Gastrointestinal Motility
Dr. Joanna Santeliz
Previously it was said, why do we breathe?
–Because we need oxygen to create ATP to
supply energy to all our cells; but in addition
to oxygen we need carbohydrates. So we eat
to obtain carbohydrates and generate ATP.
*Review Macroscopic and Microscopic
Anatomy of the Digestive System.
The basic function of the digestive system is:
taking food, which goes through a process of
digestion and absorption, so that these
processes can be carried out, glands that
secrete hormones and substances participate.
For these ultimate processes of digestion and
absorption to occur, other functions (basically
motor) of the gastrointestinal tract must have
previously occurred. Remember that when
the food enters the mouth, the digestion of
carbohydrates begins, at that level the bolus
must be generated, a series of glands
participate in its formation, including the
salivary glands; Then the esophagus is
responsible for transporting the bolus to the
stomach, where the necessary conditions are
met to begin the digestion of proteins. Then
the bolus passes to the intestine, where the
most important part of digestion/absorption
occurs with the participation of organs such
as the liver, gallbladder, pancreas, etc. Until
the metabolic wastes are eliminated.
Time spent by the bolus in the different
structures:
• Transport from mouth to stomach 10 seconds.
• Lasts 3 hours at stomach level.
• It remains in the small intestine for 7-9 hours.
Frankyelit Guédez, Denis Juárez Page 1
• It remains in the large intestine for 25-30 hours.
• In the rectum – formation of feces – lasts 30-120 hours.
Hormonal secretion: important for the OTHER FUNCTIONS OF THE DIGESTIVE SYSTEM
digestion and absorption processes to occur.
- Excretion of waste material (heavy metals such as copper and iron,
Currently, the importance of the organic anions and cations, drugs, etc.}
gastrointestinal tract in modeling immune *- Regulation of water and electrolyte balance 2- Hormonal secretion
function is being studied and to this end, the ❖ Immune function
role of the intestinal microbiota is being ❖ Role of the intestinal microbiota
studied a lot, that is, how we interact with
the intestinal microbiota.
and how that interaction shapes the immune system.
Remember in general, this is the basic structure of
the digestive system. There is a mucosa that is made
up of: Epithelium, Lamina propria, muscularis of the
mucosa, submucosa, muscularis externa –where
there are 2 layers of smooth muscle oriented in
different ways, the circular layer and the
longitudinal layer- and the serosa.
At the level of the mucosa, the digestive accessory
glands will open, which will allow the processes of
digestion and absorption to take place; and the
secretion of substances that in some way regulate
gastrointestinal motility will also occur at this level.
*This is the basic structure, but each organ/part of
the digestive system has its particularities from a
microscopic point of view.
At the level of the gastrointestinal system there is a
part of the Autonomous Nervous System, which is
the Enteric Nervous System – also called the Second
Brain of the Human Body.
The Enteric Nervous System (ENS) is made up of
approximately 100 million neurons, whose function
is influenced by other neurons of the autonomic
nervous system, such as the neurons of the
sympathetic and parasympathetic nervous system,
and is also seen
Frankyelit Guédez, Denis Juárez Page 2
its action influenced by sensory neurons.
The neurons of the ENS are organized into 2 plexuses: the Submucous Plexus , which is
included along the small and large intestine, and the Myenteric Plexus , which runs from the
esophagus to the anus. The neurons that are part of the ENS are grouped in these 2 plexuses,
and receive influences from each other through interneurons and receive influences from
other higher structures such as the sympathetic and parasympathetic systems.
The Submucosal Plexus has connections with
chemoreceptors (which are constantly
evaluating the intraluminal pH, the osmolarity
of the intraluminal fluid, etc.),
mechanoreceptors (which are constantly
evaluating the distention of the digestive
tract), endocrine cells (which are part of the
mucosa of the gastrointestinal tract). ) and
with secretory cells . -
It not only makes contact with all these cells,
but also with each other. And there are
connections of the Submucous Plexus with the
Myenteric Plexus.
These connections are made through
interneurons. At the same time, these plexuses
receive information from the sympathetic and
parasympathetic systems and sensory
neurons. Therefore, it is a highly complex
system, which is autonomous, that is,
independent of the central nervous system,
but which can be modulated by other parts of
the autonomic nervous system.
Some of the NT secreted by these
neurons:
• The most important is Acetylcholine
, which has fundamentally
excitatory (Depolarizing effects on
membranes).
• Norepinephrine and
Adrenaline have inhibitory effects,
which has hyperpolarizing effects
on membranes.
• And other substances that are
released by both the neurons of the
plexuses and the interneurons.
Frankyelit Guédez, Denis Juárez Page 3
AUTONOMIC CONTROL OF THE Gl TRACT AUTONOMIC CONTROL OF THE Gl TRACT
Parasympathetic innervation: Sympathetic innervation:
1) Cranial : coming from the vagus nerves to the - Originates between segments T5-L2
esophagus, stomach, pancreas to the first part of the large
intestine. - Most of the preganglionic fibers that innervate the TG
enter the sympathetic chains on both sides of the ME and
2) 2nd to 4th sacral segment of the ME : through the pelvic from there pass to external ganglia (e.g. celiac ganglia and
nerves to the distal portion of the large intestine and anus. other mesenteric ganglia ).
These portions receive greater parasympathetic innervation
than the rest of the TG and are important in the defecation - Most of the postganglionic sympathetic neuron bodies
reflex. are located in these ganglia and innervate the entire TG.
re you can see the cranial part of the parasympathetic through
hrough the pelvic nerves that innervate the submucosal and
onic and post-ganglionic fibers of the parasympathetic system.
hat comes out of here are postganglionic fibers that innervate
etic system is pre- and postgangional fibers.
Sensory afferent fibers : they are the
fibers that receive information about what
is happening at the intraluminal level and
take that information to the neurons of
the plexuses, that is, they act as sensors of
what is happening at the level of the
gastrointestinal mucosa; They are capable
of detecting pH, osmolarity and all of the
smooth muscle of the gastrointestinal
tract.
Their stimulus can have excitatory or
inhibitory effects depending on the NT
they are using.
he nervous system, which do not reach the brain and
anch.
reflexes (progressively) they are:
Frankyelit Guédez, Denis Juárez Page 4
-Reflexes that only occur or that their
interaction occurs at the level of the SNE, such
as those involved in digestive secretion,
peristalsis, mixing contraction and inhibitory
effects.
