Download as pdf or txt
You might also like
- Impact of Porn On Youth 9Document4 pagesImpact of Porn On Youth 9terminolohiyaNo ratings yet
- Interprofessional Education For Collaborative, Patient-Centred PracticeDocument7 pagesInterprofessional Education For Collaborative, Patient-Centred PracticeAnonymous u5UPeiWpNo ratings yet
- Interprofessional Education For Collaborative, Patient-Centred PracticeDocument7 pagesInterprofessional Education For Collaborative, Patient-Centred PracticeWahyu WijayantoNo ratings yet
- Content ServerDocument11 pagesContent ServerMona AL-FaifiNo ratings yet
- A Framework For The Design ImplementationDocument6 pagesA Framework For The Design ImplementationPATRICIA POLETTONo ratings yet
- Undergraduate-Level Teaching and LearningDocument14 pagesUndergraduate-Level Teaching and LearningNguyên NguyễnNo ratings yet
- The Core Curriculum and Integration in Medical Education: Nikoo Yamani, Masoumeh RahimiDocument5 pagesThe Core Curriculum and Integration in Medical Education: Nikoo Yamani, Masoumeh RahimiDoctorRonZ7No ratings yet
- Faculty Development CPDDocument6 pagesFaculty Development CPDAida TantriNo ratings yet
- Physiotherapy Students DiSC Behaviour Styles CanDocument16 pagesPhysiotherapy Students DiSC Behaviour Styles CanThanh Ha LeNo ratings yet
- 1 s2.0 S1807593222001119 MainDocument6 pages1 s2.0 S1807593222001119 MainNadiraNo ratings yet
- Interprofessional Educationand CollaborationDocument7 pagesInterprofessional Educationand CollaborationnersrosdianaNo ratings yet
- Chapter 1 3 ResearchDocument26 pagesChapter 1 3 ResearchAb Staholic BoiiNo ratings yet
- Interprofessional Education PDFDocument3 pagesInterprofessional Education PDFRobert MontgomeryNo ratings yet
- Thistlethwaite 2015 Anatomical Sciences EducationDocument6 pagesThistlethwaite 2015 Anatomical Sciences EducationIkhwanYudaKusumaNo ratings yet
- Interprofessional Learning: Perceptions of First Year Health StudentsDocument11 pagesInterprofessional Learning: Perceptions of First Year Health Studentsfarhan fathurohmanNo ratings yet
- Advanced Teaching SkillsDocument8 pagesAdvanced Teaching SkillsHany ElbarougyNo ratings yet
- Landasan TeoriDocument3 pagesLandasan TeoriSri WahyuNo ratings yet
- Jurnal 1Document9 pagesJurnal 1bella sariNo ratings yet
- Twelve Tips For Medical Students To Enhance Clinical Skills Learning During Disrupted PlacementsDocument6 pagesTwelve Tips For Medical Students To Enhance Clinical Skills Learning During Disrupted PlacementsÝ HoàngNo ratings yet
- Transformative Leadership Training in Medical Education A TopologyDocument9 pagesTransformative Leadership Training in Medical Education A Topologyslahri7No ratings yet
- Rw-Omj-D-18-00175 (05C)Document6 pagesRw-Omj-D-18-00175 (05C)nersrosdianaNo ratings yet
- Actividades Profesionales ConfiablesDocument6 pagesActividades Profesionales ConfiablesOscar F RojasNo ratings yet
- Submit Due 9.12Document11 pagesSubmit Due 9.12Are HidayuNo ratings yet
- Learning Styles of Physiotherapists: A Systematic Scoping ReviewDocument9 pagesLearning Styles of Physiotherapists: A Systematic Scoping ReviewAndy Delos ReyesNo ratings yet
- Learning Styles of Physiotherapists: A Systematic Scoping ReviewDocument9 pagesLearning Styles of Physiotherapists: A Systematic Scoping ReviewAndy Delos ReyesNo ratings yet
- Academic Emergency Medicine - 2008 - Rudolph - Debriefing As Formative Assessment Closing Performance Gaps in MedicalDocument7 pagesAcademic Emergency Medicine - 2008 - Rudolph - Debriefing As Formative Assessment Closing Performance Gaps in MedicalHafiz RabbiNo ratings yet
