Download as pdf or txt
You might also like
- EKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationFrom EverandEKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationRating: 3 out of 5 stars3/5 (1)
- Chapter 5 - Vision and Mission AnalysisDocument40 pagesChapter 5 - Vision and Mission AnalysisNero Sha100% (5)
- Allstate/McKinsey Bates H000001010Document495 pagesAllstate/McKinsey Bates H0000010104207west59th100% (3)
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsFrom EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNo ratings yet
- EKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasFrom EverandEKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasRating: 3 out of 5 stars3/5 (5)
- ECG Made EasyDocument15 pagesECG Made Easyjrubin83No ratings yet
- Measurement of Line Impedances and Mutual Coupling of Parallel LinesDocument8 pagesMeasurement of Line Impedances and Mutual Coupling of Parallel LinesKhandai SeenananNo ratings yet
- 1MRB520176 Ben RIO580Document20 pages1MRB520176 Ben RIO580alimaghamiNo ratings yet
- An Assignment On Business Ethics..Document11 pagesAn Assignment On Business Ethics..Rahul Dhurka100% (1)
- Acute Inferior Wall Myocardial Infarction: What Is The Culprit Artery?Document3 pagesAcute Inferior Wall Myocardial Infarction: What Is The Culprit Artery?Tom BiusoNo ratings yet
- ECGsDocument4 pagesECGsTom BiusoNo ratings yet
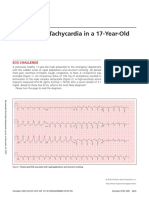
- A Wide QRS Tachycardia in A 17-Year-OldDocument4 pagesA Wide QRS Tachycardia in A 17-Year-OldTaynan MassaroNo ratings yet
- Wide QRS Complex Tachycardia What The Algorithms FearDocument4 pagesWide QRS Complex Tachycardia What The Algorithms FearVerónica UriósteguiNo ratings yet
- J.jaccas.2021.11.016 Rare Congenital Muscle PDFDocument5 pagesJ.jaccas.2021.11.016 Rare Congenital Muscle PDFMariana MorochoNo ratings yet
- Casos de Taquicardia de A NchoDocument4 pagesCasos de Taquicardia de A NchoJosé G. Rodríguez CordovaNo ratings yet
- Current Management Strategies in ACS-Intervention or Conservative - Note, Dr. Faris B, SP - JP (K) FAP PDFDocument51 pagesCurrent Management Strategies in ACS-Intervention or Conservative - Note, Dr. Faris B, SP - JP (K) FAP PDFSofia KusumadewiNo ratings yet
- 2018.the Right-Sided ECG For The Right DiagnosisDocument3 pages2018.the Right-Sided ECG For The Right DiagnosisWeila dos Santos VieiraNo ratings yet
- Myocardial Concept MappingDocument34 pagesMyocardial Concept MappingTHIRD YEARNo ratings yet
- Lee Et Al 2023 Concurrent Acute Ischemic Stroke and Myocardial Infarction Associated With Atrial FibrillationDocument5 pagesLee Et Al 2023 Concurrent Acute Ischemic Stroke and Myocardial Infarction Associated With Atrial FibrillationBlackswannnNo ratings yet
- Crochetage' Sign On ECG in Secundum ASDDocument2 pagesCrochetage' Sign On ECG in Secundum ASDAishah Shalimar PutriNo ratings yet
- 191 201 PDFDocument11 pages191 201 PDFDanyal ShabbirNo ratings yet
- Understanding EKG's: Avant Healthcare ProfessionalsDocument20 pagesUnderstanding EKG's: Avant Healthcare ProfessionalsmarshaNo ratings yet
- Final Oral EditedDocument1 pageFinal Oral EditedRey CortezNo ratings yet
- Anatomically Corrected Malposition of Great Arteries - (I, L, D) Type: First ContactDocument2 pagesAnatomically Corrected Malposition of Great Arteries - (I, L, D) Type: First ContactanhiramdhaniNo ratings yet
- Chyu Shah 2022 Electrocardiograms in Critical Care CardiologyDocument5 pagesChyu Shah 2022 Electrocardiograms in Critical Care Cardiologytegar ksatriaNo ratings yet
- Intramural Hematoma: Journal of Cardiothoracic and Vascular AnesthesiaDocument22 pagesIntramural Hematoma: Journal of Cardiothoracic and Vascular AnesthesiaRomeo GuevaraNo ratings yet
- Multimodality Imaging in Sepsis Related Myocardial CalcificationDocument5 pagesMultimodality Imaging in Sepsis Related Myocardial CalcificationRakhmat RamadhaniNo ratings yet