-Reflexes that go from the intestines to the
prevertebral sympathetic ganglia and then can
return, which are the gastrocolic, enterogastric
and colicoileal.
-Reflexes that go to the spinal cord or brain
stem and return to the digestive tract, such as
the defecation reflex and pain reflexes.
Apart from NTs, GI motility is also controlled
by hormones. HORMONAL CONTROL OF Gl MOTILITY
- Cholecystokinin (CCK) : is produced by cells
in the duodenum and jejunum. Which
increases the contraction of the gallbladder.
This is a hormone that somehow modulates
the ENS response and promotes contraction of
the gallbladder.
- Motilin: is produced by cells
endocrine in the upper GI tract, favors the
contraction of intestinal smooth muscle.
Observe which elements are involved in GI
motility and what is their level of importance.
The base is formed by GI and ENS smooth
muscle which is modulated by other parts of
the ANS, and they regulate smooth muscle
contraction.
Between the SNE and the smooth muscle are
the interstitial cells of Cajal. These cells are
not neurons because embryologically they
are derived from the mesoderm, but they
have a very important function.
because they act as pacemaker cells and are where slow waves are generated/occur.
Frankyelit Guédez, Denis Juárez Page 5
The interstitial cells of Cajal can spontaneously
depolarize their cell membrane, it is a depolarization
of small magnitude and short, and that is why they
are said to be pacemaker cells, that is, the cells
where slow waves are generated.
On these slow waves, a greater depolarization can
occur, which can be individual or in the form of a
burst, which does lead to the generation of an action
potential, which will lead to a smooth muscle
contraction response.
Who stimulates this major depolarization in these
cells?
-Acetylcholine, the parasympathetic nervous system
and GI smooth muscle distention.
This depolarization occurs because voltage-
dependent Calcium channels and some voltage-
dependent Potassium channels open.
Norepinephrine and the sympathetic nervous
system produce hyperpolarization of the membrane,
that is, it opposes the effect of acetylcholine.
The interstitial cells of Cajal are located in
different portions in different parts,
where slow waves are produced; These
slow waves will be transmitted to the GI
smooth muscle.
Why can these waves be transmitted
quickly through GI smooth muscle?
-Due to the microscopic characteristic of
GI smooth muscle, it is a syncytium ,
remember the Gap junctions that are
between cells, and which are areas of low
resistance through which the
depolarization wave is transmitted.
*Conclusion: Slow waves are produced in the Cajal
cells (that is why they are called pacemaker cells)
and once those slow waves are produced there, they
are transferred/transmitted through those low
resistance areas, to the rest of the smooth muscle
which is what is going to contract.
There are different types of interstitial cells of Cajal
depending on their location:
* The Cajal cells of the myenteric plexus are what
are really considered the pacemaker cells .
Frankyelit Guédez, Denis Juárez Page 6
*Cajal cells of the subserosa.
Frankyelit Guédez, Denis Juárez Page 7
*Cajal cells of the circular smooth muscle, electrical waves are not sufficiently
between the smooth muscle fibers of the TONIC CONTRACTION OF THE Gl MUSCLE
circular, longitudinal, submucosa portion.
Cajal cells are responsible for the ❖ Tonic contraction is continuous, not associated with
spasmodic contraction of smooth muscle,
but there is a contraction slow waves (it can last from a few minutes to hours)
continuous/permanent what is the ❖ It can be caused by spike-type electrical waves
tonic contraction of smooth muscle.
(repetitive) or by a hormonal effect.
Tonic contraction can be caused by spike- ❖ It can also be caused by continuous entry of calcium
type electrical waves or by hormonal
effects. The interesting thing is that these through still unknown mechanisms.
strong to generate action potentials,
that is, to generate action potentials
that will produce a spasmodic contraction of the smooth muscle. They are the product of a
depolarization, but a depolarization that is not enough to generate an action potential, but it is
not a slow wave either; It is between a slow wave and the depolarization that generates
potentials. These depolarizations are responsible for tonic contraction.
And it is believed that the entry of calcium is involved, through channels that are unknown.
Each of the motor functions of the GI system occur in
different segments of the GI tract.
Each of the types of motility will be seen when each
segment is studied.
CHEWING
*Note: study on your own Mastication, Swallowing.
Chewing is a voluntary motor activity
Continuation -Dr. Vanessa Gómez- controlled by motor cortical areas
When does GI motility begin/at what point?
• It is the result of the rhythmic protraction and retraction of the
• Before digestion begins, the intestine is
prepared, there is production of a secretion, jaw to which lateral and anteroposterior displacements and
which is nothing more than the preparation of coordinated activity of the lips and tongue are associated.
the digestive system.
• Allows the formation of the bolus
Frankyelit Guédez, Denis Juárez Page 8
Chewing: begins the moment there is contact with food, it is a voluntary event. In which the
food is first cut with the incisors and then mixed/crushed with the molars. The goal of this event
is for large food fragments to be transformed into small food fragments that will have a greater
surface area available for enzymatic action.
All GI motility is based on transforming large CHEWING
pieces into small fragments so that the
enzymatic action is easier and there is also • Promotes the efficiency of food digestion by increasing the
greater contact SWALLOWING
with the enteral surface for contact area with digestive enzymes and stimulating the
absorption. secretion of saliva and gastric juice.
❖ It is a complex motor act that requires the coordinated ❖ Starts digestion through the activation of salivary amylase
*Mastication is voluntary , however there is
contractile activity of the muscles of the oral cavity, pharynx, • Prevents large portions of food from entering the digestive tract
literature that speaks of it having an involuntary
esophagus and proximal part of the stomach (No irritation)
component, in which when the jaw is lowered
• It has
the three leads
reflex phases: oral
to a(voluntary),
rise of thepharyngeal
jaw, and esophageal
a contraction
of the jaw.
phase
❖ Coordination of swallowing is a function of the CNS through the the flower pots. So it has a voluntary
swallowing center located in the reticular formation of the component and an involuntary component, but
medulla mainly it is a voluntary activity.
After chewing, another process begins, which is Swallowing, which is nothing more than the
passage of the bolus from the oral cavity to
the proximal portion of the stomach.
