
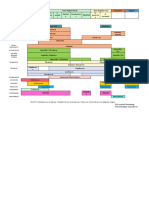
Clinicpath Beta Lactam Cross Reaction Tip Sheet
Clinicpath Beta Lactam Cross Reaction Tip Sheet
You might also like
- Allergy Free Italy With Italian Language Dining Cards For Food AllergiesDocument2 pagesAllergy Free Italy With Italian Language Dining Cards For Food AllergiesKim KoellerNo ratings yet
- Sai Sanjeevini Radionic CardsDocument34 pagesSai Sanjeevini Radionic Cardskwag100% (5)
- PCA Patient Checklist PDFDocument14 pagesPCA Patient Checklist PDFSuper SummonerNo ratings yet
- Antibiotic CoverageDocument1 pageAntibiotic CoverageYNo ratings yet
- ASCIA HP Penicillin Allergy Guide 2016Document1 pageASCIA HP Penicillin Allergy Guide 2016kkkssbbNo ratings yet
- Antibiotics: I - IntroductionDocument8 pagesAntibiotics: I - IntroductionjisooNo ratings yet
- New AntibioticsDocument4 pagesNew AntibioticsMylz MendozaNo ratings yet
- Pcol QSDocument17 pagesPcol QSFaye Kashmier Embestro NamoroNo ratings yet
- Contact Dermatitis ModuleDocument68 pagesContact Dermatitis Moduletimvrghs123No ratings yet
- Allergy Article WorksheetDocument3 pagesAllergy Article Worksheetapi-299996815100% (3)
- Auto Immune DiseasesDocument10 pagesAuto Immune DiseasesliafeliciaNo ratings yet
- Feeding Strategies For Older Infants and ToddlersDocument6 pagesFeeding Strategies For Older Infants and Toddlersxxxxxx100% (2)
- Antibiotic Cross-Sensitivity ChartDocument1 pageAntibiotic Cross-Sensitivity ChartAji YudhaNo ratings yet
- AntibioticsDocument2 pagesAntibioticsPGI Custodio, Ed KristianNo ratings yet
- Pembekalan UKTTK - 2 - 2022Document14 pagesPembekalan UKTTK - 2 - 2022AZIZAHNo ratings yet
- Antibiotic PrescribingDocument1 pageAntibiotic PrescribingJay KayNo ratings yet
- (Pharma A) Antimicrobials 1-Dr. Co (Royce Tan)Document19 pages(Pharma A) Antimicrobials 1-Dr. Co (Royce Tan)Reggie Lyn BaricanNo ratings yet
- Antibotics Venn DiagramDocument2 pagesAntibotics Venn DiagramTop Vids100% (1)
- PDF Antibiotic Prescribing - CompressDocument1 pagePDF Antibiotic Prescribing - CompressMaximilian BezzeghNo ratings yet
- AntibioticsDocument8 pagesAntibioticsmohamed mowafeyNo ratings yet
- Cephalosporins in Veterinary MedicineDocument23 pagesCephalosporins in Veterinary MedicineSunil100% (3)
- ANTIMICROBIAL SmallAnimals - FlipbookDocument14 pagesANTIMICROBIAL SmallAnimals - FlipbookMr. questionNo ratings yet
- Antibiotik Bu DewiDocument2 pagesAntibiotik Bu DewiRohaniNo ratings yet
- Chart Antibacterial Drugs PDFDocument1 pageChart Antibacterial Drugs PDFMunaf AlsumaryNo ratings yet
- CefalosporinasDocument12 pagesCefalosporinasVALENTINA ZAMBRANO ROMERONo ratings yet
- Antibiotic Stewardship Guidebook 2022 v4FINALDocument36 pagesAntibiotic Stewardship Guidebook 2022 v4FINALRabiatul AdawiahNo ratings yet
- Intrinsic Resistance and Unusual Phenotypes Tables v3.2 20200225Document12 pagesIntrinsic Resistance and Unusual Phenotypes Tables v3.2 20200225Roy MontoyaNo ratings yet
- Oct-2023-Durb-Agenda-Item3dDocument28 pagesOct-2023-Durb-Agenda-Item3dI Made AryanaNo ratings yet
- Cephalosporins 2018Document33 pagesCephalosporins 2018Harsha MaheshwariNo ratings yet
- Nursing Home Antimicrobial Stewardship Guide: Help Clinicians Choose The Right AntibioticDocument5 pagesNursing Home Antimicrobial Stewardship Guide: Help Clinicians Choose The Right AntibioticJe Ann Catherine FeliasNo ratings yet
