
Acid-Base-Regulation
Acid-Base-Regulation
You might also like
- IQ Protocol Pass BoxDocument6 pagesIQ Protocol Pass Boxziauddin bukhari100% (1)
- Feasibility StudyDocument5 pagesFeasibility StudyKath Garcia50% (4)
- Clinical Establishment ActDocument44 pagesClinical Establishment ActNeelesh Bhandari100% (1)
- 018 Acid Base BalanceDocument9 pages018 Acid Base BalanceRiggs VDNo ratings yet
- Arterial Blood Gas Interpretation – A case study approachFrom EverandArterial Blood Gas Interpretation – A case study approachRating: 1 out of 5 stars1/5 (1)
- Iso 10003 - 2018 (Eng)Document44 pagesIso 10003 - 2018 (Eng)mblancol75% (4)
- LGIS. PH and BuffersDocument25 pagesLGIS. PH and Buffershasaanmushtaq98765No ratings yet
- Unit 1: Renal System: Acid-Base BalanceDocument48 pagesUnit 1: Renal System: Acid-Base BalancePPP MOHD SUKRINo ratings yet
- 9 - (D) Acid Base Balance Dec 4.17Document61 pages9 - (D) Acid Base Balance Dec 4.17khaledNo ratings yet
- UntitledDocument12 pagesUntitledKeith OmwoyoNo ratings yet
- Respiratory Acid Base Balance 3Document83 pagesRespiratory Acid Base Balance 3Harlyn MagsinoNo ratings yet
- Acid Base BalanceDocument104 pagesAcid Base BalanceKevin VillaranteNo ratings yet
- AcidBase BalanceDocument101 pagesAcidBase BalanceAli Can GunesNo ratings yet
- Acid-Base DisorderDocument68 pagesAcid-Base DisorderPrafulla Paudel100% (3)
- Acid-Base Balance Lecture - Part 1Document43 pagesAcid-Base Balance Lecture - Part 1yigermalamanuel32No ratings yet
- Acid Base Disorders-MD3Document44 pagesAcid Base Disorders-MD3juliuskahabi1No ratings yet
- Clinical Chemistry 2Document37 pagesClinical Chemistry 2Tweetie SiaNo ratings yet
- "If One Advances Confidently in The Direction of His Dreams, He Will Meet With A Success Unexpected in Common HoursDocument44 pages"If One Advances Confidently in The Direction of His Dreams, He Will Meet With A Success Unexpected in Common Hourssantana2007No ratings yet
- Acidebase Physiology - New ConceptsDocument6 pagesAcidebase Physiology - New Conceptsk_c_mclaughlin9847No ratings yet
- Acid Base ImbalanceDocument15 pagesAcid Base ImbalanceIoana SanduNo ratings yet
- Acid-Base Balance IDocument6 pagesAcid-Base Balance Ior1da2sa3No ratings yet
- Acid Base BalanceDocument35 pagesAcid Base BalanceDhanasvi Dessai100% (1)
- Acid Base BalanceDocument43 pagesAcid Base Balanceanju KvNo ratings yet
- Interpretation of Arterial Blood Gases 2009 Surgery OxfordDocument5 pagesInterpretation of Arterial Blood Gases 2009 Surgery OxfordPedro GasparNo ratings yet
- CC Acid and Base Balance and ImbalanceDocument7 pagesCC Acid and Base Balance and ImbalanceGianna SablanNo ratings yet
- Acids BasedDocument5 pagesAcids BasedAngeline TaghapNo ratings yet
- Acid Base Equilibrium, Clinical Concepts and Acid Base DisordersDocument64 pagesAcid Base Equilibrium, Clinical Concepts and Acid Base DisordersevanNo ratings yet
- ABGDocument7 pagesABGEva Marie GaaNo ratings yet
- LECTURE ON Acid-Base BalanceDocument229 pagesLECTURE ON Acid-Base BalanceNayyer Khan100% (1)
- Acid Base Balance PhysiologyDocument49 pagesAcid Base Balance PhysiologyDarshini Nagarajan100% (1)
- Buffer System: Danica Alyssa C. Cruz, RMTDocument27 pagesBuffer System: Danica Alyssa C. Cruz, RMTDanica Alyssa CruzNo ratings yet
- BCH 201 ModuleDocument15 pagesBCH 201 ModuleJoyNo ratings yet
