Download as pdf or txt
You might also like
- Embryology ReviewerDocument52 pagesEmbryology ReviewerAngela Nicole ManasNo ratings yet
- Heart FailureDocument44 pagesHeart FailureSalman Habeeb100% (7)
- EdemaDocument26 pagesEdemaNyco100% (2)
- Case Study: Congestive Heart FailureDocument7 pagesCase Study: Congestive Heart FailureXI-E / 21 / MARY TRIANANo ratings yet
- CHFDocument33 pagesCHFsebghatullah mubarezNo ratings yet
- Pediatric Test 2Document28 pagesPediatric Test 2Nurse JonesNo ratings yet
- Heart Failure: Zelalem T., MD Yr III Resident, PediatricsDocument65 pagesHeart Failure: Zelalem T., MD Yr III Resident, PediatricsChalie MequanentNo ratings yet
- Midterm PRT 2aDocument24 pagesMidterm PRT 2aReysel MonteroNo ratings yet
- Final Exam NotesDocument24 pagesFinal Exam NotesNicholeGarcesCisnerosNo ratings yet
- NSG124 - Pedia Written ReportDocument12 pagesNSG124 - Pedia Written Reportlaurie.charlynjaneNo ratings yet
- Heart Failure PharmacyDocument47 pagesHeart Failure PharmacyKhashayar MastooriNo ratings yet
- 9, CHF BestDocument43 pages9, CHF BestauNo ratings yet
- Cardiac DiseasesDocument8 pagesCardiac DiseasesTJ NgNo ratings yet
- Heart Failure PAED 604 2023 VileshDocument34 pagesHeart Failure PAED 604 2023 VileshAvneelNo ratings yet
- Heart Failure: Scott Kaba MatafwaliDocument25 pagesHeart Failure: Scott Kaba MatafwaliAngetile KasangaNo ratings yet
- Cardiovascular Disorders 2Document78 pagesCardiovascular Disorders 2Erlinda SagadsadNo ratings yet
- Disturbances in CirculationDocument10 pagesDisturbances in CirculationSHERIE ANNE BERNABENo ratings yet
- Obstetrical Anesthesia: ObjectivesDocument10 pagesObstetrical Anesthesia: ObjectivesIsabel CastilloNo ratings yet
- CardiacDocument3 pagesCardiacKami SookramNo ratings yet
- Congestive Heart FailureDocument14 pagesCongestive Heart FailureRooben LallNo ratings yet
- Congenital Heart DefectsDocument45 pagesCongenital Heart Defectskathylaine100% (1)
- Heart FailureDocument4 pagesHeart FailureDane WrightNo ratings yet
- Midterm PRT 2 A qq9Document33 pagesMidterm PRT 2 A qq9Reysel MonteroNo ratings yet
- Acynotic DiseaseDocument55 pagesAcynotic DiseaseTesfamichael AbathunNo ratings yet
- Asuhan Keperawatan Pada Pasien Dengan Hipertensi Susilawati, M. Kep. Ns. Sp. Kep. MBDocument77 pagesAsuhan Keperawatan Pada Pasien Dengan Hipertensi Susilawati, M. Kep. Ns. Sp. Kep. MBChipot NoviNo ratings yet
- L8 9 Cardiac Fluids Disorders in ChildrenDocument17 pagesL8 9 Cardiac Fluids Disorders in ChildrenRose Anne AbivaNo ratings yet
- Heart Failure: Andi Wahjono Adi, MD, FIHADocument46 pagesHeart Failure: Andi Wahjono Adi, MD, FIHAYuanita WahyuningsihNo ratings yet
- FE Enrichment 2024Document4 pagesFE Enrichment 2024tarahggggNo ratings yet
- Heart Failure: Presented By: Leslie PaguioDocument38 pagesHeart Failure: Presented By: Leslie PaguioLeslie PaguioNo ratings yet
- Cardiovascular DiseasesDocument4 pagesCardiovascular DiseasesAshley Nicole LimNo ratings yet
- Congenital Heart Defect EDITDocument57 pagesCongenital Heart Defect EDITnicholasacquah680No ratings yet
- Cardiovascular DisorderDocument40 pagesCardiovascular DisorderAmy Del CarmenNo ratings yet
- CME Cyanotic Heart DiseaseDocument38 pagesCME Cyanotic Heart DiseaseTan Zhi HongNo ratings yet