- 191119-GCA3076-MS ANITA GAIKWAD-. Antimicrobial Susceptibility Test NEGDocument1 page191119-GCA3076-MS ANITA GAIKWAD-. Antimicrobial Susceptibility Test NEGMohan RadiyaNo ratings yet
- Overview of by Mechanism 2Document16 pagesOverview of by Mechanism 2daven100% (1)
- Antibiotic Spectrum HKDocument1 pageAntibiotic Spectrum HKhk.medicinesoptNo ratings yet
- Penicillin PDFDocument1 pagePenicillin PDFKumar Bhai0% (1)
- Antibio MergedDocument4 pagesAntibio MergedgaelNo ratings yet
- List of Cephalosporins + Uses, Types & Side EffectsDocument5 pagesList of Cephalosporins + Uses, Types & Side EffectsMd. Sabit Ahsan SarkerNo ratings yet
- Antibiotic Pharmacokinetics & Pharmacodynamics: Bacteriostatic BactericidalDocument4 pagesAntibiotic Pharmacokinetics & Pharmacodynamics: Bacteriostatic BactericidalMd NoumanNo ratings yet
- DiareDocument1 pageDiarejumraaqabah382No ratings yet
- Antibiotics Handout ReferenceDocument3 pagesAntibiotics Handout Referencebl9nkverseNo ratings yet
- Microbiology Urine Culture 2019 2Document1 pageMicrobiology Urine Culture 2019 2Luis Ferdinand Dacera-Gabronino Gamponia-NonanNo ratings yet
- Cell WallDocument5 pagesCell WallNotfor TaoNo ratings yet
- Cell Wall Synthesis InhibitorsDocument6 pagesCell Wall Synthesis Inhibitorshoa1212No ratings yet
- DD Final 1Document22 pagesDD Final 1RafiaNo ratings yet
- CephalosporinDocument34 pagesCephalosporinliamhenry9449No ratings yet
- Clinicpath Cap InfographicDocument1 pageClinicpath Cap InfographicWaleed saleemNo ratings yet
- 1 Generation: Cefalexin Cefradin Cefadroxil Cefachlor Yes Yes Yes Yes YesDocument67 pages1 Generation: Cefalexin Cefradin Cefadroxil Cefachlor Yes Yes Yes Yes YesadystiNo ratings yet
- Prefinal Drug ClassDocument4 pagesPrefinal Drug ClassFtm Ashe SariolNo ratings yet
- First Aid PharmDocument52 pagesFirst Aid PharmJason ClemonsNo ratings yet
- First Aid Pharm PDFDocument52 pagesFirst Aid Pharm PDFRayan OlivaNo ratings yet
- MicroDocument1 pageMicroPatrick DazaNo ratings yet
- Meningitis Treatment & Management - Approach Considerations, Treatment of Subacute Meningitis, Treatment of Bacterial MeningitisDocument15 pagesMeningitis Treatment & Management - Approach Considerations, Treatment of Subacute Meningitis, Treatment of Bacterial MeningitisdilaNo ratings yet
- Antibiogram Pola KumanDocument1 pageAntibiogram Pola KumannadiaNo ratings yet
- Antibiogram 07Document1 pageAntibiogram 07damondouglas100% (1)
- Antibx Cheat SheetDocument1 pageAntibx Cheat Sheetshaun.varghese7No ratings yet
- Description of AntibacterialDocument102 pagesDescription of AntibacterialChristopher SongoroNo ratings yet
- Antibiogram TableDocument2 pagesAntibiogram TableIris ArtNo ratings yet
- AntibioticsDocument1 pageAntibioticsmadeha goharNo ratings yet
- Harrison 2008Document12 pagesHarrison 2008anggaririnNo ratings yet
- Β-Lactam Antibiotics That Share Identical R1-Group Side ChainsDocument2 pagesΒ-Lactam Antibiotics That Share Identical R1-Group Side ChainsFauziah DiayuNo ratings yet
- MICROBIO 1.2 Antimicrobial DrugsDocument3 pagesMICROBIO 1.2 Antimicrobial DrugsPatricia Elena ManaliliNo ratings yet
