Download as pdf or txt
You might also like
- Steinberg - The Eye Is A Part of The Mind PDFDocument18 pagesSteinberg - The Eye Is A Part of The Mind PDFTimajosNo ratings yet
- Lab Safety WorksheetDocument2 pagesLab Safety WorksheetTcer Odah25% (4)
- AtelectasisDocument9 pagesAtelectasisArni ZulsitaNo ratings yet
- Atelectasis-Dr JokoDocument20 pagesAtelectasis-Dr JokoMamanHermawanNo ratings yet
- Atelectasis: Go ToDocument10 pagesAtelectasis: Go Tosuci triana putriNo ratings yet
- ATELECTASISDocument5 pagesATELECTASISAngellene GraceNo ratings yet
- The Respiratory SystemDocument8 pagesThe Respiratory SystemJane Rose SuperadaNo ratings yet
- Case Study On AtelectasisDocument14 pagesCase Study On AtelectasisSanhati Ghosh BanerjeeNo ratings yet
- Non-Rebreather MaskDocument15 pagesNon-Rebreather MaskKesyaNo ratings yet
- Plate-Like Atelectasis: PembimbingDocument5 pagesPlate-Like Atelectasis: Pembimbingandi140207No ratings yet
- Diagnostic Imaging Chest Sigfrido 2022-79-90Document12 pagesDiagnostic Imaging Chest Sigfrido 2022-79-90S ONo ratings yet
- Emphysema Is A LongDocument54 pagesEmphysema Is A LongryemoralesNo ratings yet
- Atelectasis Case Study Cajucom Reylibeth T.Document12 pagesAtelectasis Case Study Cajucom Reylibeth T.Prince Juzzel BanagNo ratings yet
- Emphysema Chronic Obstructive Pulmonary Disease (COPD) : Call Dasco Today For More Information 855-442-7912Document6 pagesEmphysema Chronic Obstructive Pulmonary Disease (COPD) : Call Dasco Today For More Information 855-442-7912Nazif Aiman IsmailNo ratings yet
- AtelectasisDocument4 pagesAtelectasisYanyan PanesNo ratings yet
- AtelectasisDocument2 pagesAtelectasisiMaibelle BelleNo ratings yet
- Depressed Level of Consciousness: Indicated Oxygenating Oxygen Supplementation Simple Face MaskDocument2 pagesDepressed Level of Consciousness: Indicated Oxygenating Oxygen Supplementation Simple Face MaskJhen Buenaflor LorenzoNo ratings yet
- AtelectasisDocument26 pagesAtelectasisArini NurlelaNo ratings yet
- Atelektasis Jurnal RadiologiDocument19 pagesAtelektasis Jurnal RadiologiRachmi MerrinaNo ratings yet
- Interstitial Lung DiseaseDocument14 pagesInterstitial Lung DiseaseAzkaZulfiqarNo ratings yet
- AtelectasisDocument24 pagesAtelectasisTiara RahmawatiNo ratings yet
- ATELECTASISDocument4 pagesATELECTASISAshley Jane MacapayadNo ratings yet
- PBL Respi 1 Week 1Document6 pagesPBL Respi 1 Week 1FrinkaWijayaNo ratings yet
- Atelectasis, (Lung Collapse) A Simple Guide To The Condition, Diagnosis, Treatment And Related DiseasesFrom EverandAtelectasis, (Lung Collapse) A Simple Guide To The Condition, Diagnosis, Treatment And Related DiseasesNo ratings yet
- Pulmonary Atelectasis: A Pathogenic Perioperative EntityDocument18 pagesPulmonary Atelectasis: A Pathogenic Perioperative Entityハルァン ファ烏山No ratings yet
- AtelectasisDocument30 pagesAtelectasisashoaib0313No ratings yet
- EMPHYSEMADocument2 pagesEMPHYSEMAJerick DaangNo ratings yet
- Medsurg Transes RespiratoryDocument17 pagesMedsurg Transes RespiratoryAprille Kaye TayoneNo ratings yet
- RespiratorDocument53 pagesRespiratorlianarodicaNo ratings yet
- Prenotes C23Document40 pagesPrenotes C23Erika Boots CabalunaNo ratings yet
- NCM 103 Aliasas AtelectasisDocument3 pagesNCM 103 Aliasas AtelectasisDARREN EDMARKNo ratings yet
- AtelectasisDocument12 pagesAtelectasisAureliaNo ratings yet
- AtelectasisDocument3 pagesAtelectasisMicah MagallanoNo ratings yet
- Approach To The Patient With DyspneaDocument22 pagesApproach To The Patient With DyspneaLuis Gerardo Alcalá GonzálezNo ratings yet
- Lecture 6 LungsDocument14 pagesLecture 6 LungsOsama MalikNo ratings yet
