecco R. A turning point in cancer
acute myeloid leukemia. Leukemia 2007; 17. Pratz K, Levis M. Incorporating FLT3 research: sequencing the human genome.
21:571-4. inhibitors into acute myeloid leukemia Science 1986;231:1055-6.
9. Walter MJ, Payton JE, Ries RE, et al. treatment regimens. Leuk Lymphoma 30. Stratton MR, Campbell PJ, Futreal PA.
Acquired copy number alterations in adult 2008;49:852-63. The cancer genome. Nature 2009;458:719-
acute myeloid leukemia genomes. Proc 18. Ley TJ, Mardis ER, Ding L, et al. DNA 24.
Natl Acad Sci U S A (in press). sequencing of a cytogenetically normal Copyright © 2009 Massachusetts Medical Society.
1066 n engl j med 361;11 nejm.org september 10, 2009
The New England Journal of Medicine
Downloaded from nejm.org at TEXAS STATE UNIV on May 17, 2013. For personal use only. No other uses without permission.
Copyright © 2009 Massachusetts Medical Society. All rights reserved.
You might also like
- Pedigree Chart WorksheetDocument72 pagesPedigree Chart Worksheetapi-3075658820% (1)
- Genome Sequencing As An Alternative To Cytogenetic Analysis in Myeloid CancersDocument12 pagesGenome Sequencing As An Alternative To Cytogenetic Analysis in Myeloid CancersJck YyNo ratings yet
- Age-Related Clonal HematopoiesisDocument11 pagesAge-Related Clonal HematopoiesisgiulioNo ratings yet
- 2013 Clinical WES Nejmoa1306555Document10 pages2013 Clinical WES Nejmoa1306555MCuk2606No ratings yet
- SF3B1 and Other Novel Cancer Genes: in Chronic Lymphocytic LeukemiaDocument10 pagesSF3B1 and Other Novel Cancer Genes: in Chronic Lymphocytic LeukemiaRafael ColinaNo ratings yet
- Cancer Research Review PDFDocument57 pagesCancer Research Review PDFCiocan AlexandraNo ratings yet
- Mesenchymal Stem Cells Literature ReviewDocument9 pagesMesenchymal Stem Cells Literature ReviewafdtygyhkNo ratings yet
- Detection of Mutations in EGFR in Circulating Lung-Cancer Cells.Document12 pagesDetection of Mutations in EGFR in Circulating Lung-Cancer Cells.Joonseok ParkNo ratings yet
- Variant of TYR and Autoimmunity Susceptibility Loci in Generalized VitiligoDocument12 pagesVariant of TYR and Autoimmunity Susceptibility Loci in Generalized VitiligoIvo AfianiNo ratings yet
- A Switch in Time Through Genes Aligned Unraveling The Geno - 2020 - Cell StemDocument3 pagesA Switch in Time Through Genes Aligned Unraveling The Geno - 2020 - Cell StemBandar Ternama XBNo ratings yet
- Aula LogisticaDocument64 pagesAula LogisticaglaucomassotoNo ratings yet
- Chromosomal Microarray Versus Karyotyping For Prenatal Diagnosis - 2012Document10 pagesChromosomal Microarray Versus Karyotyping For Prenatal Diagnosis - 2012George CarvalhoNo ratings yet
- Libro de InmunohematologiaDocument44 pagesLibro de InmunohematologiaMijael Edgar Guadalupe MagnoNo ratings yet
- Postdoc Position in David Chen Lab at City of HopeDocument2 pagesPostdoc Position in David Chen Lab at City of HopeAdolfo De La Rosa JrNo ratings yet
- Radiation-Induced Bystander Effects - Implications For Cancer - Mothersill and Seymour, 2004Document8 pagesRadiation-Induced Bystander Effects - Implications For Cancer - Mothersill and Seymour, 2004Isabella LiedtkeNo ratings yet