- Penisilin: Sensitif Terhadap PenicilinaseDocument2 pagesPenisilin: Sensitif Terhadap PenicilinaseSanti ParambangNo ratings yet
- Antibioticsforyear3medics PDFDocument13 pagesAntibioticsforyear3medics PDFShonaMalhanNo ratings yet
- 3 CephalosporinsDocument11 pages3 Cephalosporinsnusaiba.alobaidyNo ratings yet
- The Essential Guide to Cephalexin: Usage, Precautions, Interactions and Side Effects.From EverandThe Essential Guide to Cephalexin: Usage, Precautions, Interactions and Side Effects.No ratings yet
- Adenovirus Vaccine:: What You Need To KnowDocument2 pagesAdenovirus Vaccine:: What You Need To KnowmpersiNo ratings yet
- EnglishDocument7 pagesEnglishAini YuliaNo ratings yet
- Allergic Contact Dermatitis Caused by PEG 22dodecyl GlycolDocument2 pagesAllergic Contact Dermatitis Caused by PEG 22dodecyl GlycolFreddy RojasNo ratings yet
- Nursing Management of Children With Bronchial AsthmaDocument17 pagesNursing Management of Children With Bronchial AsthmaalmishalnetNo ratings yet
- 12 Unit 12.7 - Reading, Speaking, Vocabulary - Medical Science or Science FictionDocument3 pages12 Unit 12.7 - Reading, Speaking, Vocabulary - Medical Science or Science FictionDemian MacedoNo ratings yet
- Critical Care PowerpointDocument63 pagesCritical Care PowerpointtikoNo ratings yet
- Anaphylaxis: Identification, Management and PreventionDocument5 pagesAnaphylaxis: Identification, Management and PreventionÓscar A. Castejón CruzNo ratings yet
- Alergi Susu SapiDocument2 pagesAlergi Susu SapiMaya FikriNo ratings yet
- Allergist OIT Packet 180913 NutsDocument74 pagesAllergist OIT Packet 180913 Nutsmuaz.rizviNo ratings yet
- Anaphylaxis (Case)Document4 pagesAnaphylaxis (Case)drkmwaiNo ratings yet
- ABThera™ PDFDocument2 pagesABThera™ PDFazab00No ratings yet
- Molecular Allergology WebDocument401 pagesMolecular Allergology WebAna-Maria DuMiNo ratings yet
- By Mayo Clinic Staff: Milk Allergy or Milk Intolerance?Document5 pagesBy Mayo Clinic Staff: Milk Allergy or Milk Intolerance?riadwiNo ratings yet
- Vaccine: What You Need To Know: Haemophilus Influenzae Type B (Hib)Document2 pagesVaccine: What You Need To Know: Haemophilus Influenzae Type B (Hib)mpersiNo ratings yet
- Drug StudyDocument5 pagesDrug StudyJohn Cyprian AbeloNo ratings yet
- Section 3, Lay Person's Guide To MedicinesDocument78 pagesSection 3, Lay Person's Guide To MedicinesS.Srinivasan ('Chinu'); Renu KhannaNo ratings yet
- Vn3110-Cv2-A-Pro-5086 - 00 ApprovedDocument40 pagesVn3110-Cv2-A-Pro-5086 - 00 Approvedakın bektaşNo ratings yet
- Sodium ChlorideDocument1 pageSodium ChlorideRAIYYAN COSAINNo ratings yet
- Belgian Atopic Dermatitis GuidelinesDocument14 pagesBelgian Atopic Dermatitis GuidelinesLevi PNo ratings yet
- ALT2022 0622 - Air Purifier Catalogue 2022 - R5 - PagesDocument20 pagesALT2022 0622 - Air Purifier Catalogue 2022 - R5 - PagesChristine HarNo ratings yet
- MENTOR SESSION 1 MARY Format Oet For NursingDocument7 pagesMENTOR SESSION 1 MARY Format Oet For NursingAnjana VargheseNo ratings yet
- Global Atlas AllergyDocument406 pagesGlobal Atlas AllergyΔημήτριος Ιωαννίδης100% (5)
- Ethnomedicinal Survey Report On Plants of Tribal Regions of Anuppur 270Document3 pagesEthnomedicinal Survey Report On Plants of Tribal Regions of Anuppur 270Medtext PublicationsNo ratings yet


















































