- Transfer of Learning Using Simulation Based Education Among Students of Teaching InstitutionsDocument5 pagesTransfer of Learning Using Simulation Based Education Among Students of Teaching InstitutionsEditor IJTSRDNo ratings yet
- Med/Ed Enews v3 No. 06 (MAY 2015)Document13 pagesMed/Ed Enews v3 No. 06 (MAY 2015)KC Spear Ellinwood, former Director Instructional DevelopmentNo ratings yet
- 2011 Impacto Do Uso Da Estrutura Da CIF em Fisioterapia PediátricaDocument8 pages2011 Impacto Do Uso Da Estrutura Da CIF em Fisioterapia PediátricaCibelle FormigaNo ratings yet
- Competency Based Medical Education To Be Edited REVDocument7 pagesCompetency Based Medical Education To Be Edited REVbbytes356No ratings yet
- Sebok Syer 2018 Considering The Interdependence ofDocument11 pagesSebok Syer 2018 Considering The Interdependence ofYoliset RomeroNo ratings yet
- Tips For Teaching SkillsDocument6 pagesTips For Teaching Skillsmuhammad zubair khanNo ratings yet
- Assessment of Learning NeedsDocument4 pagesAssessment of Learning NeedsRhonaJoyNo ratings yet
- A Reflective Analysis of Medical Education Research OnDocument9 pagesA Reflective Analysis of Medical Education Research Onedja minakNo ratings yet
- Quality in Health Care: Strategic Issues in Health Care Management. Huw TO Davies, Manouche Tavakoli, MoDocument2 pagesQuality in Health Care: Strategic Issues in Health Care Management. Huw TO Davies, Manouche Tavakoli, MoTrinh TruongNo ratings yet
- Hee Kim, Yeon. Effects of A Work-Based Critical Reflection Program For Novice NursesDocument6 pagesHee Kim, Yeon. Effects of A Work-Based Critical Reflection Program For Novice Nursescantoni1No ratings yet
- UA OMSE Med/Ed Enews v3 No. 01 (AUG 2014)Document10 pagesUA OMSE Med/Ed Enews v3 No. 01 (AUG 2014)KC Spear Ellinwood, former Director Instructional DevelopmentNo ratings yet
- New Paradigm For CME - JCEHP Sep 2011Document8 pagesNew Paradigm For CME - JCEHP Sep 2011Daniel GuineeNo ratings yet
- The Blacksmith Approach A Strategy For Teaching AnDocument14 pagesThe Blacksmith Approach A Strategy For Teaching AnSamuel BrunNo ratings yet
- Overcoming BarriersDocument10 pagesOvercoming Barriersanidem-No ratings yet
- Strategic Elements of Residency Training in China: Transactional Leadership, Self-Efficacy, and Employee-Orientation CultureDocument8 pagesStrategic Elements of Residency Training in China: Transactional Leadership, Self-Efficacy, and Employee-Orientation CultureChenpeng FENGNo ratings yet
- Foreign Literature FinalsDocument14 pagesForeign Literature FinalsAnghel CruzNo ratings yet
- Levett-Jones Et Al-2018-Journal of Nursing Scholarship1Document10 pagesLevett-Jones Et Al-2018-Journal of Nursing Scholarship1Nande BandeNo ratings yet
- Dimensions of Learning Organizations Questionnaire (DLOQ) in A Low-Resource Health Care Setting in NepalDocument8 pagesDimensions of Learning Organizations Questionnaire (DLOQ) in A Low-Resource Health Care Setting in Nepalsapit90No ratings yet
- A Comparison of Two Scales For Assessing Health Professional Students' Attitude Toward Interprofessional LearningDocument11 pagesA Comparison of Two Scales For Assessing Health Professional Students' Attitude Toward Interprofessional LearningLitera HusadaNo ratings yet
- The Effectiveness of Case-Based Learning in Health Professional Education. A BEME Systematic Review BEME Guide No. 23Document25 pagesThe Effectiveness of Case-Based Learning in Health Professional Education. A BEME Systematic Review BEME Guide No. 23adms.medicalNo ratings yet
- The Development of A Questionnaire To Assess The Readiness (Nurse)Document6 pagesThe Development of A Questionnaire To Assess The Readiness (Nurse)neizhaNo ratings yet
- 12 Tips For Community Based Medical EducationDocument4 pages12 Tips For Community Based Medical EducationRiry AmbarsaryNo ratings yet