- CMT WEGS Nejmoa0908094Document11 pagesCMT WEGS Nejmoa0908094MCuk2606No ratings yet
- Wyandt2017 Book HumanChromosomeVariationHeteroDocument500 pagesWyandt2017 Book HumanChromosomeVariationHeteroRicardo OlguinNo ratings yet
- Lapun: ImashukuDocument2 pagesLapun: ImashukuApsopela SandiveraNo ratings yet
- This Content Downloaded From 88.231.62.252 On Tue, 25 Apr 2023 09:08:44 UTCDocument8 pagesThis Content Downloaded From 88.231.62.252 On Tue, 25 Apr 2023 09:08:44 UTCMaman AhmadNo ratings yet
- Stem Cell Cancer: By: Monali.R.Bhakta Sem: 8 Roll No: 86Document13 pagesStem Cell Cancer: By: Monali.R.Bhakta Sem: 8 Roll No: 86coolharsh111No ratings yet
- References: Department of Pharmaceutical Sciences, Kumaun UniversityDocument3 pagesReferences: Department of Pharmaceutical Sciences, Kumaun Universityhemajoshi4517No ratings yet
- Zheng Hong 郑 红 Department of Medical Genetics & Cell BiologyDocument63 pagesZheng Hong 郑 红 Department of Medical Genetics & Cell BiologyinakiNo ratings yet
- BloodDocument145 pagesBloodRanintha Surbakti100% (2)
- Stem Cells and Cancer Stem Cells, Volume 3 - Stem Cells and Cancer Stem Cells, Therapeutic Applications in Disease and Injury - Volume 3Document426 pagesStem Cells and Cancer Stem Cells, Volume 3 - Stem Cells and Cancer Stem Cells, Therapeutic Applications in Disease and Injury - Volume 3Artan100% (1)
- Tumor Cell Intrinsic FactorsDocument24 pagesTumor Cell Intrinsic FactorsBanh Ti HonNo ratings yet
- Lee Eun JooDocument344 pagesLee Eun JooDana GoldoniNo ratings yet
- Lehmann Werman 2016Document9 pagesLehmann Werman 2016Felipe MNo ratings yet
- Nej Mo A 1516767Document11 pagesNej Mo A 1516767mayrapp16No ratings yet
- NEJMoa 1700554Document9 pagesNEJMoa 1700554Titi OrellanaNo ratings yet
- Wallace 20131Document48 pagesWallace 20131DCPNo ratings yet
- Glioblastoma Cells Through An ERK-dependent Pathway, Oncol. Rep., 28: 41-48Document1 pageGlioblastoma Cells Through An ERK-dependent Pathway, Oncol. Rep., 28: 41-48ilssNo ratings yet
- NCI60 Target RefsDocument6 pagesNCI60 Target RefsDioxelis LópezNo ratings yet
- NIH Public AccessDocument20 pagesNIH Public Accessaaasim93No ratings yet
- ReferencesDocument4 pagesReferencesfidabimeeNo ratings yet
- Integrative Multi-Omic Cancer Profiling Reveals DNA Methylation Patterns Associated With Therapeutic Vulnerability and Cell-Of-OriginDocument42 pagesIntegrative Multi-Omic Cancer Profiling Reveals DNA Methylation Patterns Associated With Therapeutic Vulnerability and Cell-Of-Origin戴义宾No ratings yet
- Stem Cell ReportDocument2 pagesStem Cell Reporttaleenwas2No ratings yet
- Oncogenic CSF3R Mutations in Chronic Neutrophilic Leukemia and Atypical CMLDocument1 pageOncogenic CSF3R Mutations in Chronic Neutrophilic Leukemia and Atypical CMLSav GaNo ratings yet
- XMRK in MedakaDocument4 pagesXMRK in Medakaxiaozi92No ratings yet