- MCN PihDocument4 pagesMCN PihBSN 1-N CASTRO, RicciNo ratings yet
- Hemodialysis Fact SheetDocument4 pagesHemodialysis Fact SheetGelo BallartaNo ratings yet
- AntihypertensivesDocument32 pagesAntihypertensivesJianne CaloNo ratings yet
- Reading Assignment: Read, Understand & Prepare Concept Maps ForDocument4 pagesReading Assignment: Read, Understand & Prepare Concept Maps ForrubyNo ratings yet
- Pediatric Cardiology: Betsy Johnson, MSN, CPNP-PC Aya Rahav, MS, RN, CPNDocument90 pagesPediatric Cardiology: Betsy Johnson, MSN, CPNP-PC Aya Rahav, MS, RN, CPNGelsey Gelsinator JianNo ratings yet
- CN 118 - Lecture ReviewerDocument40 pagesCN 118 - Lecture ReviewerCamille SanguyoNo ratings yet
- Acute Biologic CrisisDocument60 pagesAcute Biologic Crisisraidis100% (4)
- Valvular Heart Disease. KulDocument60 pagesValvular Heart Disease. KulIntan Kumalasari RambeNo ratings yet
- Lecture 12 Cardio Intensive CasesDocument32 pagesLecture 12 Cardio Intensive Casesraul0% (1)
- Cardiovascular DiseaseDocument5 pagesCardiovascular DiseaseLizeil VelardeNo ratings yet
- Derupe-IV FluidsDocument5 pagesDerupe-IV FluidsEllamae DerupeNo ratings yet
- Pre Gestational 1Document12 pagesPre Gestational 1Fatima TañedoNo ratings yet
- Hypertension PathoDocument13 pagesHypertension Pathowajehak40No ratings yet
- Nursing Care Plan: Thyroid HormonesDocument3 pagesNursing Care Plan: Thyroid HormonesShenaNo ratings yet
- Heart Failure Ncm106Document4 pagesHeart Failure Ncm106KeThSantibanNo ratings yet
- (OSCE) 3.0 Cardiovascular ExaminationDocument5 pages(OSCE) 3.0 Cardiovascular ExaminationJara RogacionNo ratings yet
- MS Quiz ReviewerDocument6 pagesMS Quiz ReviewerAndrea PayumoNo ratings yet
- Unit 7 Cardiac (S)Document78 pagesUnit 7 Cardiac (S)Cheyenne SchimpfNo ratings yet
- Altered Level of Consciousness (Ms Mark)Document5 pagesAltered Level of Consciousness (Ms Mark)Cristelle Joy RebocaNo ratings yet
- CHAP20Document5 pagesCHAP20syroise margauxNo ratings yet
- Pharmacologic Management of HypertensionDocument8 pagesPharmacologic Management of HypertensionL2 - MAKILALA, Zion joy B.No ratings yet
- 5,6.heart FailureDocument12 pages5,6.heart FailureKUMUTHA MALAR A/P PARMESWARANNo ratings yet
- Week 3 Clinical ResearchDocument15 pagesWeek 3 Clinical ResearchkatiegracemcleodNo ratings yet
- LTC CHF Case PresentationDocument8 pagesLTC CHF Case Presentationapi-650480818No ratings yet
- Case Presentation: Congenital Heart DiseaseDocument37 pagesCase Presentation: Congenital Heart DiseaseKarin Nadia UtamiNo ratings yet
- Pedia AbnormalDocument34 pagesPedia Abnormallight_tyrNo ratings yet
- The Ideal Heart Healthy Diet Cookbook; The Superb Diet Guide To Lower Your Blood Pressure And Cholesterol Levels With Nutritious Low Sodium Low Fat RecipesFrom EverandThe Ideal Heart Healthy Diet Cookbook; The Superb Diet Guide To Lower Your Blood Pressure And Cholesterol Levels With Nutritious Low Sodium Low Fat RecipesNo ratings yet
- Sources of Demographic Data: Demography Vital and Health StatisticsDocument3 pagesSources of Demographic Data: Demography Vital and Health Statisticsayowna.524No ratings yet
- Chapter 10Document2 pagesChapter 10ayowna.524No ratings yet