This occurs due to a coordinated activity of
the muscles of the oral cavity, pharynx,
esophagus and proximal part of the
stomach, which allows this process.
It has 3 Phases:
(The names of these phases are anatomical
references of where the bolus is at that
moment) -Oral Phase : it is voluntary. In
this phase the tongue pushes the bolus
against the palate and then presses it in
such a way that the bolus passes into the
pharynx.
-Pharyngeal Phase: it is involuntary and from this phase onwards the entire swallowing
process is irreversible. The first thing that must occur is the closure of the glottis, closure of the
choanae - so that the bolus does not pass into the nasal cavity. When the bolus passes into the
oropharynx, the soft palate must collide with the oropharynx to obstruct the choanae, so that the
bolus does not pass.
Frankyelit Guédez, Denis Juárez Page 9
bolus towards the nasopharynx and nasal cavity. In addition to that, another situation that
occurs is that the vocal cords become tense, the neck muscles pull the larynx and make it
ascends and the epiglottis closes. It ends with the beginning of the esophagus.
SWALLOWING
-Oesophageal Phase: the upper esophageal sphincter must relax (because it is always tonically
contracted) and in this way the bolus passes - of course initiating a peristaltic wave - towards
the esophagus. Hard-e-_/
Palate bolus * Soft Tongue—
-i palate Epiglottis
EXPLANATION OF THE VIDEO (SWALLOWING). Trachea Thoracic Inlet' of esoohagus
Bolus h
Esophagus ----------RT
The tongue pushes the bolus towards the soft palate and subsequentlySwallowing towards the oropharynx;
d
the larynx can be seen rising. The first phase, which is the oral phase, is going to be voluntary
FIGURE 9.22 Swallowing. Side views A. The bolus of food I pushed to the back of the oral cavity by pushing the
tongue against the palate B. The nasopharynx is sealed off and the larynx is elevated, enlarging the pharynx to
and is coordinated by the cortex while the pharyngeal and esophageal phases are controlled in
receive food C. The pharyngeal sphincters contract sequentially, squeezing food into the esophagus The epiglottis
closes the trachea 0. The bolus of food moves down the esophagus by peristaltic contractions.
the swallowing center located in the bulb. Subsequently, there are mechanoreceptors in the
oropharynx that generate a reflex arc that is directed towards the swallowing center and will
subsequently generate a response, what will occur is the closure of the choanae over the
nasopharynx and also epiglottic closure and rise of the larynx and They tense the vocal cords.
The bolus is then passed through the upper esophageal sphincter, which relaxes at this time.
What are the afferent pathways of this reflex? Cranial Pairs V, IX and
The integrating center: it is the swallowing center, which is located in the bulb.
The efferent pathways of swallowing: they are V, IX, X and XII Cranial Pair.
Once the bolus is in the esophagus, remember ESOPHAGEAL MOTILITY
that the esophageal phase lasts about 8-10
seconds , that is, you swallow and it is not until
about 8-10 seconds that the contents are barely • From a functional point of view, the esophagus can be divided
reaching the proximal portion of the stomach.
into the upper esophageal sphincter, the body of the esophagus,
When the upper esophageal sphincter closes
again, that is when the lower esophageal and the lower esophageal sphincter.
sphincter (via the vagus nerve) relaxes so that • The types of movements that occur at the level of the esophagus
the bolus passes into the stomach. are peristalsis and tonic contraction.
*Primary peristalsis: refers to a peristaltic wave
• Primary peristalsis and secondary peristalsis may occur
that begins with swallowing.
*Secondary peristalsis: it is actually a response
to a distension of the distal part of the
esophagus or a response to an irritant agent found in that inner part of the esophagus, which
will allow this response to be a peristaltic wave at that level, so that the content that is irritating
that region or distending it can pass into the stomach.
PERISTALSIS
When you have an area that is being distended by the passage of a bolus, there are reflexes that
allow that bolus to be directed towards a certain region. There are reflexes that are located right
there in the ENS, who are in charge of motility? the myenteric and submucosal nervous system,
of which the myenteric is the one
Frankyelit Guédez, Denis Juárez Page 10
mainly responsible for motility (not totally but
mainly). That plexus is the brain of the
intestine, there are reflexes at that level that
cause movement. If this area is distended,
there is a communication through this plexus
that allows the contraction of the proximal
area and immediately adjacent to it and also
allows the advancement of a wave of
contraction in the distal direction. In addition
to this, not only does the proximal area
contract, but as the bolus advances there is a
relaxation that allows the content to descend .
(So there is a proximal contraction and a
distal relaxation as the bolus progresses.)
This type of movement is very generalized
throughout the intestine, esophagus, distal
portion of the stomach, small intestine and
large intestine, all of them have the same type
of movement.
Observe that the propulsive segment
contracts while the receptive segment
relaxes and in this way the same direction of
propulsion - the movement of the bolus - is
maintained.
TONIC CONTRACTION
It occurs mainly in the sphincters, this contraction allows the sphincters to work as a valve,
because under normal conditions they will only allow the passage of the bolus in a
unidirectional manner.
If there is a distension proximal to these sphincters, it means that there is a bolus there that
needs to pass to the next level and this generates relaxation of that sphincter so that the bolus
passes.
But if the segment distal to that sphincter is distended, it means that there is bolus at that level
or there is gas. It is not advisable to open this sphincter, because it would allow a retrograde
passage of those foods.
In the drawing (next page, upper right corner) the pressure differences found in the esophagus
at different moments of propulsion are observed.
*Level 1, which is the upper esophageal sphincter, has a basal pressure. However, it is observed
that in different regions this upper esophageal sphincter is at rest (light green area).
Frankyelit Guédez, Denis Juárez Page 11
a lower pressure compared to this. Furthermore, it is observed how the pressure at different
levels varies with time.
When swallowing, it relaxes, the pressure
drops and then increases again over time.
As it (the bolus) descends, there is an
increase in pressure at different levels,
which corresponds to the contraction of the
proximal level where the bolus is located.
Until relaxation is observed in the lower
esophageal sphincter and then its state of
tonic contraction is maintained.
GASTRIC MOTILITY
In the stomach, contraction and relaxation
occur.
* Anatomical division of the stomach :
fundus, body, antrum and pylorus.