- Acid Base Im Balance-2a - 3.05.2021Document75 pagesAcid Base Im Balance-2a - 3.05.2021Kavya FouzdarNo ratings yet
- Acid Base Balance: Acid: A Molecule That Contributes HDocument16 pagesAcid Base Balance: Acid: A Molecule That Contributes HOsama MohamedNo ratings yet
- Acid-Base Balance - 2023 Batch OctoberDocument54 pagesAcid-Base Balance - 2023 Batch Octoberjohnthar929No ratings yet
- Tortora Asam BasaDocument8 pagesTortora Asam BasaChaori NurfadillahNo ratings yet
- Acid-Base Regulation by The Lungs (Melaku)Document73 pagesAcid-Base Regulation by The Lungs (Melaku)gostrider0093sNo ratings yet
- 9,10,11 - Basics of Acid Base Balance - Buffers - DisordersDocument68 pages9,10,11 - Basics of Acid Base Balance - Buffers - Disordersyigermalamanuel32No ratings yet
- Acid-Base DisordersDocument11 pagesAcid-Base DisordersShia LevyNo ratings yet
- LPN Acid Base Balance UpdateDocument12 pagesLPN Acid Base Balance UpdateLiaqat HussainNo ratings yet
- Acid Base Balance 11Document37 pagesAcid Base Balance 11Mustafa KhandgawiNo ratings yet
- Acid Base DisorderDocument48 pagesAcid Base DisorderAGUNG SETIADI NUGROHONo ratings yet
- Acid Base PhysiologyDocument12 pagesAcid Base PhysiologyaequNo ratings yet
- NCM 3114 Acid Base Imbalance-2Document13 pagesNCM 3114 Acid Base Imbalance-2Fayeh Harah PadrillanNo ratings yet
- Acid-Base Balance and DisodersDocument86 pagesAcid-Base Balance and DisodersPrincewill SeiyefaNo ratings yet
- Acid - Base BalancesDocument68 pagesAcid - Base Balancesjames makulaNo ratings yet
- Acid Base DisordersDocument11 pagesAcid Base DisordersS100% (1)
- Acid Base ImbalancesDocument127 pagesAcid Base ImbalancesKartik RatiNo ratings yet
- Mark Joshua S. Cruz RTRPDocument140 pagesMark Joshua S. Cruz RTRPJeeb Mc TayongNo ratings yet
- (Final) ACID BASE BALANCEDocument68 pages(Final) ACID BASE BALANCEPauline SalvadorNo ratings yet
- Acid Secretion by The KidneyDocument37 pagesAcid Secretion by The KidneyHakimah K. Suhaimi100% (1)
- Lecture 1 Acid Base BiochemistryDocument29 pagesLecture 1 Acid Base BiochemistryThe Great AmegboNo ratings yet
- Prepared by C.J. Latorre 3EMT: PH PK + Log (A) / (HA)Document7 pagesPrepared by C.J. Latorre 3EMT: PH PK + Log (A) / (HA)Nathaniel Derige AndesNo ratings yet
- Arterial Blood GasDocument55 pagesArterial Blood GasLal NandaniNo ratings yet
- Acid-Base Disorders: Dr. Bibhukalyani DasDocument7 pagesAcid-Base Disorders: Dr. Bibhukalyani DasM Fathur Arief KurniawanNo ratings yet
- Regulation of Acid-Base BalanceDocument14 pagesRegulation of Acid-Base BalanceTee bag100% (1)
- Acid Base Balance Flashcards QuizletDocument1 pageAcid Base Balance Flashcards QuizletapolloNo ratings yet
- Tentir Keseimbangan Cairan Dan ElektrolitDocument15 pagesTentir Keseimbangan Cairan Dan ElektrolitErik Ahmad HasyimNo ratings yet
- 1st Chap-2Document40 pages1st Chap-2RJ Noor JanNo ratings yet
- 2 Water PH BuffersDocument45 pages2 Water PH BuffersJoxNo ratings yet
- Acid-Base Balance and DisodersDocument86 pagesAcid-Base Balance and DisodersPrincewill SeiyefaNo ratings yet
- Module 1 Lecture 4Document29 pagesModule 1 Lecture 4Amirs AmjadNo ratings yet
- Acid Base Balance NotesheetDocument12 pagesAcid Base Balance NotesheetMariam MohammedNo ratings yet
- ABG Webinar March 2018Document51 pagesABG Webinar March 2018arbazNo ratings yet