- Neurologic DisordersDocument8 pagesNeurologic Disordersayowna.524No ratings yet
- MATERNALDocument3 pagesMATERNALayowna.524No ratings yet
- WrightPanksepp NPSA 2012Document73 pagesWrightPanksepp NPSA 2012Tim PetersonNo ratings yet
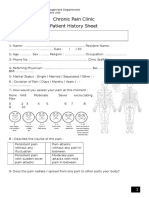
- Chronic Pain Clinic Patient History SheetDocument4 pagesChronic Pain Clinic Patient History SheetBelal N. MahfouzNo ratings yet
- 60 Samples Questions and Answers For MRCOphth IDocument26 pages60 Samples Questions and Answers For MRCOphth Imacheso0% (1)
- Flow Sheet TemplateDocument4 pagesFlow Sheet TemplateIulia Tania AndronacheNo ratings yet
- Table of Epithelia of Human OrgansDocument3 pagesTable of Epithelia of Human OrgansDr-Atin Kumar SrivastavaNo ratings yet
- Essay On ProteinDocument2 pagesEssay On ProteinLester MendigoriaNo ratings yet
- Vet Flash CardsDocument13 pagesVet Flash CardsgraysonvetscienceNo ratings yet
- Name - Date - Urinary System and Excretion WebquestDocument4 pagesName - Date - Urinary System and Excretion WebquestAmanda IrvingNo ratings yet
- Worksheet 1 Respiration and Breathing AnswersDocument3 pagesWorksheet 1 Respiration and Breathing AnswersL NarineNo ratings yet
- Anatomy Lecture Notes DigestiveDocument9 pagesAnatomy Lecture Notes DigestiveKenneth dela CruzNo ratings yet
- Hukin 72 069Document10 pagesHukin 72 069Sarah OctaviaNo ratings yet
- Alimentary System WritingDocument2 pagesAlimentary System WritingIsis Marian Rodriguez JaramilloNo ratings yet
- Chapter 1 - The Nervous SystemDocument8 pagesChapter 1 - The Nervous SystemRadha RamineniNo ratings yet
- The Swinging Flashlight Test: Learning Objective: Facts About The PupilDocument3 pagesThe Swinging Flashlight Test: Learning Objective: Facts About The Pupilsiti hazard aldinaNo ratings yet
- Kabilyte FinalDocument42 pagesKabilyte Finaldrchelluri100% (1)
- Emotional IntelligenceDocument152 pagesEmotional IntelligenceSofiene Guedri100% (2)
- Portal HypertensionDocument60 pagesPortal HypertensionParul VarshneyNo ratings yet
- M. Rizano Priatmoko Alvin Julian R. Dhimas Andianto M. Farrell Hidayat Rainanda MuhammadDocument36 pagesM. Rizano Priatmoko Alvin Julian R. Dhimas Andianto M. Farrell Hidayat Rainanda MuhammadfrlolNo ratings yet
- Jss1 Basic ScienceDocument9 pagesJss1 Basic SciencevbestNo ratings yet
- KZ Midwifery Ratio 2014Document71 pagesKZ Midwifery Ratio 2014KZNo ratings yet
- Design For ComfortDocument50 pagesDesign For ComfortPai Lang ZhenNo ratings yet
- PneumoniaDocument41 pagesPneumoniapaanar100% (2)
- Enzymic Method For Quantitative Determination of Nanogram Amounts of Total and Oxidized GlutathioneDocument21 pagesEnzymic Method For Quantitative Determination of Nanogram Amounts of Total and Oxidized GlutathioneJosué Velázquez100% (1)
- Types of SphygmomanometerDocument2 pagesTypes of SphygmomanometerBea AbesamisNo ratings yet
- Central DogmaDocument50 pagesCentral DogmaIvilyn ManguladNo ratings yet
- Annelid ADocument52 pagesAnnelid AMohammad Sharifuddin SallehNo ratings yet
- Beyond HypnagogiaDocument72 pagesBeyond HypnagogiaMarko Markaba100% (1)
- Drug Study (Cervical Polyp)Document4 pagesDrug Study (Cervical Polyp)aerondominicbasilioNo ratings yet
- Children of A Lessor GodDocument30 pagesChildren of A Lessor GodMunir KhattakNo ratings yet