* Functional division of the stomach :
1. Proximal Stomach , composed of the
bottom and part of the body, its function is
storage.
2. Distal Stomach , composed of part of the
body and the antrum, it generates a phasic
contraction that is the Antral Pump that will
allow the propulsion of the bolus towards
the duodenum.
The stomach distends, it has 50ml of
volume and distends, 250ml-500ml-1500ml
distends. The stomach in its proximal
division has a reservoir function, there it stores that volume, what we eat in a fast meal, and it
distends.
Proximal Stomach
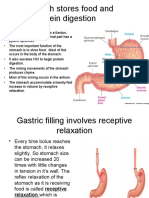
•Receptive relaxation : once
When we swallow, there is a relaxation
of the ---, which means that the stomach
is preparing to receive the bolus (the
“bolus” stimulus is above). This is a Vago-
vagal reflex, meaning that the afferent
pathway is vagal and the efferent
pathway follows
Frankyelit Guédez, Denis Juárez Page 12
being vagal and connecting with motor neurons that are inhibitory within the ENS, which will
release, for example: vasoactive intestinal peptide or even nitric oxide; and this will relax at the
level of the sphincter and also at this level it will distend.
V Adaptive relaxation: the stimulus (bolus) now
It is in the stomach, it is a relaxation in which the Mnemonics: The afferent pathway of
stomach adapts to that bolus that is arriving. It is also a the 3 relaxations is different.
vago-vagal reflex but its location is different.
While the efferent route, that is, the
• Feedback relaxation : the stimulus It is found effect is the same, because the effect
will always be relaxation.
in the duodenum, in response to different nutrients,
in response to a distention of the duodenum; this relaxation will reduce emptiness
Feedback Relaxation
GASTRIC MOTILITY GASTRIC MOTILITY
Receptive Relaxation Adaptive Relaxation
It is a reflex initiated with swallowing
ResU taco stimulation of mechanoreceptors
pharyngeal afferent fibers complex
dorsal vagus nerve vagal efferent fibers
inhibitory
gastric
GASTRIC MOTILITY
Helajaciín
musouar
It is initiated by the presence of food material in the
small intestine
It could be the result of: 1) activation of reflexes
local nervous system leaving intestinal receptors
o 2 release by intestinal endocrine cells of
hormones that would reach the SNE through the blood
gastric GASTRIC MOTILITY
Distal Stomach Contraction
Remember that the distal stomach is made up of
the distal part of the body, the antrum and the pylorus.
In the greater curvature of the stomach we have a
pacemaker region, which will generate peristaltic
contraction waves that will be directed towards the
pylorus. When these contractions occur and the bolus
advances towards the pylorus and the latter is
contracted by means of contraction rings, the bolus
Frankyelit Guédez, Denis Juárez Page 13
Feeding is mixed, that is, there
is segmentation. The contractile
rings advance towards the pylorus
and once the content is at the antral
level and that contraction advances
distally, that content passes to more
proximal regions of the stomach, this
is known as Retropulsion.
So initially a Propulsion
process occurs, in which there is a
movement of the bolus towards the
pylorus and then a Retropulsion, in Figure 51 -19 Propulsive motility of the gastric antral pump as a consequence of food
, a. beginning of the action potential and the contractile cycle in the body, b
view of having great resistance to propagation in the antrum, c, arrival at the pyorus with closure of the pyloric
the passage of food, so the bolus sphincter as a result of primary contraction; another cycle begins at the body
passes to more proximal regions of level. Note that in the terminal antrum and in the ploro, in the plateau phase,
potentials with peaks are inserted that cause short phasic contractions, which
the stomach. add to the secondary contraction and contribute to the sphincter function of the
Generally the diameter that plorus in the prevention of reflux. towards the stomach of the duodenal material.
remains permeable in the pylorus is (Modified from JD Wood, 2003.)
2mm, which indicates that anything
that has a diameter greater than
2mm will not pass through the
pylorus, all of this is postpandrial,
because this is when the pylorus is
tightly closed. However, as time goes
by and we are fasting, everything
larger than 2mm will pass. For
example: a child who swallows a
coin and has an x-ray, in which it is
seen that the coin is somewhere in
the intestine. How could the coin
pass if it measures more than 2mm?
Figure 51-20 Jet retropulsion toward the storage region of gastric luminal
contents, a, beginning of contraction of the terminal antrum; b. Complete explains with what was previously
contraction of the terminal antrum. described. The first 2-3 hours after
ingesting a foreign object, you may
Formation of gastric chyme
think that the object is at the level of
the stomach, so it is very important to know the physiology.
REGULATION OF GASTRIC EMPTYING
Factors that stimulate it:
•Volume of food in the stomach, which generates a myenteric reflex, this is the one
mentioned at the time of peristalsis, which, due to the action of the enteric nervous system,
contracts proximal regions and advances.
Stimulating factors
* Volume of food in the stomach (enteric
reflex)
* Gastrin release (activates pyloric
Frankyelit Guédez, Denis Juárez Page 14
• Release of gastrin, a hormone that is secreted in the G cells of the antrum and
stimulates stomach motility (pyloric pump activation).
Factors that inhibit it:
• Enterogastric neural reflex:
Posterior to the stomach, that is, at the
level of the duodenum there are many
signals that cause gastric emptying to be
delayed. For example: if there is a rapid
passage of substances such as gastric
juice, osmolarly highly charged
substances or the passage of a large
amount of nutrients (CHO, lipids,
proteins), certain signals are activated at
the duodenum level that decrease
stomach and intestinal motility and adequate nutrient absorption does not take place.
therefore its emptying decreases. This occurs because the mucosa may become irritated.
• Great hormonal release: It is a product of the aforementioned. If there is a very low pH in
the duodenum, a hormone called Secretin is released, which increases the aqueous secretion of
the pancreas, allowing the pH to go from acidic to basic. When a lot of fat passes into the
duodenum, cholecystokinin (CCK) is released, and gastric emptying decreases. Gastric Inhibitory
Peptide (GIP) is secreted in the presence of fat, carbohydrates and proteins and is found in the
duodenum in greater than adequate amounts.
Ex: If you drink water and eat something very greasy like pork rinds and then eat meat and
cachapa. Which food is emptied the fastest? First, liquids are emptied faster than solids, since
they pass through the gastric folds. Now, of the solid components, the first thing that is emptied
is the cachapa (CHO), then the meat (protein) is emptied and finally the chicharró n (lipids).