Download as pdf or txt
You might also like
- Allergy Free Italy With Italian Language Dining Cards For Food AllergiesDocument2 pagesAllergy Free Italy With Italian Language Dining Cards For Food AllergiesKim KoellerNo ratings yet
- Sai Sanjeevini Radionic CardsDocument34 pagesSai Sanjeevini Radionic Cardskwag100% (5)
- PCA Patient Checklist PDFDocument14 pagesPCA Patient Checklist PDFSuper SummonerNo ratings yet
- Antibiotic CoverageDocument1 pageAntibiotic CoverageYNo ratings yet
- ASCIA HP Penicillin Allergy Guide 2016Document1 pageASCIA HP Penicillin Allergy Guide 2016kkkssbbNo ratings yet
- Antibiotics: I - IntroductionDocument8 pagesAntibiotics: I - IntroductionjisooNo ratings yet
- New AntibioticsDocument4 pagesNew AntibioticsMylz MendozaNo ratings yet
- Pcol QSDocument17 pagesPcol QSFaye Kashmier Embestro NamoroNo ratings yet
- Contact Dermatitis ModuleDocument68 pagesContact Dermatitis Moduletimvrghs123No ratings yet
- Allergy Article WorksheetDocument3 pagesAllergy Article Worksheetapi-299996815100% (3)
- Auto Immune DiseasesDocument10 pagesAuto Immune DiseasesliafeliciaNo ratings yet
- Feeding Strategies For Older Infants and ToddlersDocument6 pagesFeeding Strategies For Older Infants and Toddlersxxxxxx100% (2)
- Antibiotic Cross-Sensitivity ChartDocument1 pageAntibiotic Cross-Sensitivity ChartAji YudhaNo ratings yet
- AntibioticsDocument2 pagesAntibioticsPGI Custodio, Ed KristianNo ratings yet
- Pembekalan UKTTK - 2 - 2022Document14 pagesPembekalan UKTTK - 2 - 2022AZIZAHNo ratings yet
- Antibiotic PrescribingDocument1 pageAntibiotic PrescribingJay KayNo ratings yet
- (Pharma A) Antimicrobials 1-Dr. Co (Royce Tan)Document19 pages(Pharma A) Antimicrobials 1-Dr. Co (Royce Tan)Reggie Lyn BaricanNo ratings yet
- Antibotics Venn DiagramDocument2 pagesAntibotics Venn DiagramTop Vids100% (1)
- PDF Antibiotic Prescribing - CompressDocument1 pagePDF Antibiotic Prescribing - CompressMaximilian BezzeghNo ratings yet
- AntibioticsDocument8 pagesAntibioticsmohamed mowafeyNo ratings yet
- Cephalosporins in Veterinary MedicineDocument23 pagesCephalosporins in Veterinary MedicineSunil100% (3)
- ANTIMICROBIAL SmallAnimals - FlipbookDocument14 pagesANTIMICROBIAL SmallAnimals - FlipbookMr. questionNo ratings yet
- Antibiotik Bu DewiDocument2 pagesAntibiotik Bu DewiRohaniNo ratings yet
- Chart Antibacterial Drugs PDFDocument1 pageChart Antibacterial Drugs PDFMunaf AlsumaryNo ratings yet
- CefalosporinasDocument12 pagesCefalosporinasVALENTINA ZAMBRANO ROMERONo ratings yet
- Antibiotic Stewardship Guidebook 2022 v4FINALDocument36 pagesAntibiotic Stewardship Guidebook 2022 v4FINALRabiatul AdawiahNo ratings yet
- Intrinsic Resistance and Unusual Phenotypes Tables v3.2 20200225Document12 pagesIntrinsic Resistance and Unusual Phenotypes Tables v3.2 20200225Roy MontoyaNo ratings yet
- Oct-2023-Durb-Agenda-Item3dDocument28 pagesOct-2023-Durb-Agenda-Item3dI Made AryanaNo ratings yet
- Cephalosporins 2018Document33 pagesCephalosporins 2018Harsha MaheshwariNo ratings yet
- Nursing Home Antimicrobial Stewardship Guide: Help Clinicians Choose The Right AntibioticDocument5 pagesNursing Home Antimicrobial Stewardship Guide: Help Clinicians Choose The Right AntibioticJe Ann Catherine FeliasNo ratings yet