- Game Sense ApproachDocument7 pagesGame Sense Approachapi-408626896No ratings yet
- LeetCode 50 Common Interview Questions With Solutions 1654359171Document100 pagesLeetCode 50 Common Interview Questions With Solutions 1654359171Om SharmaNo ratings yet
- Experience With The Munster-Type Below-Elbow Prosthesis, A Preliminary ReportDocument5 pagesExperience With The Munster-Type Below-Elbow Prosthesis, A Preliminary ReportrehabeasyNo ratings yet
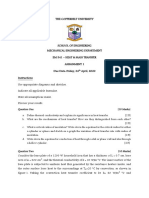
- Assignment 1 - 2020 PDFDocument2 pagesAssignment 1 - 2020 PDFLusambo SimpasaNo ratings yet
- BSBCMM511 Simulation PackDocument4 pagesBSBCMM511 Simulation PackmiraNo ratings yet
- HT Motors Data SheetDocument3 pagesHT Motors Data SheetSE ESTNo ratings yet
- Nile International Freight ServicesDocument19 pagesNile International Freight ServicessameerhamadNo ratings yet
- Tel. ++39 011 9648211 - Fax ++39 011 9648222 E-Mail: Irem@irem - It - WWW - Irem.itDocument8 pagesTel. ++39 011 9648211 - Fax ++39 011 9648222 E-Mail: Irem@irem - It - WWW - Irem.itkenneth molina100% (1)
- Didactic ProductHighlights 2020 v2.6Document20 pagesDidactic ProductHighlights 2020 v2.6agus prasetioNo ratings yet
- Terms and Conditions On The Issuance and Use of RCBC Credit CardsDocument15 pagesTerms and Conditions On The Issuance and Use of RCBC Credit CardsGillian Alexis ColegadoNo ratings yet
- 2023 AWS Partner Funding Benefits Program Guide - EnglishDocument35 pages2023 AWS Partner Funding Benefits Program Guide - EnglishVictor Villacorta ElliottNo ratings yet
- 2023 MS P2 Al Statistics Zimsec Tuks and MR ShareDocument29 pages2023 MS P2 Al Statistics Zimsec Tuks and MR SharerudomposiNo ratings yet
- Comnavsurfpac - Lant Inst 3840.1 Joint Surf ManualDocument72 pagesComnavsurfpac - Lant Inst 3840.1 Joint Surf ManualMontgomery BurksNo ratings yet
- Science 7 q3 Module 3 Week3Document23 pagesScience 7 q3 Module 3 Week3Mary Cila TingalNo ratings yet
- Stat 116Document7 pagesStat 116oguzdagciNo ratings yet
- First AId Notes - UpdatedDocument54 pagesFirst AId Notes - UpdatedewawireNo ratings yet
- Nami Solar Company Profile Aug 2020 ENGDocument13 pagesNami Solar Company Profile Aug 2020 ENGKien Trung Nguyen100% (1)
- Chess PrinciplesDocument11 pagesChess PrinciplesNick PerilNo ratings yet
- Migrating and Installing Avaya Appliance Virtualization PlatformDocument68 pagesMigrating and Installing Avaya Appliance Virtualization PlatformSathish RajanNo ratings yet
- AnycubicSlicer - Usage Instructions - V1.0 - ENDocument16 pagesAnycubicSlicer - Usage Instructions - V1.0 - ENkokiNo ratings yet
- BVM L230Document156 pagesBVM L230JFrink333No ratings yet
- Geotechnical Properties of Dublin Boulder ClayDocument18 pagesGeotechnical Properties of Dublin Boulder ClayBLPgalwayNo ratings yet
- Defiant RPG - GM Guide (Electronic Version) XDocument9 pagesDefiant RPG - GM Guide (Electronic Version) XXosé Lois PérezNo ratings yet
- Perbandingan Jumlah Eritrosit Pada Sampel Darah 3, 2 Dan 1 ML Dengan Antikoagulan K2EdtaDocument6 pagesPerbandingan Jumlah Eritrosit Pada Sampel Darah 3, 2 Dan 1 ML Dengan Antikoagulan K2EdtaNia AzNo ratings yet
- Um Ugm2006 BinggDocument3 pagesUm Ugm2006 BinggZanaNiswahNabilaNo ratings yet
- Bridget Wisnewski ResumeDocument2 pagesBridget Wisnewski Resumeapi-425692010No ratings yet
























































































