Download as pdf or txt
You might also like
- Mental Status ExaminationDocument4 pagesMental Status Examinationjayrdungca83% (18)
- 003-User - Pass (Combo)Document554 pages003-User - Pass (Combo)Juan José CamachoNo ratings yet
- Occupational Profile AnalysisDocument20 pagesOccupational Profile Analysisapi-292815157No ratings yet
- Esther Bick - Infant ObservationDocument10 pagesEsther Bick - Infant ObservationdanielalucaNo ratings yet
- Risk Assessment For Installation of BMS M Tower PDFDocument15 pagesRisk Assessment For Installation of BMS M Tower PDFAndrew HivNo ratings yet
- 101 FDI-SinDocument49 pages101 FDI-SinLê Hoàng Việt HảiNo ratings yet
- Case Study Dengue FeverDocument25 pagesCase Study Dengue FeverAdrian Mallar100% (1)
- 13 Areas of AssessmentDocument3 pages13 Areas of AssessmentCamilogsNo ratings yet
- Sleep Deprivation and Its Effect To StudentDocument30 pagesSleep Deprivation and Its Effect To StudentJoshua Capote100% (3)
- Lionet Lovey: Pattern by Mila Kralina (Ds - Mouse)Document9 pagesLionet Lovey: Pattern by Mila Kralina (Ds - Mouse)Fátima Hunter100% (3)
- One Page Summary of My CV That Can Save Some Time.Document1 pageOne Page Summary of My CV That Can Save Some Time.NaveenNo ratings yet
- Case Study - Six-Year-Old Boy With Asperger's Syndrome and HyperactivityDocument4 pagesCase Study - Six-Year-Old Boy With Asperger's Syndrome and Hyperactivityxiejie22590No ratings yet
- CaseStudy - 10 Year Old Boy PDFDocument3 pagesCaseStudy - 10 Year Old Boy PDFRachelle SalcedoNo ratings yet
- Informe TecDocument10 pagesInforme TecAmy BaquerizoNo ratings yet
- Case Study Egv Down SyndromeDocument8 pagesCase Study Egv Down SyndromeChristal Felisilda Dela CruzNo ratings yet
- 1946 Pioneer Work With Cerebral Palsy. MHDocument2 pages1946 Pioneer Work With Cerebral Palsy. MHJoseloNo ratings yet
- Case StudyDocument2 pagesCase Studymamasita25No ratings yet
- Peds Journal 2Document5 pagesPeds Journal 2serbo81No ratings yet
- Capitol Medical Center Colleges, Inc. College of Nursing NCM 105 - Lecture FinalsDocument6 pagesCapitol Medical Center Colleges, Inc. College of Nursing NCM 105 - Lecture FinalsFaye Dianne Damian-BuenafeNo ratings yet
- G3 - Final Case Study - Incomplete MiscarriageDocument37 pagesG3 - Final Case Study - Incomplete MiscarriageSiobhan GreeneNo ratings yet
- Sistema AumentativoDocument9 pagesSistema Aumentativolaura valentina castillo sanchezNo ratings yet
- Peds Journal 1Document6 pagesPeds Journal 1serbo81No ratings yet
- (Olfu) Pediatrics Case Study: Post Streptococcal Glomerulo Nephritis (PSGN)Document20 pages(Olfu) Pediatrics Case Study: Post Streptococcal Glomerulo Nephritis (PSGN)MikaCasimiroBalunanNo ratings yet
- G3 - Incomplete MiscarriageDocument35 pagesG3 - Incomplete MiscarriageSiobhan GreeneNo ratings yet
- Fieldwork I Aba Therapy PresentationDocument12 pagesFieldwork I Aba Therapy Presentationapi-739096198No ratings yet
- Midterm Evaluation - ClinicalDocument7 pagesMidterm Evaluation - Clinicalapi-240864098No ratings yet
- SCHIZODocument25 pagesSCHIZOQuinonez Anna MarieNo ratings yet
- Professional Progress SummaryDocument16 pagesProfessional Progress Summaryapi-272878167No ratings yet
- Garland Teresa Hands-On Activities For Children With Autism Sensory DisordersDocument396 pagesGarland Teresa Hands-On Activities For Children With Autism Sensory DisordersGriselda Leon100% (2)
- Autism Spectrum Disorder-MANUSCRIPT2CDocument20 pagesAutism Spectrum Disorder-MANUSCRIPT2CPaul AnteNo ratings yet