SMALL INTESTINE MOTILITY
There are several types of motility in the intestine:
• Interdigestive Motility: It occurs in
periods where there is no food consumption.
When we are fasting the stomach can make
certain noises, this is known as the Migratory
Motor Complex while the peristaltic movements
after eating food are called the Alimentary Motor
Complex.
The migratory motor complex is found in
the stomach and small intestine, it is not found in
the large intestine. It consists of 4 phases that
generally last between 90-120 min, that is, it is a
cycle.
o Phase I: It is about 40-60 minutes of total
inactivity. There are almost no bowel
movements.
o Phase II: There is a progressive increase
in peristaltic movements.
Frankyelit Guédez, Denis Juárez Page 15
o Phase III: There is a much greater increase in both the frequency and intensity of these
peristaltic movements. A hormone called Motilin acts • The MMC consists of a cycle of 90 to 120 minutes with 4 different
here (EYE: does not act at the level phases:
postprandial). I. 40 - 60 minutes of inactivity
o Phase IV: There is a rapid return to basal II. 30 - 50 minutes of irregular and progressive increase in
activity. peristaltic waves.
• Digestive motility: When food is ingested in III. 5 -10 minutes of regular, high-amplitude contractions that clear the
lumen contents (open pylorus)
IV. Quick return to basal activity.
the small intestine, in addition to the peristaltic propulsion movements that have already been
mentioned, there are Segmentation Movements, consisting of rhythmically contraction and
relaxation movements with the purpose of making a mixing or mixing process occur.
segmentation to increase the contact surface with the enteral mucosa and thus increase the
absorption of nutrients. This type of movement is found in the small intestine and large
intestine.
•
Mass propulsion: It is a single rapid movement that passes the food bolus to another
segment of the intestine. It lasts approximately 18-20 seconds, there is a constant movement of
these muscles that advances at 1cm/sec. This is what is called quick cleaning
Frankyelit Guédez, Denis Juárez Page 16
of the intestine and occurs 1-3 times per day in ❖ They are long-lasting energetic contractions (18-20 sec) of the
normal situations, however, when there is an circular muscles that propagate at a speed of 1 cm/sec.
irritating agent of the mucosa this can occur
❖ Physiological propulsive mechanism to achieve "rapid cleansing" of
more quickly, that is, the frequency increases
and this is where one of the mechanisms occurs. the intestinal lumen {occurs 1-3 times/day)
of diarrhea. ❖ Stimuli : chemical irritation of the intestinal mucosa, luminal
parasites, enterotoxins, allergens, etc.
LARGE INTESTINE MOTILITY
The large intestine receives the bolus in the Cecum, then there is the ascending,
transverse, descending, sigmoid, rectum and ends in the anus.
Functions of the large intestine:
•Absorption of large amounts of liquids and electrolytes. For example: if surgery is
performed at the level of the ileum (it is cut), the substances that come out will be of a very soft
consistency because it does not pass through the colon, which is where liquids are absorbed and
feces are formed.
•Absorption of short chain fatty acids, which were the product of the fermentation of
carbohydrates with bacteria.
• It works as a reservoir for feces.
•Controlled release of feces. There are evacuation habits, for example: there are people
who go to the bathroom every time they eat, there are others who only go once a day or once a
❖ Cecum and ascending week.
colon
1. Receives large volume of material
2. Adaptive relaxation which prevents a large increase in
Cecum and ascending colon
1. Receives large volume of material
intraluminal pressure
2. Adaptive relaxation, which means that
3. Short transit time compared to the other portions of the
the stimulus is in the stomach.
IG (few hours)
3. There is mass movement, so the bolus
4. Motor activity is characterized by orthograde or spends very little time in this part of the large
retrograde peristaltic propulsion intestine
Tra • Transverse and descending colon
nsverse and descending colon 1. The transverse colon is responsible for the absorption of
•
Absorption of water and electrolytes. water and electrolytes and its characteristic movement is
segmentation (haustration).
• There are segmentation movements 2. Propulsion segment: ring contraction
3. Receptive segment: haustras
•
Longer duration compared to previous 4. Longer duration compared to small intestine
segments segmentation
5. Prolonged transit time which allows the initiation of stool
• Long transit time formation
•
Propulsion mass movement, with the
6. The descending colon has a mass movement
(propulsive) in order to move feces over a long distance
purpose of moving feces over a long distance.
towards the anus.
Frankyelit Guédez, Denis Juárez Page 17
• Rectosigmoid region and anal canal rectosigmoid region and anal canal
1. The rectosigmoid region has a distensible storage The rectosigmoid region has a distensible
storage function. Sigmoid functions as a reservoir
function (1/2 It)
and the rectal ampulla certainly distends but when
2. Presence of mechanoreceptors that detect the degree of
there is a more marked distension it generates the
distention of this region defecation reflex.
3. The terminal portion of the anal canal has baroreceptors, Presence of mechanoreceptors, but there are
thermoreceptors, and nocireceptors connected to the
also other types of receptors such as baroreceptors,
thermoreceptors, nocireceptors. The enteric nervous
CNS (awareness of the type of material in the anal canal)
system has a connection with the CNS, so it gives us
What type of material is there. the awareness of knowing the consistency and
DEFECATION REFLEX
It is caused by greater distendibility of the
rectal ampulla and there is a relationship of the anal
sphincter (which is made up of 2 sphincters: an
internal one made up of smooth muscle and whose
relaxation and contraction is involuntary and an
external one that is striated muscle and is
voluntary) . The first thing that occurs is a myenteric
reflex, which means that the reflex is at the level of
GURE 27-9 Motor responses of the anal sphincters to «tension of the the enteric nervous system; As the distension of the
rectal blister progresses, there comes a point at
rectum. Distension produces passive tension to stretching of the wall of
the rectum, and additional active tension when the smooth muscle in the
wall contracts The internal d external sphincters respectively relax and
contract, then comfort, with each stepwise increase in distension until
the essur threshold for defecation is reached. which the pressure of the internal anal sphincter,
which is high, falls, so it relaxes and the pressure of
the external anal sphincter is high because that is
where we have the opportunity to decide to defecate,
and there is greater propulsion of that material
Frankyelit Guédez, Denis Juárez Page 18
distally.