Download as pdf or txt
You might also like
- IQ Protocol Pass BoxDocument6 pagesIQ Protocol Pass Boxziauddin bukhari100% (1)
- Feasibility StudyDocument5 pagesFeasibility StudyKath Garcia50% (4)
- Clinical Establishment ActDocument44 pagesClinical Establishment ActNeelesh Bhandari100% (1)
- 018 Acid Base BalanceDocument9 pages018 Acid Base BalanceRiggs VDNo ratings yet
- Arterial Blood Gas Interpretation – A case study approachFrom EverandArterial Blood Gas Interpretation – A case study approachRating: 1 out of 5 stars1/5 (1)
- Iso 10003 - 2018 (Eng)Document44 pagesIso 10003 - 2018 (Eng)mblancol75% (4)
- LGIS. PH and BuffersDocument25 pagesLGIS. PH and Buffershasaanmushtaq98765No ratings yet
- Unit 1: Renal System: Acid-Base BalanceDocument48 pagesUnit 1: Renal System: Acid-Base BalancePPP MOHD SUKRINo ratings yet
- 9 - (D) Acid Base Balance Dec 4.17Document61 pages9 - (D) Acid Base Balance Dec 4.17khaledNo ratings yet
- UntitledDocument12 pagesUntitledKeith OmwoyoNo ratings yet
- Respiratory Acid Base Balance 3Document83 pagesRespiratory Acid Base Balance 3Harlyn MagsinoNo ratings yet
- Acid Base BalanceDocument104 pagesAcid Base BalanceKevin VillaranteNo ratings yet
- AcidBase BalanceDocument101 pagesAcidBase BalanceAli Can GunesNo ratings yet
- Acid-Base DisorderDocument68 pagesAcid-Base DisorderPrafulla Paudel100% (3)
- Acid-Base Balance Lecture - Part 1Document43 pagesAcid-Base Balance Lecture - Part 1yigermalamanuel32No ratings yet
- Acid Base Disorders-MD3Document44 pagesAcid Base Disorders-MD3juliuskahabi1No ratings yet
- Clinical Chemistry 2Document37 pagesClinical Chemistry 2Tweetie SiaNo ratings yet
- "If One Advances Confidently in The Direction of His Dreams, He Will Meet With A Success Unexpected in Common HoursDocument44 pages"If One Advances Confidently in The Direction of His Dreams, He Will Meet With A Success Unexpected in Common Hourssantana2007No ratings yet
- Acidebase Physiology - New ConceptsDocument6 pagesAcidebase Physiology - New Conceptsk_c_mclaughlin9847No ratings yet
- Acid Base ImbalanceDocument15 pagesAcid Base ImbalanceIoana SanduNo ratings yet
- Acid-Base Balance IDocument6 pagesAcid-Base Balance Ior1da2sa3No ratings yet
- Acid Base BalanceDocument35 pagesAcid Base BalanceDhanasvi Dessai100% (1)
- Acid Base BalanceDocument43 pagesAcid Base Balanceanju KvNo ratings yet
- Interpretation of Arterial Blood Gases 2009 Surgery OxfordDocument5 pagesInterpretation of Arterial Blood Gases 2009 Surgery OxfordPedro GasparNo ratings yet
- CC Acid and Base Balance and ImbalanceDocument7 pagesCC Acid and Base Balance and ImbalanceGianna SablanNo ratings yet
- Acids BasedDocument5 pagesAcids BasedAngeline TaghapNo ratings yet
- Acid Base Equilibrium, Clinical Concepts and Acid Base DisordersDocument64 pagesAcid Base Equilibrium, Clinical Concepts and Acid Base DisordersevanNo ratings yet
- ABGDocument7 pagesABGEva Marie GaaNo ratings yet
- LECTURE ON Acid-Base BalanceDocument229 pagesLECTURE ON Acid-Base BalanceNayyer Khan100% (1)
- Acid Base Balance PhysiologyDocument49 pagesAcid Base Balance PhysiologyDarshini Nagarajan100% (1)
- Buffer System: Danica Alyssa C. Cruz, RMTDocument27 pagesBuffer System: Danica Alyssa C. Cruz, RMTDanica Alyssa CruzNo ratings yet