- 191119-GCA3076-MS ANITA GAIKWAD-. Antimicrobial Susceptibility Test NEGDocument1 page191119-GCA3076-MS ANITA GAIKWAD-. Antimicrobial Susceptibility Test NEGMohan RadiyaNo ratings yet
- Overview of by Mechanism 2Document16 pagesOverview of by Mechanism 2daven100% (1)
- Antibiotic Spectrum HKDocument1 pageAntibiotic Spectrum HKhk.medicinesoptNo ratings yet
- Penicillin PDFDocument1 pagePenicillin PDFKumar Bhai0% (1)
- Antibio MergedDocument4 pagesAntibio MergedgaelNo ratings yet
- List of Cephalosporins + Uses, Types & Side EffectsDocument5 pagesList of Cephalosporins + Uses, Types & Side EffectsMd. Sabit Ahsan SarkerNo ratings yet
- Antibiotic Pharmacokinetics & Pharmacodynamics: Bacteriostatic BactericidalDocument4 pagesAntibiotic Pharmacokinetics & Pharmacodynamics: Bacteriostatic BactericidalMd NoumanNo ratings yet
- DiareDocument1 pageDiarejumraaqabah382No ratings yet
- Antibiotics Handout ReferenceDocument3 pagesAntibiotics Handout Referencebl9nkverseNo ratings yet
- Microbiology Urine Culture 2019 2Document1 pageMicrobiology Urine Culture 2019 2Luis Ferdinand Dacera-Gabronino Gamponia-NonanNo ratings yet
- Cell WallDocument5 pagesCell WallNotfor TaoNo ratings yet
- Cell Wall Synthesis InhibitorsDocument6 pagesCell Wall Synthesis Inhibitorshoa1212No ratings yet
- DD Final 1Document22 pagesDD Final 1RafiaNo ratings yet
- CephalosporinDocument34 pagesCephalosporinliamhenry9449No ratings yet
- Clinicpath Cap InfographicDocument1 pageClinicpath Cap InfographicWaleed saleemNo ratings yet
- 1 Generation: Cefalexin Cefradin Cefadroxil Cefachlor Yes Yes Yes Yes YesDocument67 pages1 Generation: Cefalexin Cefradin Cefadroxil Cefachlor Yes Yes Yes Yes YesadystiNo ratings yet
- Prefinal Drug ClassDocument4 pagesPrefinal Drug ClassFtm Ashe SariolNo ratings yet
- First Aid PharmDocument52 pagesFirst Aid PharmJason ClemonsNo ratings yet
- First Aid Pharm PDFDocument52 pagesFirst Aid Pharm PDFRayan OlivaNo ratings yet
- MicroDocument1 pageMicroPatrick DazaNo ratings yet
- Meningitis Treatment & Management - Approach Considerations, Treatment of Subacute Meningitis, Treatment of Bacterial MeningitisDocument15 pagesMeningitis Treatment & Management - Approach Considerations, Treatment of Subacute Meningitis, Treatment of Bacterial MeningitisdilaNo ratings yet
- Antibiogram Pola KumanDocument1 pageAntibiogram Pola KumannadiaNo ratings yet
- Antibiogram 07Document1 pageAntibiogram 07damondouglas100% (1)
- Antibx Cheat SheetDocument1 pageAntibx Cheat Sheetshaun.varghese7No ratings yet
- Description of AntibacterialDocument102 pagesDescription of AntibacterialChristopher SongoroNo ratings yet
- Antibiogram TableDocument2 pagesAntibiogram TableIris ArtNo ratings yet
- AntibioticsDocument1 pageAntibioticsmadeha goharNo ratings yet
- Harrison 2008Document12 pagesHarrison 2008anggaririnNo ratings yet
- Β-Lactam Antibiotics That Share Identical R1-Group Side ChainsDocument2 pagesΒ-Lactam Antibiotics That Share Identical R1-Group Side ChainsFauziah DiayuNo ratings yet
- MICROBIO 1.2 Antimicrobial DrugsDocument3 pagesMICROBIO 1.2 Antimicrobial DrugsPatricia Elena ManaliliNo ratings yet