- Curriculum Integration From Ladder To LudoDocument4 pagesCurriculum Integration From Ladder To LudoAjay DherwaniNo ratings yet
- Pharmacy Student Professional Identity Formation: A Scoping ReviewDocument20 pagesPharmacy Student Professional Identity Formation: A Scoping ReviewLitera HusadaNo ratings yet
- Faculty Development As An Instrument of 20151121-9725-Jzhlxk-with-cover-page-V2Document9 pagesFaculty Development As An Instrument of 20151121-9725-Jzhlxk-with-cover-page-V2Vice President for Academic Affairs VPAANo ratings yet
- 9 12-OumDocument9 pages9 12-OumAre HidayuNo ratings yet
- Interprofessional Communication (IPC) ForDocument17 pagesInterprofessional Communication (IPC) FornersrosdianaNo ratings yet
- Simulation in Healthcare Education: A Best Evidence Practical Guide. AMEE Guide No. 82Document21 pagesSimulation in Healthcare Education: A Best Evidence Practical Guide. AMEE Guide No. 82Raneem FathyNo ratings yet
- Balance Clinic AcademDocument16 pagesBalance Clinic AcademQaseh MaizaNo ratings yet
- Exploring Faculty Preparedness and Capability For Interprofessional LearningDocument1 pageExploring Faculty Preparedness and Capability For Interprofessional LearningSadashiv RahaneNo ratings yet
- Medical Education in The United States. The Role of AndragogyDocument5 pagesMedical Education in The United States. The Role of AndragogydarkbyronsNo ratings yet
- Harden, R.,1986 - Ten Questions To Ask When Planning A Course or CurriculumDocument10 pagesHarden, R.,1986 - Ten Questions To Ask When Planning A Course or CurriculumSage GrimNo ratings yet
- Medical Education - 2017 - Cleland - Using Paradox Theory To Understand Responses To Tensions Between Service and TrainingDocument14 pagesMedical Education - 2017 - Cleland - Using Paradox Theory To Understand Responses To Tensions Between Service and TrainingJack WaltonNo ratings yet
- A Guide to Medical Teaching and Learning Training of the Trainers (Tot): In the View of the Learner-Centered Learning ModelFrom EverandA Guide to Medical Teaching and Learning Training of the Trainers (Tot): In the View of the Learner-Centered Learning ModelNo ratings yet
- English 2Document22 pagesEnglish 2Alfa TrumpNo ratings yet
- The Context of State Level Policy Formation.Document67 pagesThe Context of State Level Policy Formation.Alfa TrumpNo ratings yet
- The Rise and Rise of The Administrative StateDocument25 pagesThe Rise and Rise of The Administrative StateAlfa TrumpNo ratings yet
- Developing Academic Strategic Alliances - Reconciling Multiple Institutional Cultures, Policies, and PracticesDocument28 pagesDeveloping Academic Strategic Alliances - Reconciling Multiple Institutional Cultures, Policies, and PracticesAlfa TrumpNo ratings yet
- An Opt-In Option For Class ActionsDocument45 pagesAn Opt-In Option For Class ActionsAlfa TrumpNo ratings yet
- The Making of A New Working Class A Study of Collective 3uew1pt8pbDocument20 pagesThe Making of A New Working Class A Study of Collective 3uew1pt8pbAlfa TrumpNo ratings yet
- Power and Legal Artifice The Federal Class Action 4q2dghwrovDocument37 pagesPower and Legal Artifice The Federal Class Action 4q2dghwrovAlfa TrumpNo ratings yet
- Design Your Own Avatar to join our keynote speeches and parallel sessions via Gather.Town - Joint 6th International Conference on New Media Studies and 2nd International Conference On Smart Cities, Automation & InDocument1 pageDesign Your Own Avatar to join our keynote speeches and parallel sessions via Gather.Town - Joint 6th International Conference on New Media Studies and 2nd International Conference On Smart Cities, Automation & InAlfa TrumpNo ratings yet