- BCH 201 ModuleDocument15 pagesBCH 201 ModuleJoyNo ratings yet
- Acid Base Im Balance-2a - 3.05.2021Document75 pagesAcid Base Im Balance-2a - 3.05.2021Kavya FouzdarNo ratings yet
- Acid Base Balance: Acid: A Molecule That Contributes HDocument16 pagesAcid Base Balance: Acid: A Molecule That Contributes HOsama MohamedNo ratings yet
- Acid-Base Balance - 2023 Batch OctoberDocument54 pagesAcid-Base Balance - 2023 Batch Octoberjohnthar929No ratings yet
- Tortora Asam BasaDocument8 pagesTortora Asam BasaChaori NurfadillahNo ratings yet
- Acid-Base Regulation by The Lungs (Melaku)Document73 pagesAcid-Base Regulation by The Lungs (Melaku)gostrider0093sNo ratings yet
- 9,10,11 - Basics of Acid Base Balance - Buffers - DisordersDocument68 pages9,10,11 - Basics of Acid Base Balance - Buffers - Disordersyigermalamanuel32No ratings yet
- Acid-Base DisordersDocument11 pagesAcid-Base DisordersShia LevyNo ratings yet
- LPN Acid Base Balance UpdateDocument12 pagesLPN Acid Base Balance UpdateLiaqat HussainNo ratings yet
- Acid Base Balance 11Document37 pagesAcid Base Balance 11Mustafa KhandgawiNo ratings yet
- Acid Base DisorderDocument48 pagesAcid Base DisorderAGUNG SETIADI NUGROHONo ratings yet
- Acid Base PhysiologyDocument12 pagesAcid Base PhysiologyaequNo ratings yet
- NCM 3114 Acid Base Imbalance-2Document13 pagesNCM 3114 Acid Base Imbalance-2Fayeh Harah PadrillanNo ratings yet
- Acid-Base Balance and DisodersDocument86 pagesAcid-Base Balance and DisodersPrincewill SeiyefaNo ratings yet
- Acid - Base BalancesDocument68 pagesAcid - Base Balancesjames makulaNo ratings yet
- Acid Base DisordersDocument11 pagesAcid Base DisordersS100% (1)
- Acid Base ImbalancesDocument127 pagesAcid Base ImbalancesKartik RatiNo ratings yet
- Mark Joshua S. Cruz RTRPDocument140 pagesMark Joshua S. Cruz RTRPJeeb Mc TayongNo ratings yet
- (Final) ACID BASE BALANCEDocument68 pages(Final) ACID BASE BALANCEPauline SalvadorNo ratings yet
- Acid Secretion by The KidneyDocument37 pagesAcid Secretion by The KidneyHakimah K. Suhaimi100% (1)
- Lecture 1 Acid Base BiochemistryDocument29 pagesLecture 1 Acid Base BiochemistryThe Great AmegboNo ratings yet
- Prepared by C.J. Latorre 3EMT: PH PK + Log (A) / (HA)Document7 pagesPrepared by C.J. Latorre 3EMT: PH PK + Log (A) / (HA)Nathaniel Derige AndesNo ratings yet
- Arterial Blood GasDocument55 pagesArterial Blood GasLal NandaniNo ratings yet
- Acid-Base Disorders: Dr. Bibhukalyani DasDocument7 pagesAcid-Base Disorders: Dr. Bibhukalyani DasM Fathur Arief KurniawanNo ratings yet
- Regulation of Acid-Base BalanceDocument14 pagesRegulation of Acid-Base BalanceTee bag100% (1)
- Acid Base Balance Flashcards QuizletDocument1 pageAcid Base Balance Flashcards QuizletapolloNo ratings yet
- Tentir Keseimbangan Cairan Dan ElektrolitDocument15 pagesTentir Keseimbangan Cairan Dan ElektrolitErik Ahmad HasyimNo ratings yet
- 1st Chap-2Document40 pages1st Chap-2RJ Noor JanNo ratings yet
- 2 Water PH BuffersDocument45 pages2 Water PH BuffersJoxNo ratings yet
- Acid-Base Balance and DisodersDocument86 pagesAcid-Base Balance and DisodersPrincewill SeiyefaNo ratings yet
- Module 1 Lecture 4Document29 pagesModule 1 Lecture 4Amirs AmjadNo ratings yet
- Acid Base Balance NotesheetDocument12 pagesAcid Base Balance NotesheetMariam MohammedNo ratings yet