- Melanoma With Striking Adenocarcinomatous DifferentiationHUMANSDocument11 pagesMelanoma With Striking Adenocarcinomatous DifferentiationHUMANSgranulomatous pneumoniaNo ratings yet
- Germline Mutations in Predisposition Genes in Pediatric CancerDocument11 pagesGermline Mutations in Predisposition Genes in Pediatric CancerGuadalupeA.OsorioNo ratings yet
- (2983) of Double Esterase in Bone Marrow Cells of Patients WithDocument2 pages(2983) of Double Esterase in Bone Marrow Cells of Patients WithApsopela SandiveraNo ratings yet
- JurnalDocument3 pagesJurnalnurlaras201102No ratings yet
- Genomic Instability in CancerDocument17 pagesGenomic Instability in Cancerhibahussain74305No ratings yet
- Colorectal Cancer in StoolDocument8 pagesColorectal Cancer in StoolAnmol KumarNo ratings yet
- Ata Ur Rehman: Research Proposal For PHD AdmissionDocument5 pagesAta Ur Rehman: Research Proposal For PHD AdmissionSajjad AliNo ratings yet
- The Cell Biological Basis of Cancer - ThesisDocument50 pagesThe Cell Biological Basis of Cancer - ThesisRamesh MahakurNo ratings yet
- Thorsson 2018 Immune Landscape of CancerDocument34 pagesThorsson 2018 Immune Landscape of Cancershivi misraNo ratings yet
- Cancer EpigeneticsDocument18 pagesCancer EpigeneticsIrfan AlviNo ratings yet
- JurnalDocument5 pagesJurnalNers A 2016No ratings yet
- Corrections: Neuroscience. Cell BiologyDocument8 pagesCorrections: Neuroscience. Cell BiologySammer BurgosNo ratings yet
- The Disruption of Profiling of Serotonergic Neurons, Results in Autism-Related BehaviorsDocument22 pagesThe Disruption of Profiling of Serotonergic Neurons, Results in Autism-Related BehaviorsAngelinni Taglioni StangeNo ratings yet
- GenomiclibraryDocument2 pagesGenomiclibraryJonathan AlanizNo ratings yet
- Microenvironment Drives Cell State, Plasticity, and Drug Response in Pancreatic CancerDocument46 pagesMicroenvironment Drives Cell State, Plasticity, and Drug Response in Pancreatic Cancerka1400ra-sNo ratings yet
- Guangbin Luo-Curriculum VitaeDocument6 pagesGuangbin Luo-Curriculum Vitaeluol35No ratings yet
- This Content Downloaded From 120.126.70.24 On Wed, 29 Mar 2023 11:59:10 UTCDocument8 pagesThis Content Downloaded From 120.126.70.24 On Wed, 29 Mar 2023 11:59:10 UTCmarcia suNo ratings yet
- Phipps Solitary Fibrous Tumors of The Pleura Results of Surgical Treatment 2009Document13 pagesPhipps Solitary Fibrous Tumors of The Pleura Results of Surgical Treatment 2009JZNo ratings yet
- Lynch SyndromeDocument6 pagesLynch SyndromeduminduNo ratings yet
- 2002 DavidsonDocument5 pages2002 DavidsonBianca PapadopolNo ratings yet
- Majalah Kedokteran Atmajaya, 2 (2) : Halaman 85-96: WWW - LeukemiaDocument0 pagesMajalah Kedokteran Atmajaya, 2 (2) : Halaman 85-96: WWW - LeukemiaHasan Ibn MutholibNo ratings yet
- Daftar PustakaDocument6 pagesDaftar PustakaMerliana DebyantiNo ratings yet
- The Bethesda System for Reporting Thyroid Cytopathology: Definitions, Criteria and Explanatory NotesFrom EverandThe Bethesda System for Reporting Thyroid Cytopathology: Definitions, Criteria and Explanatory NotesNo ratings yet