The Reflex not only stays at the level of the enteric nervous system
because here the propulsion is slight, so it advances one more level and reaches
the PNS (Integration Center at the sacral level), then through various fibers it
reaches the cortex to make us aware of that desire. In addition to having greater
motility of the smooth muscles of the colon and relaxation of the sphincters,
other eventualities occur when defecating: action of the facial nerve (gestures
are made with the face), action of the diaphragm, action of the abdominal
muscles so that there is greater intra-abdominal pressure, closing the glottis so
that there is no air escape and maintaining intra-abdominal pressure.
Frankyelit Guédez, Denis Juárez Page 19
ORTHOCOLIC REFLEX
It happens when we get up and this
generates the desire to defecate. Ex: a
patient who has just had surgery is sent to
walk, why? Because movement stimulates
peristalsis.
GASTROCOLIC REFLEX
It occurs when food is ingested. Ex:
There are people who eat and
They immediately go to the bathroom. It
occurs at the level of the thoracic
sympathetic chains and celiac, superior
mesenteric and inferior mesenteric
plexuses.
GASTROILEAL REFLEX
It is similar to gastrocolic, but
instead of there being an increase in
movement at the level of the rectosigmoid
region and descending colon, what there is is an increase in motility in the ileum and the content
passes from the ileum to the cecum and ascending colon.
Frankyelit Guédez, Denis Juárez Page 20
You might also like
- Gut Feelings - The Emerging Biology of Gut-Brain Communication, Emeran A. MayerDocument15 pagesGut Feelings - The Emerging Biology of Gut-Brain Communication, Emeran A. Mayeraltemio100% (1)
- Differences Between The Myenteric and Submucosal Plexuses: Figure 62-4 Neural Control of The Gut WallDocument2 pagesDifferences Between The Myenteric and Submucosal Plexuses: Figure 62-4 Neural Control of The Gut WallMaryama AflahaNo ratings yet
- Neural Control of GITDocument11 pagesNeural Control of GITdoctoroid88% (8)
- Enteric Nervous System1/ Lecture 10:: Extrinsic Nerve SupplyDocument18 pagesEnteric Nervous System1/ Lecture 10:: Extrinsic Nerve SupplyHoney BaseriNo ratings yet
- Enteric Nervous SystemDocument24 pagesEnteric Nervous SystemScribdTranslationsNo ratings yet
- Farmacologie CURS 5 MGDocument44 pagesFarmacologie CURS 5 MGIonescu SarahNo ratings yet
- Autononomic Nervous SystemDocument53 pagesAutononomic Nervous SystemNwandu ChukwukaNo ratings yet
- 10 MotilidadDocument42 pages10 MotilidadKaren GomezNo ratings yet
- General Principles of Gastrointestinal Motility: Alimentary TractDocument6 pagesGeneral Principles of Gastrointestinal Motility: Alimentary TractKC White Dela Rosa100% (1)
- Gut Feelings The Emerging Biology of Gut-Brain ComDocument14 pagesGut Feelings The Emerging Biology of Gut-Brain ComFanny CarrilloNo ratings yet
- Coordination of Nervous System and Endocrine System To Achieve HomeostasisDocument27 pagesCoordination of Nervous System and Endocrine System To Achieve Homeostasiskate corveraNo ratings yet
- 8.1 The Nervous and Endocrine Systems: Neurones (Or Neurons)Document14 pages8.1 The Nervous and Endocrine Systems: Neurones (Or Neurons)KasspapNo ratings yet
- 23.1 Gen Bio ReportingDocument39 pages23.1 Gen Bio ReportingKruk KrukNo ratings yet
- تلخيص 2Document23 pagesتلخيص 2rawanmushtaqtalpNo ratings yet
- 2autonomic Nervous SystemDocument28 pages2autonomic Nervous SystemSolomon H.No ratings yet
- Sistema Nervioso EntéricoDocument6 pagesSistema Nervioso EntéricoCAMILO ANDRES TOVAR DAZANo ratings yet
- Fowler 2008Document14 pagesFowler 2008Pablo IgnacioNo ratings yet
- ANS Ny-NCP 22Document15 pagesANS Ny-NCP 22fatimasulaimanishereNo ratings yet
- Anatomy of The Autonomic Nervous SystemDocument27 pagesAnatomy of The Autonomic Nervous SystemKELVINNo ratings yet
- Physiology of Autonomic Nervous System: J J M Medical College, Davangere. Dept of AnesthesiaDocument117 pagesPhysiology of Autonomic Nervous System: J J M Medical College, Davangere. Dept of AnesthesiaKithminaNo ratings yet
- Untitled 2 4Document8 pagesUntitled 2 4nicksscribd7No ratings yet
- 3rd Lec PharmaDocument30 pages3rd Lec Pharmanightfury200313No ratings yet
- Nervous SystemDocument32 pagesNervous SystemMahadi Hasan KhanNo ratings yet
- Enteric N. System 10011Document5 pagesEnteric N. System 10011Jose Mariano MelendezNo ratings yet
- Exam 3 NotesDocument50 pagesExam 3 NotesAnonymous C6g8uUmWGNo ratings yet
- The Second Brain SeminarDocument85 pagesThe Second Brain SeminarNitish Singla80% (5)
- The Autonomic Nervous System OverviewDocument39 pagesThe Autonomic Nervous System OverviewAhaisibwe GordonNo ratings yet
- Assignment Autonomic Nervous SystemDocument8 pagesAssignment Autonomic Nervous Systemahmad72 raza72No ratings yet
- By: Abduljabbar Hamid Jabbar: University of Baghdad-College of Medicine M. B. Ch. BDocument97 pagesBy: Abduljabbar Hamid Jabbar: University of Baghdad-College of Medicine M. B. Ch. BXena XenaNo ratings yet
- Genbio Finals Lesson 1Document4 pagesGenbio Finals Lesson 1Seb LlaveNo ratings yet
- Unit 4 Perception and Coordination 1Document84 pagesUnit 4 Perception and Coordination 1Iker anubisNo ratings yet