- ABG Webinar March 2018Document51 pagesABG Webinar March 2018arbazNo ratings yet
- Game Sense ApproachDocument7 pagesGame Sense Approachapi-408626896No ratings yet
- LeetCode 50 Common Interview Questions With Solutions 1654359171Document100 pagesLeetCode 50 Common Interview Questions With Solutions 1654359171Om SharmaNo ratings yet
- Experience With The Munster-Type Below-Elbow Prosthesis, A Preliminary ReportDocument5 pagesExperience With The Munster-Type Below-Elbow Prosthesis, A Preliminary ReportrehabeasyNo ratings yet
- Assignment 1 - 2020 PDFDocument2 pagesAssignment 1 - 2020 PDFLusambo SimpasaNo ratings yet
- BSBCMM511 Simulation PackDocument4 pagesBSBCMM511 Simulation PackmiraNo ratings yet
- HT Motors Data SheetDocument3 pagesHT Motors Data SheetSE ESTNo ratings yet
- Nile International Freight ServicesDocument19 pagesNile International Freight ServicessameerhamadNo ratings yet
- Tel. ++39 011 9648211 - Fax ++39 011 9648222 E-Mail: Irem@irem - It - WWW - Irem.itDocument8 pagesTel. ++39 011 9648211 - Fax ++39 011 9648222 E-Mail: Irem@irem - It - WWW - Irem.itkenneth molina100% (1)
- Didactic ProductHighlights 2020 v2.6Document20 pagesDidactic ProductHighlights 2020 v2.6agus prasetioNo ratings yet
- Terms and Conditions On The Issuance and Use of RCBC Credit CardsDocument15 pagesTerms and Conditions On The Issuance and Use of RCBC Credit CardsGillian Alexis ColegadoNo ratings yet
- 2023 AWS Partner Funding Benefits Program Guide - EnglishDocument35 pages2023 AWS Partner Funding Benefits Program Guide - EnglishVictor Villacorta ElliottNo ratings yet
- 2023 MS P2 Al Statistics Zimsec Tuks and MR ShareDocument29 pages2023 MS P2 Al Statistics Zimsec Tuks and MR SharerudomposiNo ratings yet
- Comnavsurfpac - Lant Inst 3840.1 Joint Surf ManualDocument72 pagesComnavsurfpac - Lant Inst 3840.1 Joint Surf ManualMontgomery BurksNo ratings yet
- Science 7 q3 Module 3 Week3Document23 pagesScience 7 q3 Module 3 Week3Mary Cila TingalNo ratings yet
- Stat 116Document7 pagesStat 116oguzdagciNo ratings yet
- First AId Notes - UpdatedDocument54 pagesFirst AId Notes - UpdatedewawireNo ratings yet
- Nami Solar Company Profile Aug 2020 ENGDocument13 pagesNami Solar Company Profile Aug 2020 ENGKien Trung Nguyen100% (1)
- Chess PrinciplesDocument11 pagesChess PrinciplesNick PerilNo ratings yet
- Migrating and Installing Avaya Appliance Virtualization PlatformDocument68 pagesMigrating and Installing Avaya Appliance Virtualization PlatformSathish RajanNo ratings yet
- AnycubicSlicer - Usage Instructions - V1.0 - ENDocument16 pagesAnycubicSlicer - Usage Instructions - V1.0 - ENkokiNo ratings yet
- BVM L230Document156 pagesBVM L230JFrink333No ratings yet
- Geotechnical Properties of Dublin Boulder ClayDocument18 pagesGeotechnical Properties of Dublin Boulder ClayBLPgalwayNo ratings yet
- Defiant RPG - GM Guide (Electronic Version) XDocument9 pagesDefiant RPG - GM Guide (Electronic Version) XXosé Lois PérezNo ratings yet
- Perbandingan Jumlah Eritrosit Pada Sampel Darah 3, 2 Dan 1 ML Dengan Antikoagulan K2EdtaDocument6 pagesPerbandingan Jumlah Eritrosit Pada Sampel Darah 3, 2 Dan 1 ML Dengan Antikoagulan K2EdtaNia AzNo ratings yet
- Um Ugm2006 BinggDocument3 pagesUm Ugm2006 BinggZanaNiswahNabilaNo ratings yet
- Bridget Wisnewski ResumeDocument2 pagesBridget Wisnewski Resumeapi-425692010No ratings yet