- Birth Trauma Case Study. A. Learner BackgroundDocument4 pagesBirth Trauma Case Study. A. Learner BackgroundlydianajaswinNo ratings yet
- Sensory Alterations TestbankDocument26 pagesSensory Alterations Testbankalaisahmae02No ratings yet
- Case Pres )Document18 pagesCase Pres )Justin Faye VibarNo ratings yet
- Date/ Time Focus DAR: Disturbed Thought ProcessDocument1 pageDate/ Time Focus DAR: Disturbed Thought ProcessMaria Chrislyn Marcos GenorgaNo ratings yet
- KYLE OLOR RLE REQS - Docx 1Document14 pagesKYLE OLOR RLE REQS - Docx 1Bernadeth Barrientos ZamoraNo ratings yet
- Developmental AssessmentDocument2 pagesDevelopmental Assessmentapi-300851869No ratings yet
- Case AnalyisisDocument10 pagesCase AnalyisisRubelleMicahCagampangSapongNo ratings yet
- 22childhood Masturbation Simulating Epileptic Seizures A Report of Two Cases and Review of The LiteratureDocument3 pages22childhood Masturbation Simulating Epileptic Seizures A Report of Two Cases and Review of The Literaturesam_mad00100% (1)
- 1I02 Clinical Nursing Practice Notes Week 3 Reflection (3 Parts)Document39 pages1I02 Clinical Nursing Practice Notes Week 3 Reflection (3 Parts)NTRisforthinkersNo ratings yet
- Prodigalidad, Z C. - Week 1 - Day 2 - MCN DutyDocument2 pagesProdigalidad, Z C. - Week 1 - Day 2 - MCN DutyZxiayieee JeonNo ratings yet
- Midterm - DaijaunaDocument6 pagesMidterm - Daijaunaapi-312474169No ratings yet
- Performance Portfolio Of: Anna Anjelica R. SanchezDocument8 pagesPerformance Portfolio Of: Anna Anjelica R. SanchezMargaux SarmientoNo ratings yet
- Dwnload Full Cognitive Psychology Connecting Mind Research and Everyday Experience 4th Edition Goldstein Test Bank PDFDocument36 pagesDwnload Full Cognitive Psychology Connecting Mind Research and Everyday Experience 4th Edition Goldstein Test Bank PDFsummitmoleskinzr9x8100% (17)
- BASEMA 13 Areas of AssessmentDocument3 pagesBASEMA 13 Areas of AssessmentBasema HashhashNo ratings yet
- Acute PyelonephritisDocument27 pagesAcute PyelonephritisLucia CaseNo ratings yet
- Adhd Case StudyDocument7 pagesAdhd Case Studyharmno1No ratings yet
- Objectives PsychDocument6 pagesObjectives PsychHerbie SoNo ratings yet
- Sitio Gonzales, Barangay Kamputhaw, Cebu City, Cebu: Submitted byDocument48 pagesSitio Gonzales, Barangay Kamputhaw, Cebu City, Cebu: Submitted byLester DalanonNo ratings yet
- Midwifery Case StudyDocument51 pagesMidwifery Case StudyJosphat KoinangeNo ratings yet
- Hearing Impairement Case StudyDocument19 pagesHearing Impairement Case StudyKJovejera Ovejera100% (1)
- Case StudDocument13 pagesCase StudCzar Alexis FernandezNo ratings yet
- Our Lady of Fatima University - Valenzuela Campus College of NursingDocument16 pagesOur Lady of Fatima University - Valenzuela Campus College of NursingKHRISTINE MAE ROQUENo ratings yet
- Our Lady of Fatima University - Valenzuela Campus College of NursingDocument17 pagesOur Lady of Fatima University - Valenzuela Campus College of NursingKHRISTINE MAE ROQUENo ratings yet
- ObjectivesDocument10 pagesObjectivesCzar Alexis FernandezNo ratings yet
- Occupational Profile and Analysis Final EditedDocument14 pagesOccupational Profile and Analysis Final Editedapi-233645719No ratings yet
- Intellectual DisabilityDocument15 pagesIntellectual Disabilitykhanyumna472No ratings yet
- NH11functionalpatterns PADocument4 pagesNH11functionalpatterns PAYusephAwangSanaaniNo ratings yet
- Masquerade of Loneliness : Filamer Chistian University College of Nursing Roxas CityDocument16 pagesMasquerade of Loneliness : Filamer Chistian University College of Nursing Roxas CityJason A. AdoyoganNo ratings yet