- Psychology PresentationDocument16 pagesPsychology PresentationFasih RehmanNo ratings yet
- Ceballos, Mary Kate L. (BSN 1-Ya-18) - Week 7 - Laboratory Exercise - The Nervous System Cns and PnsDocument9 pagesCeballos, Mary Kate L. (BSN 1-Ya-18) - Week 7 - Laboratory Exercise - The Nervous System Cns and PnsKay ChoiNo ratings yet
- Unit 4 Perception and CoordinationDocument86 pagesUnit 4 Perception and CoordinationMaríaNo ratings yet
- Module 3: The Gastrointestinal System: Learning ObjectivesDocument1 pageModule 3: The Gastrointestinal System: Learning ObjectivesZeina SharkasNo ratings yet
- PHYS - 2S19 - Introduction To Endocrine SystemDocument12 pagesPHYS - 2S19 - Introduction To Endocrine SystemDanes PaguioNo ratings yet
- Exam 3 NotesDocument50 pagesExam 3 NotesAnonymous C6g8uUmWGNo ratings yet
- Biological FoundationDocument13 pagesBiological FoundationsaivdanniiNo ratings yet
- Kuliah PSPD - 2021 - General Principles of Gastrointestinal Function - Motility, Nervous Control, and Blood CirculationDocument31 pagesKuliah PSPD - 2021 - General Principles of Gastrointestinal Function - Motility, Nervous Control, and Blood CirculationadiarthagriadhiNo ratings yet
- Neuroanatomy: Autonomic Nervous System Dr. Antonio T. Parong JRDocument10 pagesNeuroanatomy: Autonomic Nervous System Dr. Antonio T. Parong JRZllison Mae Teodoro MangabatNo ratings yet
- Antiemeticos, Fisiol de VomitosDocument5 pagesAntiemeticos, Fisiol de VomitosFrancisco Ferrer TorresNo ratings yet
- ANS Notes 2000Document2 pagesANS Notes 2000Mkhize KhabazelaNo ratings yet
- GIT Innervation2Document49 pagesGIT Innervation2ammarsaleh186No ratings yet
- Lecture 5.doc AnsDocument8 pagesLecture 5.doc AnsElijah KamaniNo ratings yet
- ANSDocument7 pagesANSKim VilleneuveNo ratings yet
- Ans PharmacologyDocument30 pagesAns PharmacologyBii MarshalNo ratings yet
- Gastrointestinal PhysiologyDocument18 pagesGastrointestinal Physiologyfarwafurqan1No ratings yet
- Lecture 2 Biological Bases of BehaviorDocument35 pagesLecture 2 Biological Bases of BehaviorNURUL FARHANA BINTI IMRAN -No ratings yet
- SGD5 GitDocument59 pagesSGD5 GitMARGARET BLANCHE NICOLASNo ratings yet
- Neurons and Nerves: Building The NetworkDocument6 pagesNeurons and Nerves: Building The NetworkjhustinlaurenteNo ratings yet
- Channels Uro BladderDocument12 pagesChannels Uro BladderKurniadi YusufNo ratings yet
- نسخة Presentation of NeurobiologyDocument29 pagesنسخة Presentation of Neurobiologymonica.a.elnoklawyNo ratings yet
- Chemical and Nervous SystemDocument42 pagesChemical and Nervous SystemMa Divina Kristi DiscarNo ratings yet
- Digestive System ModulesDocument42 pagesDigestive System ModulesOlivia ValenzuelaNo ratings yet
- Chapter II ModuleDocument57 pagesChapter II ModuleAyen LatosaNo ratings yet
- Chapter 7 Bio Class 10Document15 pagesChapter 7 Bio Class 10Aysha KhanNo ratings yet
- Furness Inervação GIDocument33 pagesFurness Inervação GIAndressa SulamitaNo ratings yet
- Physiology of The Digestive System (GIT) : The Gastrointestinal System Carries Out The Following ActivitiesDocument53 pagesPhysiology of The Digestive System (GIT) : The Gastrointestinal System Carries Out The Following ActivitiesBelay MulugetaNo ratings yet
- Ascending SystemDocument104 pagesAscending SystemCharles OkohNo ratings yet
- Natural History of Parkinson's DiseaseDocument49 pagesNatural History of Parkinson's DiseaseScribdTranslationsNo ratings yet
- SYLLABUS Mechanical Drawing 2Document7 pagesSYLLABUS Mechanical Drawing 2ScribdTranslationsNo ratings yet
- Abbreviated File-Process Case 01 Marco A. and CounterclaimDocument25 pagesAbbreviated File-Process Case 01 Marco A. and CounterclaimScribdTranslationsNo ratings yet
- Application of Copper Sulfate in AquacultureDocument2 pagesApplication of Copper Sulfate in AquacultureScribdTranslationsNo ratings yet
- Retirement Instructions Unemployment PorvenirDocument6 pagesRetirement Instructions Unemployment PorvenirScribdTranslationsNo ratings yet
- Ethnicity, Language and IdentityDocument4 pagesEthnicity, Language and IdentityScribdTranslationsNo ratings yet
- Comparative Table of Rationalism and EmpiricismDocument7 pagesComparative Table of Rationalism and EmpiricismScribdTranslationsNo ratings yet
- Chapter X. Precision Shooting From Naval Air PlatformsDocument24 pagesChapter X. Precision Shooting From Naval Air PlatformsScribdTranslationsNo ratings yet
- History and Evolution of Reciprocating MotorsDocument32 pagesHistory and Evolution of Reciprocating MotorsScribdTranslationsNo ratings yet
- Musical Instruments of EuropeDocument3 pagesMusical Instruments of EuropeScribdTranslationsNo ratings yet
- Boxing PDFDocument49 pagesBoxing PDFScribdTranslationsNo ratings yet
- Tourist PlanningDocument39 pagesTourist PlanningScribdTranslationsNo ratings yet
- Legal Aspects GuatemalaDocument20 pagesLegal Aspects GuatemalaScribdTranslationsNo ratings yet
- Practical Work The Familiar PDFDocument1 pagePractical Work The Familiar PDFScribdTranslationsNo ratings yet
- Sixth Grade Reading Comprehension AssessmentDocument8 pagesSixth Grade Reading Comprehension AssessmentScribdTranslationsNo ratings yet