- Pulmonary DiseasesDocument36 pagesPulmonary DiseasescelecosibNo ratings yet
- Wheeze OlderDocument99 pagesWheeze OlderLaith AL-GurayfiiNo ratings yet
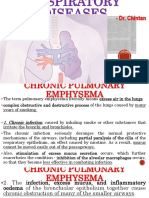
- Dr. ChintanDocument26 pagesDr. ChintanArshad KhanNo ratings yet
- Mechanisms of Atelectasis in The Perioperative PeriodDocument13 pagesMechanisms of Atelectasis in The Perioperative PeriodXavi Navarro FontNo ratings yet
- Atelectasis. Mechanisms, Diagnosis and Management (Peroni, 2000)Document5 pagesAtelectasis. Mechanisms, Diagnosis and Management (Peroni, 2000)Renato Li SoldevillaNo ratings yet
- Atelectasis (Collapse)Document6 pagesAtelectasis (Collapse)anojNo ratings yet
- Respiratory SystemDocument85 pagesRespiratory SystemDr:-Ustaad Aakass Ahmed Junejo SahabNo ratings yet
- What Does A Barrel Chest Indicate?Document3 pagesWhat Does A Barrel Chest Indicate?Moira Kelly SolangNo ratings yet
- Acute Respiratory Failure 1Document7 pagesAcute Respiratory Failure 1Trish 0019No ratings yet
- Ventilator Induced Lung Injury PreventionDocument8 pagesVentilator Induced Lung Injury Preventionapi-602219685No ratings yet
- Respiratory SystemDocument7 pagesRespiratory SystemLinh LeNo ratings yet
- Measurement of RV, FRC, TLC: Abu Ahmed 2019Document21 pagesMeasurement of RV, FRC, TLC: Abu Ahmed 2019Khalid AbdullahNo ratings yet
- Andrew Idoko Group 332 Variant 14Document5 pagesAndrew Idoko Group 332 Variant 14dreNo ratings yet
- GenPath Lab Activity 13 - ElsayedDocument9 pagesGenPath Lab Activity 13 - Elsayedabdallahtarek2000No ratings yet
- Airway ManagementDocument28 pagesAirway ManagementghazyNo ratings yet
- X Ray InterprationDocument6 pagesX Ray InterprationMelvita KurniawanNo ratings yet
- Radiology AssignmentDocument27 pagesRadiology AssignmentRoyce GonzagaNo ratings yet
- 07 (1) Pulmonary Effects of InhaledDocument46 pages07 (1) Pulmonary Effects of InhaledLeticia MeloNo ratings yet
- Bronchioles Then Divide Into Three TypesDocument3 pagesBronchioles Then Divide Into Three TypesJeremy EvansNo ratings yet
- Review Article: Expiratory Central Airway Collapse: A Concise ReviewDocument13 pagesReview Article: Expiratory Central Airway Collapse: A Concise ReviewfaberNo ratings yet
- 0000542-200504000-00021Document17 pages0000542-200504000-00021Daniel Martinez HernándezNo ratings yet
- Oxygenation and Airway Management: Quick LookDocument24 pagesOxygenation and Airway Management: Quick LookNining Komala SariNo ratings yet
- Atelectasis: Contraction Atelectasis (Or Cicatrization Atelectasis)Document10 pagesAtelectasis: Contraction Atelectasis (Or Cicatrization Atelectasis)Gan BangNo ratings yet
- Distress RespiratoriopdfDocument11 pagesDistress RespiratoriopdfDiana CarolinaNo ratings yet
- 4 Respiratory ExaminationsDocument53 pages4 Respiratory Examinationscawsey mohamedNo ratings yet
- Pulmonary Function Tests in Clinical PracticeFrom EverandPulmonary Function Tests in Clinical PracticeAli AltalagRating: 5 out of 5 stars5/5 (1)
- A Simple Guide to Pulmonary Infarction, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Pulmonary Infarction, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Pharmacy Content Bloxazoc-2020-09 FinalDocument8 pagesPharmacy Content Bloxazoc-2020-09 Finalهادي تركي شنبارةNo ratings yet
- 2nd Trial 2020Document1 page2nd Trial 2020هادي تركي شنبارةNo ratings yet
- اطفال فاينل 2021Document15 pagesاطفال فاينل 2021هادي تركي شنبارةNo ratings yet
- لقطة شاشة ٢٠٢١-٠٧-٣١ في ٤.٢٣.٤٩ مDocument1 pageلقطة شاشة ٢٠٢١-٠٧-٣١ في ٤.٢٣.٤٩ مهادي تركي شنبارةNo ratings yet