- A Case Study On Acute Tonsillopharyngitis: Bulacan State University City of Malolos, Bulacan College of NursingDocument61 pagesA Case Study On Acute Tonsillopharyngitis: Bulacan State University City of Malolos, Bulacan College of NursingHomework PingNo ratings yet
- Internship Case HistoryDocument7 pagesInternship Case HistoryYamini JohriNo ratings yet
- I. Patient'S Profile: V. Mse (Mental Status Examination)Document2 pagesI. Patient'S Profile: V. Mse (Mental Status Examination)Loungayvan BatuyogNo ratings yet
- Armada Unit IvDocument17 pagesArmada Unit IvInna ThalleiahNo ratings yet
- Angeles Case PresentationDocument54 pagesAngeles Case Presentationangeles khartuNo ratings yet
- IT Week1Document11 pagesIT Week1Mustafa AdilNo ratings yet
- Course Syllabus - People and The Earth's Ecosystem - GED 172Document8 pagesCourse Syllabus - People and The Earth's Ecosystem - GED 172Michaella Dometita100% (1)
- Final New ProfileDocument26 pagesFinal New ProfileParveshNo ratings yet
- Green Building Designing Innovation in India A Literature Review PDFDocument8 pagesGreen Building Designing Innovation in India A Literature Review PDFBulbul SahuNo ratings yet
- Lesson PlanDocument5 pagesLesson Planapi-239291032No ratings yet
- Mémoire AI For The Recognition and Classification of Catastrophic ScenariosDocument116 pagesMémoire AI For The Recognition and Classification of Catastrophic ScenariosMohamed TekoukNo ratings yet
- Ut Slides.Document114 pagesUt Slides.Y ShameyaNo ratings yet
- Grade 316 316LDocument9 pagesGrade 316 316LvsajuNo ratings yet
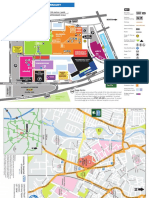
- Leicester Royal Infirmary: M1 M69 Football Stadium KEYDocument2 pagesLeicester Royal Infirmary: M1 M69 Football Stadium KEYpdhoppyNo ratings yet
- Computer Applications in ChemistryDocument16 pagesComputer Applications in ChemistryGanesh NNo ratings yet
- Assignment For Week 1 - 2022Document5 pagesAssignment For Week 1 - 2022Rajveer deepNo ratings yet
- Go Global Unix DatasheetDocument2 pagesGo Global Unix Datasheetthangdv82No ratings yet
- Ronald J. Adamson 1Document2 pagesRonald J. Adamson 1Dan BaumanNo ratings yet
- Soal B. Inggris Kls 10 Genap, 2023Document3 pagesSoal B. Inggris Kls 10 Genap, 2023smkterpadu insancitaNo ratings yet
- Potatoes: Free TemplatesDocument50 pagesPotatoes: Free TemplatesMichael AraujoNo ratings yet
- 4ES0 02 Rms 20120823Document9 pages4ES0 02 Rms 20120823Phyu Sin WinNo ratings yet
- Big Radiant Pointed Siar AfghanDocument4 pagesBig Radiant Pointed Siar AfghanbyronNo ratings yet
- Ad 2 Fapp enDocument12 pagesAd 2 Fapp enNagapranav Nagapranavm.jNo ratings yet
- Textile Industry in IndiaDocument97 pagesTextile Industry in IndiaDharmendra B MistryNo ratings yet
- 006 PLI - Form - Inspection Lifting GearDocument3 pages006 PLI - Form - Inspection Lifting GearRicky Stormbringer ChristianNo ratings yet
- Bangladesh Payment & Settlement System PDFDocument18 pagesBangladesh Payment & Settlement System PDFrokib0116No ratings yet
- FTII Acting Entance EXAM Notes - JET 2019Document61 pagesFTII Acting Entance EXAM Notes - JET 2019Vipul ShankarNo ratings yet
- Nx-8035-G7 Specification: Model Nutanix: Per Node ( (2) Per Block) NX-8035-G7 (Configure To Order)Document2 pagesNx-8035-G7 Specification: Model Nutanix: Per Node ( (2) Per Block) NX-8035-G7 (Configure To Order)Nazakat MallickNo ratings yet
- Caterpillar: Service ReportDocument1 pageCaterpillar: Service ReportUGINo ratings yet
- Unit 18 - Data Types and OrganizationDocument16 pagesUnit 18 - Data Types and OrganizationCLARA D SOUZA THOMASNo ratings yet