- Project On Electricity For ChildrenDocument13 pagesProject On Electricity For ChildrenScribdTranslationsNo ratings yet
- Reading Comprehension and Contextual Vocabulary Exercises 4th Middle #8.Document5 pagesReading Comprehension and Contextual Vocabulary Exercises 4th Middle #8.ScribdTranslationsNo ratings yet
- 5th Grade Plan - Block 4 GeographyDocument12 pages5th Grade Plan - Block 4 GeographyScribdTranslationsNo ratings yet
- Application of Regulations in The Financial SystemDocument74 pagesApplication of Regulations in The Financial SystemScribdTranslationsNo ratings yet
- PH Portfolio Recovery ProposalDocument3 pagesPH Portfolio Recovery ProposalScribdTranslationsNo ratings yet
- iTEP in - House PDFDocument12 pagesiTEP in - House PDFScribdTranslationsNo ratings yet
- Driver's Manual in TexasDocument109 pagesDriver's Manual in TexasScribdTranslationsNo ratings yet
- Chemistry Laboratory Report 1Document14 pagesChemistry Laboratory Report 1ScribdTranslationsNo ratings yet
- Types of Banks Based On OwnershipDocument2 pagesTypes of Banks Based On OwnershipScribdTranslationsNo ratings yet
- Expo22 Daily ExperienceDocument6 pagesExpo22 Daily ExperienceScribdTranslationsNo ratings yet
- Security of Accounting Information SystemsDocument2 pagesSecurity of Accounting Information SystemsScribdTranslationsNo ratings yet
- Applied StatisticsDocument209 pagesApplied StatisticsScribdTranslationsNo ratings yet
- Examples of Operant ConditioningDocument1 pageExamples of Operant ConditioningScribdTranslationsNo ratings yet
- Vibrational Sound Therapy ManualDocument12 pagesVibrational Sound Therapy ManualScribdTranslationsNo ratings yet
- Event Security ProtocolDocument7 pagesEvent Security ProtocolScribdTranslationsNo ratings yet
- Ahp Ut4Document83 pagesAhp Ut4jeniferNo ratings yet
- Snell AbdomenDocument43 pagesSnell AbdomenBenNo ratings yet
- Common Surgical Problems in Paediatrics Review PDFDocument15 pagesCommon Surgical Problems in Paediatrics Review PDF1031 Muhammad zaryabNo ratings yet
- Hypertrophic Pyloric StenosisDocument22 pagesHypertrophic Pyloric StenosisRex MagallanesNo ratings yet
- GRDDSDocument16 pagesGRDDSRavirajsinh GohilNo ratings yet
- Animal Nutrition and Digestive SystemDocument9 pagesAnimal Nutrition and Digestive SystemJan Alixia BasilioNo ratings yet
- MCQS GitDocument9 pagesMCQS GitMuhammad AdnanNo ratings yet
- Dr. Fatima Safira Alatas, PH.D, Sp.a (K) - Neonatal Gastrointestinal EmergenciesDocument38 pagesDr. Fatima Safira Alatas, PH.D, Sp.a (K) - Neonatal Gastrointestinal EmergenciesMegiNo ratings yet
- Army Public School, Kirkee: Human Digestive Organ-StomachDocument16 pagesArmy Public School, Kirkee: Human Digestive Organ-StomachV Deepak KumarNo ratings yet
- Gastroparesis InfoDocument9 pagesGastroparesis Infoडा. सत्यदेव त्यागी आर्य100% (1)
- Gastroduodenal Peptic UlcerDocument32 pagesGastroduodenal Peptic UlcerLuca Serena0% (1)
- Gastrointestinal PhysiologyDocument134 pagesGastrointestinal Physiologyapi-19916399100% (1)
- Digestive System Anatomy and PhysiologyDocument44 pagesDigestive System Anatomy and PhysiologyPORTRAIT OF A NURSENo ratings yet
- Physiology, Lecture 8, GIT 2 (Stomach) (Slides)Document24 pagesPhysiology, Lecture 8, GIT 2 (Stomach) (Slides)Ali Al-Qudsi100% (2)
- Regulation of Body Weight Lessons Learned FromDocument20 pagesRegulation of Body Weight Lessons Learned FromPolliana CarolinaNo ratings yet
- Fase CefalicaDocument16 pagesFase CefalicaDenisseNo ratings yet
- Ultrasonography of Pylorospasm: Findings May Simulate Hypertrophic Pyloric StenosisDocument7 pagesUltrasonography of Pylorospasm: Findings May Simulate Hypertrophic Pyloric StenosisGladysIndikaNo ratings yet
- Om Health Campus Affiliated To Purbanchal University Gopikrishnanagar, KathmanduDocument107 pagesOm Health Campus Affiliated To Purbanchal University Gopikrishnanagar, KathmanduAdditi SatyalNo ratings yet
- Pyloric StenosisDocument8 pagesPyloric StenosisRej PanganibanNo ratings yet
- Git Physiology Compiled by Umah, Umah VictorDocument43 pagesGit Physiology Compiled by Umah, Umah VictorNwaoha Chibuzor AnthonyNo ratings yet
- Unit Plan Science - Digestive and Excretory SystemsDocument51 pagesUnit Plan Science - Digestive and Excretory Systemsapi-256746237No ratings yet
- Human Physiology DIGESTION & ABSORPTIONDocument12 pagesHuman Physiology DIGESTION & ABSORPTIONM JeevanNo ratings yet
- AnatomyDocument4 pagesAnatomyFaisal AwanNo ratings yet
- Ultraspund in Pediatric EmergencyDocument22 pagesUltraspund in Pediatric EmergencyAli Akbar RahmaniNo ratings yet
- Hypertrophic Pyloric StenosisDocument23 pagesHypertrophic Pyloric StenosisRahel Imelda PanggabeanNo ratings yet
- Esofagus-Anus - UBAYA'21Document61 pagesEsofagus-Anus - UBAYA'21Gek NissaNo ratings yet
- Anatomy and Physiology of Gastrointestinal TractDocument23 pagesAnatomy and Physiology of Gastrointestinal TractJasmin Jacob100% (4)
- PathologyDocument8 pagesPathologyJemimah Tomarong DespabeladeroNo ratings yet
- Module 5 Anatomy I Splanchnology 1Document17 pagesModule 5 Anatomy I Splanchnology 1neannaNo ratings yet
- Class Teaching On Pyloric StenosisDocument23 pagesClass Teaching On Pyloric StenosisRuchika KaushalNo ratings yet