- Population-Based Incremental LearningDocument3 pagesPopulation-Based Incremental Learningemma698No ratings yet
- Brosur KIT HPV DNADocument2 pagesBrosur KIT HPV DNARonna EfriyanaNo ratings yet
- Cloning Dolly & MicromanipulationDocument29 pagesCloning Dolly & Micromanipulationnitinyadav16No ratings yet
- Meiosis LabDocument9 pagesMeiosis Labpeter103958No ratings yet
- 13-1: The Genetic Material: Frederick Griffith's Experiment - TransformationDocument7 pages13-1: The Genetic Material: Frederick Griffith's Experiment - Transformationapi-233187566No ratings yet
- Chapter 8.4-8.7 Study GuideDocument5 pagesChapter 8.4-8.7 Study GuideHomerNo ratings yet
- PGT & TGT (Biology) SyllabusDocument7 pagesPGT & TGT (Biology) SyllabusNikkisonuNo ratings yet
- Ronda2019 SupDocument31 pagesRonda2019 SupEmna BouhajjaNo ratings yet
- Trancriptome and Proteome AnalysisDocument68 pagesTrancriptome and Proteome AnalysisNeeru RedhuNo ratings yet
- Flowering Pathway in Arabidopsis-CouplandDocument3 pagesFlowering Pathway in Arabidopsis-CouplandJay Prakash MauryaNo ratings yet
- 2023 Article 1738Document19 pages2023 Article 1738Murillo Pyaia Alves PaixãoNo ratings yet
- RESEARCH PaperDocument6 pagesRESEARCH PaperLlana ToribioNo ratings yet
- Grade 12 Biology Mechanisms of InheritanceDocument22 pagesGrade 12 Biology Mechanisms of Inheritanceapi-635512040No ratings yet
- Molecular Markers and Their Applicationsin CattleDocument5 pagesMolecular Markers and Their Applicationsin CattleDEEPANKER BISHTNo ratings yet
- CSI Wildlife: Analyzing Genetic EvidenceDocument4 pagesCSI Wildlife: Analyzing Genetic EvidenceInsaf MNo ratings yet
- La Biología de La Cromatina Complejos de Remodelación: FurtherDocument24 pagesLa Biología de La Cromatina Complejos de Remodelación: FurtherVíc AltamarNo ratings yet
- ATP 2023-24 GR 12 Life SciDocument4 pagesATP 2023-24 GR 12 Life SciPfarelo TshidzumbaNo ratings yet
- hssb0800t StudygdbDocument17 pageshssb0800t StudygdbyawahabNo ratings yet
- Liu2011 PDFDocument6 pagesLiu2011 PDFAnonymous cUzAJWocPCNo ratings yet
- Meiosis: Chromatids (The Two Halves of A Duplicated Chromosome), As inDocument29 pagesMeiosis: Chromatids (The Two Halves of A Duplicated Chromosome), As inyamamaNo ratings yet
- CITOSISDocument3 pagesCITOSISKylliíanNo ratings yet
- Types of MutationsDocument43 pagesTypes of MutationsElyNo ratings yet
- Molecular Cell Biology (Chapter 25 - Cancer)Document42 pagesMolecular Cell Biology (Chapter 25 - Cancer)qwertyNo ratings yet
- Articulo MacacosDocument15 pagesArticulo MacacosAdolfo Mora SanchezNo ratings yet
- 15.1 History of Evolutionary ThoughtDocument11 pages15.1 History of Evolutionary ThoughtlutimoNo ratings yet
- Mutation and Sickle CellDocument16 pagesMutation and Sickle Cellapi-309893409No ratings yet
- Biotechnology and Its Applications: Pre-Medical: Biology AllenDocument5 pagesBiotechnology and Its Applications: Pre-Medical: Biology AllenJK JHANo ratings yet
- ARECA ThesisDocument32 pagesARECA ThesisMdkhurshed AlamNo ratings yet
- Biotechnology SyllabusDocument111 pagesBiotechnology SyllabusSatyam SinghNo ratings yet