- Serial T-Wave Changes in A Patient With Chest PainDocument2 pagesSerial T-Wave Changes in A Patient With Chest PainsunhaolanNo ratings yet
- Cardio Diabetes 1Document15 pagesCardio Diabetes 1miguel contrerasNo ratings yet
- Depresion Del ST DX DifDocument7 pagesDepresion Del ST DX DifMiguel Angel Hernandez SerratoNo ratings yet
- Mimicking stemi in cardiac metastasis escDocument3 pagesMimicking stemi in cardiac metastasis esctelavaniumri14No ratings yet
- ECG Feature Extraction For Stress Recognition in Automobile DriversDocument5 pagesECG Feature Extraction For Stress Recognition in Automobile DriversVeronica JanethNo ratings yet
- The Electrophysiological Substrate of Early Repolarization SyndromeDocument12 pagesThe Electrophysiological Substrate of Early Repolarization SyndromeEliomar Garcia BelloNo ratings yet
- Basics ECGpediaDocument6 pagesBasics ECGpediaCarina SuarezNo ratings yet
- Ong 2011Document3 pagesOng 2011arieftamaNo ratings yet
- Typical Chest Pain and An Ominous ECGDocument2 pagesTypical Chest Pain and An Ominous ECGsunhaolanNo ratings yet
- Ebsteins Anomaly-An OverviewDocument36 pagesEbsteins Anomaly-An OverviewRJMNo ratings yet
- Transkutaneus 7 PDFDocument6 pagesTranskutaneus 7 PDFdora mantulNo ratings yet
- 2021 Article 2376Document6 pages2021 Article 2376Anna Sofía ParedesNo ratings yet
- OMedEd - Cardiology - CAD PDFDocument2 pagesOMedEd - Cardiology - CAD PDFJohn DoeNo ratings yet
- Vascular CatastropheDocument3 pagesVascular CatastropheJesily JoyNo ratings yet
- Severe Mitral Stenosis: Images in Clinical MedicineDocument1 pageSevere Mitral Stenosis: Images in Clinical MedicineTaqim IsdaNo ratings yet
- Takotsubo Cardiomyopathy With A Rapidly Resolved LDocument5 pagesTakotsubo Cardiomyopathy With A Rapidly Resolved Lcharmantmayuwano4No ratings yet
- HArtwork EdtDocument3 pagesHArtwork EdtLakshmana PrabuNo ratings yet
- Patofisiologi AneurysmaDocument17 pagesPatofisiologi AneurysmaQori Latifah Ulfah HayatiNo ratings yet
- Eisenmenger Sendromunun E - Lik Etti - I Adams-Oliver Sendromlu Hastalar - in - Loprost Tedavisi (#496559) - 595742Document3 pagesEisenmenger Sendromunun E - Lik Etti - I Adams-Oliver Sendromlu Hastalar - in - Loprost Tedavisi (#496559) - 595742Gabriela GheorgheNo ratings yet
- Pseudonormalization of T Waves After Coronary Angioplasty A Medical Emergency 6656Document3 pagesPseudonormalization of T Waves After Coronary Angioplasty A Medical Emergency 6656Veer VajraNo ratings yet
- ECG Quiz: Sonia Chacko, 5th Year MedicineDocument2 pagesECG Quiz: Sonia Chacko, 5th Year MedicineAņņå SëiŗÿúùNo ratings yet
- TV Dreapta Vs StangaDocument15 pagesTV Dreapta Vs StangaStefana MoisaNo ratings yet
- ECG Course - ECG in Coronary Artery DiseaseDocument33 pagesECG Course - ECG in Coronary Artery DiseasePD-A UB 2017No ratings yet
- (Patho) 1s-3 Cell Adaptation, Injury and DeathDocument10 pages(Patho) 1s-3 Cell Adaptation, Injury and DeathKim RamosNo ratings yet
- An Epsilon Wave On ECG Caso Clinico BMJDocument2 pagesAn Epsilon Wave On ECG Caso Clinico BMJMr. LNo ratings yet
- CIRCULATIONDocument2 pagesCIRCULATIONRVDNo ratings yet
- Acute Coronary SyndromeDocument43 pagesAcute Coronary SyndromeberthyNo ratings yet
- Intercoronary Communication Between The Circumflex and Right Coronary Arteries: A Very Rare Coronary AnomalyDocument2 pagesIntercoronary Communication Between The Circumflex and Right Coronary Arteries: A Very Rare Coronary AnomalyDANNA21No ratings yet
- Blakeway Et Al - 2012 - ECGsDocument2 pagesBlakeway Et Al - 2012 - ECGsRutvik ShahNo ratings yet
- Sample ChapterDocument14 pagesSample ChaptercpfredNo ratings yet
- Acute Coronary SyndromeDocument2 pagesAcute Coronary Syndromemoen bonNo ratings yet
- J Wave SyndromesDocument15 pagesJ Wave SyndromesTony Miguel Saba SabaNo ratings yet
- DR SAN - Update On ACS Management - Workshop PIN PAPDIDocument55 pagesDR SAN - Update On ACS Management - Workshop PIN PAPDIM Daffa Abhista ReviansyahNo ratings yet