- Penisilin: Sensitif Terhadap PenicilinaseDocument2 pagesPenisilin: Sensitif Terhadap PenicilinaseSanti ParambangNo ratings yet
- Antibioticsforyear3medics PDFDocument13 pagesAntibioticsforyear3medics PDFShonaMalhanNo ratings yet
- 3 CephalosporinsDocument11 pages3 Cephalosporinsnusaiba.alobaidyNo ratings yet
- The Essential Guide to Cephalexin: Usage, Precautions, Interactions and Side Effects.From EverandThe Essential Guide to Cephalexin: Usage, Precautions, Interactions and Side Effects.No ratings yet
- Adenovirus Vaccine:: What You Need To KnowDocument2 pagesAdenovirus Vaccine:: What You Need To KnowmpersiNo ratings yet
- EnglishDocument7 pagesEnglishAini YuliaNo ratings yet
- Allergic Contact Dermatitis Caused by PEG 22dodecyl GlycolDocument2 pagesAllergic Contact Dermatitis Caused by PEG 22dodecyl GlycolFreddy RojasNo ratings yet
- Nursing Management of Children With Bronchial AsthmaDocument17 pagesNursing Management of Children With Bronchial AsthmaalmishalnetNo ratings yet
- 12 Unit 12.7 - Reading, Speaking, Vocabulary - Medical Science or Science FictionDocument3 pages12 Unit 12.7 - Reading, Speaking, Vocabulary - Medical Science or Science FictionDemian MacedoNo ratings yet
- Critical Care PowerpointDocument63 pagesCritical Care PowerpointtikoNo ratings yet
- Anaphylaxis: Identification, Management and PreventionDocument5 pagesAnaphylaxis: Identification, Management and PreventionÓscar A. Castejón CruzNo ratings yet
- Alergi Susu SapiDocument2 pagesAlergi Susu SapiMaya FikriNo ratings yet
- Allergist OIT Packet 180913 NutsDocument74 pagesAllergist OIT Packet 180913 Nutsmuaz.rizviNo ratings yet
- Anaphylaxis (Case)Document4 pagesAnaphylaxis (Case)drkmwaiNo ratings yet
- ABThera™ PDFDocument2 pagesABThera™ PDFazab00No ratings yet
- Molecular Allergology WebDocument401 pagesMolecular Allergology WebAna-Maria DuMiNo ratings yet
- By Mayo Clinic Staff: Milk Allergy or Milk Intolerance?Document5 pagesBy Mayo Clinic Staff: Milk Allergy or Milk Intolerance?riadwiNo ratings yet
- Vaccine: What You Need To Know: Haemophilus Influenzae Type B (Hib)Document2 pagesVaccine: What You Need To Know: Haemophilus Influenzae Type B (Hib)mpersiNo ratings yet
- Drug StudyDocument5 pagesDrug StudyJohn Cyprian AbeloNo ratings yet
- Section 3, Lay Person's Guide To MedicinesDocument78 pagesSection 3, Lay Person's Guide To MedicinesS.Srinivasan ('Chinu'); Renu KhannaNo ratings yet
- Vn3110-Cv2-A-Pro-5086 - 00 ApprovedDocument40 pagesVn3110-Cv2-A-Pro-5086 - 00 Approvedakın bektaşNo ratings yet
- Sodium ChlorideDocument1 pageSodium ChlorideRAIYYAN COSAINNo ratings yet
- Belgian Atopic Dermatitis GuidelinesDocument14 pagesBelgian Atopic Dermatitis GuidelinesLevi PNo ratings yet
- ALT2022 0622 - Air Purifier Catalogue 2022 - R5 - PagesDocument20 pagesALT2022 0622 - Air Purifier Catalogue 2022 - R5 - PagesChristine HarNo ratings yet
- MENTOR SESSION 1 MARY Format Oet For NursingDocument7 pagesMENTOR SESSION 1 MARY Format Oet For NursingAnjana VargheseNo ratings yet
- Global Atlas AllergyDocument406 pagesGlobal Atlas AllergyΔημήτριος Ιωαννίδης100% (5)
- Ethnomedicinal Survey Report On Plants of Tribal Regions of Anuppur 270Document3 pagesEthnomedicinal Survey Report On Plants of Tribal Regions of Anuppur 270Medtext PublicationsNo ratings yet