- TAD F.M.S - غير مقفلة 24 3 21Document3 pagesTAD F.M.S - غير مقفلة 24 3 21هادي تركي شنبارةNo ratings yet
- RDS 21-Sep-2019 22-27-42Document3 pagesRDS 21-Sep-2019 22-27-42هادي تركي شنبارةNo ratings yet
- Candidate Handbook 2021Document27 pagesCandidate Handbook 2021Jose Daniel NuñezNo ratings yet
- Eng Fixed Speed R45i 2013.08Document1 pageEng Fixed Speed R45i 2013.08Carlos JiménezNo ratings yet
- Most Suitable Mother Wavelet For Measurement of Power System Harmonics Using DWT in View of IEEE Standard 1459-2000Document6 pagesMost Suitable Mother Wavelet For Measurement of Power System Harmonics Using DWT in View of IEEE Standard 1459-2000Ivan BallesterosNo ratings yet
- Uvm TutorialDocument36 pagesUvm Tutorialravichettyravi100% (2)
- 22 10691 - BPSU CAT Confirmation SlipDocument1 page22 10691 - BPSU CAT Confirmation SlipJoryan VenturaNo ratings yet
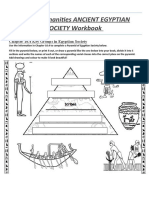
- ANCIENT EGYPTIAN SOCIETY WorkbookDocument7 pagesANCIENT EGYPTIAN SOCIETY WorkbookRick BartNo ratings yet
- Huawei Esight Brief Product Brochure (05-Sept-2013)Document8 pagesHuawei Esight Brief Product Brochure (05-Sept-2013)Tahitii ObiohaNo ratings yet
- Code Black Personal ThreatDocument2 pagesCode Black Personal ThreatpatientsafetyNo ratings yet
- MP CCIdocDocument933 pagesMP CCIdocMasterAlbus3dNo ratings yet
- Shakeeb Resume1Document3 pagesShakeeb Resume1Shakeeb AshaiNo ratings yet
- HP ZBOOK 17 QUICKSPECS c04111344Document45 pagesHP ZBOOK 17 QUICKSPECS c04111344hutz5000No ratings yet
- HUC Program Grading SchemeDocument1 pageHUC Program Grading SchemeThanis RaoNo ratings yet
- Mathematical Olympiad 2008-09Document29 pagesMathematical Olympiad 2008-09meatulin09No ratings yet
- Rail Movement Joints: Products DilatationenDocument0 pagesRail Movement Joints: Products DilatationenmarkicivanNo ratings yet
- Note On Marsh Crocodile, Presentation On Marsh Crocodile or Marsh Crocodile LifeDocument18 pagesNote On Marsh Crocodile, Presentation On Marsh Crocodile or Marsh Crocodile LifeKirfan 123No ratings yet
- Form 16: Warora Kurnool Transmission LimitedDocument10 pagesForm 16: Warora Kurnool Transmission LimitedBHASKAR pNo ratings yet
- Kosher 149 Complete Secular Book ListDocument434 pagesKosher 149 Complete Secular Book ListPond OfCraftsNo ratings yet
- Bryce Boerste - Personal College Essay - Draft 2Document3 pagesBryce Boerste - Personal College Essay - Draft 2api-492128881No ratings yet
- NCP For GERD (Risk For Aspiration)Document2 pagesNCP For GERD (Risk For Aspiration)Ma Kristina Apolonio63% (8)
- DTP HomeworkDocument6 pagesDTP Homeworkcffge1tw100% (1)
- Hys U14 and Above Coaching Player Development CurriculumDocument15 pagesHys U14 and Above Coaching Player Development CurriculumBogdan OpreaNo ratings yet
- Viichy France and The Resistance Culture & IdeologyDocument301 pagesViichy France and The Resistance Culture & IdeologyandybgNo ratings yet
- Maria Margaretha: Personal DetailDocument3 pagesMaria Margaretha: Personal DetailncocikaNo ratings yet
- EDN 2104-4 MidtermsDocument40 pagesEDN 2104-4 MidtermsJuls LolNo ratings yet
- Gazette SSCI A1 2023Document927 pagesGazette SSCI A1 2023Ahsan ShabirNo ratings yet
- Book Review of I Love You Since 1892Document2 pagesBook Review of I Love You Since 1892hannah100% (1)
- Filed - New York County Clerk 07 - 16 - 2012 Index No - 2012 Nyscef Doc. No. 25 Received Nyscef - 07 - 16 - 2012Document45 pagesFiled - New York County Clerk 07 - 16 - 2012 Index No - 2012 Nyscef Doc. No. 25 Received Nyscef - 07 - 16 - 2012MISSTY1027No ratings yet
- Recruitment and Selection Kamini-200Document98 pagesRecruitment and Selection Kamini-200Mohammad ShoebNo ratings yet