- Journal Coartation AortaDocument6 pagesJournal Coartation AortaMangaismeNo ratings yet
- A Sea of Broken Hearts: Patient Rights in a Dangerous, Profit-Driven Health Care SystemFrom EverandA Sea of Broken Hearts: Patient Rights in a Dangerous, Profit-Driven Health Care SystemNo ratings yet
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookFrom EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookNo ratings yet
- 570 Academic Word ListDocument5 pages570 Academic Word ListTrà MyNo ratings yet
- Digital Signal Processing by Ramesh Babu PDFDocument303 pagesDigital Signal Processing by Ramesh Babu PDFJAYA CHANDRA AKULANo ratings yet
- Oracle Demand Management Cloud DsDocument6 pagesOracle Demand Management Cloud DsmrssabaNo ratings yet
- WWW Thestalkingofsarahdegeyter Com 2020-09-26 Wikileaks Founder Julian Assange RDocument6 pagesWWW Thestalkingofsarahdegeyter Com 2020-09-26 Wikileaks Founder Julian Assange RKeith LankfordNo ratings yet
- DHL Strategy ModelDocument59 pagesDHL Strategy Modelfssankar100% (12)
- Irene RAYOS-OMBAC, Complainant, Orlando A. RAYOS, RespondentDocument5 pagesIrene RAYOS-OMBAC, Complainant, Orlando A. RAYOS, RespondentGraceNo ratings yet
- Environmental Liabilities in Colombia: A Critical Review of Current Status and Challenges For A Megadiverse CountryDocument16 pagesEnvironmental Liabilities in Colombia: A Critical Review of Current Status and Challenges For A Megadiverse CountryDgo PalaciosNo ratings yet
- CO2 Supply Agreement - A-ZDocument13 pagesCO2 Supply Agreement - A-ZEslam A. FahmyNo ratings yet
- 5.1079 Compromise Agreement (Arwin) v1.1Document3 pages5.1079 Compromise Agreement (Arwin) v1.1Aldrin LeynesNo ratings yet
- (Laporan Check-In) - Demo MasakDocument1 page(Laporan Check-In) - Demo MasakBudi SuopoNo ratings yet
- Ultra 150 300 Ts FileDocument136 pagesUltra 150 300 Ts FileEmanuel GutierrezNo ratings yet
- Prof. Gandeza - Review Notes in Civil LawDocument58 pagesProf. Gandeza - Review Notes in Civil LawFlorenz Efren CacatianNo ratings yet
- A Hybrid Intrution Detection Approach Based On Deep LearningDocument16 pagesA Hybrid Intrution Detection Approach Based On Deep LearningVictor KingbuilderNo ratings yet
- SM ART-CUT@ Techno Logy S 0 1 A New High Volume Application For Ion ImplantationDocument4 pagesSM ART-CUT@ Techno Logy S 0 1 A New High Volume Application For Ion ImplantationMarco Aurélio DonatoNo ratings yet
- Braille Actuator Report MAJORDocument32 pagesBraille Actuator Report MAJORSwapnil BeheraNo ratings yet
- FEA - Calculation of The Hydroforming Process With LS-DYNADocument8 pagesFEA - Calculation of The Hydroforming Process With LS-DYNAadrianNo ratings yet
- Nas-1000 Ais SartDocument2 pagesNas-1000 Ais SartAntonio VellaraNo ratings yet
- Efficient Securities MarketDocument19 pagesEfficient Securities MarketAnnisa MuktiNo ratings yet
- Amasicon Trade BrochureDocument6 pagesAmasicon Trade BrochureShantanu Saha SaniNo ratings yet
- Lesson 10b: Aggregate Planning Finding An Optimal Production Plan Using Excel SolverDocument7 pagesLesson 10b: Aggregate Planning Finding An Optimal Production Plan Using Excel SolvervaraduNo ratings yet
- 3 If D⋅∇=∈∇.Eand∇.J = σ∇.Ein a given material, the material is said to beDocument3 pages3 If D⋅∇=∈∇.Eand∇.J = σ∇.Ein a given material, the material is said to besai kumar vemparalaNo ratings yet
- EPDDocument34 pagesEPDRobin AbrahamNo ratings yet
- The 60 MM Diameter Solid Shaft Is Subjected To The... PDFDocument3 pagesThe 60 MM Diameter Solid Shaft Is Subjected To The... PDFxy2h5bjs27No ratings yet
- Group 8 Design Main Report + Appendix (1) 1 400Document400 pagesGroup 8 Design Main Report + Appendix (1) 1 400Manishaa Varatha RajuNo ratings yet
- Data Cleansing Process For Master DataDocument4 pagesData Cleansing Process For Master DataAjay Kumar KhattarNo ratings yet