- Protogan Towards Few Shot Learning For Action Recognition 4x7h50r6bjDocument9 pagesProtogan Towards Few Shot Learning For Action Recognition 4x7h50r6bjAlfa TrumpNo ratings yet
- Studi Pengembangan Bahasa Anak Di TK Hosana SoeDocument6 pagesStudi Pengembangan Bahasa Anak Di TK Hosana SoeAlfa TrumpNo ratings yet
- Liabilities and EquityDocument23 pagesLiabilities and Equityadmiral spongebobNo ratings yet
- Bio Ethanol DBGDocument30 pagesBio Ethanol DBGGhulam RabbaniNo ratings yet
- Nursing Care PlanDocument8 pagesNursing Care Planalexander abasNo ratings yet
- Yokogawa RAGN ManualDocument46 pagesYokogawa RAGN ManualJohn AdewaleNo ratings yet
- Vibration Measurement and Analysis of Rotational Machines: at Makstil Hotplate MillDocument4 pagesVibration Measurement and Analysis of Rotational Machines: at Makstil Hotplate MillMarija PetkovskaNo ratings yet
- RHU Situanional ReportDocument8 pagesRHU Situanional ReportErnest AtonNo ratings yet
- Weathering and Organic Processes Form Soil.: What Makes Soils Different?Document8 pagesWeathering and Organic Processes Form Soil.: What Makes Soils Different?Precious BalgunaNo ratings yet
- Asphaltene Deposition Fundamentals, Prediction, Prevention, and RemediationDocument383 pagesAsphaltene Deposition Fundamentals, Prediction, Prevention, and RemediationDjihan HebbachiNo ratings yet
- Domestic ViolenceDocument17 pagesDomestic ViolenceKhairul IdzwanNo ratings yet
- Past Life Regression Therapist Training WorkshopDocument3 pagesPast Life Regression Therapist Training WorkshopDrManjiree Gokhale50% (2)
- Evelyn Glennie (Responses) PDFDocument8 pagesEvelyn Glennie (Responses) PDFRohit JhambNo ratings yet
- Migraine DiaryDocument1 pageMigraine DiaryEmily KirbyNo ratings yet
- Domestic Dogs: Temporal Range: at Least 14,200 Years Ago - PresentDocument35 pagesDomestic Dogs: Temporal Range: at Least 14,200 Years Ago - PresentirayoNo ratings yet
- BilcoDocument16 pagesBilcoruloNo ratings yet
- Bacteria ProfileDocument18 pagesBacteria ProfileNOR-FATIMAH BARATNo ratings yet
- Improving Fast-Food Restaurants' Method of Operation: Automated Drive-Through Ordering SystemDocument12 pagesImproving Fast-Food Restaurants' Method of Operation: Automated Drive-Through Ordering SystemAllin John FranciscoNo ratings yet
- JuvenilleDocument5 pagesJuvenilleelviemjmontemayorNo ratings yet
- Zoology Mammals (Rabbit)Document3 pagesZoology Mammals (Rabbit)PerrieNo ratings yet
- Tecan Sunrise Absorbance Reader Analyser - User ManualDocument74 pagesTecan Sunrise Absorbance Reader Analyser - User Manualomer oartbNo ratings yet
- How To MentorDocument54 pagesHow To Mentorgetahun esubalewNo ratings yet
- Evolution of Life On Earth: General Biology 2Document10 pagesEvolution of Life On Earth: General Biology 2Geox NikeeNo ratings yet
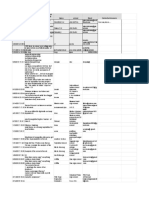
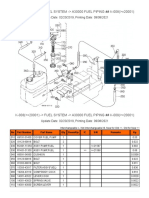
- K-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Document2 pagesK-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Martin LindbergNo ratings yet
- 2022 Children's ReportDocument3 pages2022 Children's ReportMSWD Camiling100% (2)
- SZ Sales ProgramDocument28 pagesSZ Sales ProgramrossifrancescoNo ratings yet
- Laboratory Request Form - TemplateDocument2 pagesLaboratory Request Form - TemplateShafiq Azam RumiNo ratings yet
- OutbreakWksht UpdatedMay18 ADocument3 pagesOutbreakWksht UpdatedMay18 ASatya DwiparthaNo ratings yet
- Anxiety Among High School StudentsDocument21 pagesAnxiety Among High School StudentsFr. Joseph KattakayamNo ratings yet
- Sore ThroatDocument10 pagesSore Throatapi-551073862No ratings yet
- Human TraffickingDocument26 pagesHuman TraffickingNiyoga Singarimbun100% (3)