Download as pdf or txt
You might also like
- Child 20protection 20policy BB 2012Document27 pagesChild 20protection 20policy BB 2012imaan0% (1)
- QC and QA in Molecular LaboratoryDocument20 pagesQC and QA in Molecular LaboratoryMd. Minhazul IslamNo ratings yet
- SMK Bandar Sungai Petani 2021 Yearly Planner (Mapping Table) For English Language Form 5Document3 pagesSMK Bandar Sungai Petani 2021 Yearly Planner (Mapping Table) For English Language Form 5Siti Rohana Darus100% (1)
- Three Years' Experience of Quality Monitoring Program On Pre-Analytical Errors in ChinaDocument7 pagesThree Years' Experience of Quality Monitoring Program On Pre-Analytical Errors in ChinaCenyiqanita NurqanitaNo ratings yet
- Mistakes in A Stat Laboratory: Types and Frequency: Clinical Chemistry September 1997Document5 pagesMistakes in A Stat Laboratory: Types and Frequency: Clinical Chemistry September 1997Othman MaaiNo ratings yet
- Quality Improvement Measures As EffectivDocument9 pagesQuality Improvement Measures As EffectivSalman AbuzuhairaNo ratings yet
- Using Outlier Events To Monitor Test Turnaround TimeDocument8 pagesUsing Outlier Events To Monitor Test Turnaround TimeWilmer UcedaNo ratings yet
- 10.1515 - CCLM 2022 1143Document8 pages10.1515 - CCLM 2022 1143AraceliNo ratings yet
- QC in Lab ChapterDocument10 pagesQC in Lab ChapterSasabilNo ratings yet
- Bertholf2017 Chapter LaboratoryStructureAndFunctionDocument23 pagesBertholf2017 Chapter LaboratoryStructureAndFunctionci8084102No ratings yet
- Designing and Evaluating Autoverification Rules For Thyroid Function Profiles and Sex Hormone TestsDocument10 pagesDesigning and Evaluating Autoverification Rules For Thyroid Function Profiles and Sex Hormone TestsAli DokumaciogluNo ratings yet
- Internal Quality Control Practices in Coagulation LaboratoriesDocument10 pagesInternal Quality Control Practices in Coagulation LaboratoriesMy LeNo ratings yet
- Erdal-2017-The Economic Impact of Poor SampleDocument10 pagesErdal-2017-The Economic Impact of Poor SampleGökhanNo ratings yet
- 8-Encuesta Sobre Control de Calidad en Hematologia 2017Document11 pages8-Encuesta Sobre Control de Calidad en Hematologia 2017maxikuchtaNo ratings yet
- Application of Indices CP and CPK To Improve Quality Control Capability in Clinical Biochemistry LaboratoriesDocument6 pagesApplication of Indices CP and CPK To Improve Quality Control Capability in Clinical Biochemistry LaboratoriesMrinal BhandariNo ratings yet
- Challenges Towards Quality Improvement in Medical Laboratory Service in Nepal PDFDocument3 pagesChallenges Towards Quality Improvement in Medical Laboratory Service in Nepal PDFAngellaNo ratings yet
- Lot-To-Lot Variation and Verification - cclm-2022-1126Document8 pagesLot-To-Lot Variation and Verification - cclm-2022-1126Georgiana Daniela DragomirNo ratings yet
- Clinical Laboratory Analysis - 2020 - Tao - Research and Discussion On The Evaluation Scheme of Reagent Lot To LotDocument9 pagesClinical Laboratory Analysis - 2020 - Tao - Research and Discussion On The Evaluation Scheme of Reagent Lot To LotLorena Ek MaciasNo ratings yet
- Clinical Biochemistry: 10.1016/j.clinbiochem.2016.10.007Document13 pagesClinical Biochemistry: 10.1016/j.clinbiochem.2016.10.007MeryamNo ratings yet
- Plebani Etal 2014Document8 pagesPlebani Etal 2014vivi maykasariNo ratings yet
- SVERRE SANDBERG PoCT 2015 MXDocument35 pagesSVERRE SANDBERG PoCT 2015 MXMaaz HatimNo ratings yet
- Preanalytical Phase Management: Identification and Control of Nonconformities in The Sampling Room of A Clinical Laboratory in TunisiaDocument6 pagesPreanalytical Phase Management: Identification and Control of Nonconformities in The Sampling Room of A Clinical Laboratory in TunisiandogyenoubaNo ratings yet
- Laboratory Test Turnaround Time and The Needs of Medical CareDocument2 pagesLaboratory Test Turnaround Time and The Needs of Medical Caremy accountNo ratings yet
- JC Libeer JC Libeer Brussels, Belgium Brussels, BelgiumDocument63 pagesJC Libeer JC Libeer Brussels, Belgium Brussels, BelgiumJessa Marie EscalaNo ratings yet
- Quality Indicators in A Hematology Laboratory-A Retrospective AnalysisDocument6 pagesQuality Indicators in A Hematology Laboratory-A Retrospective AnalysisCenyiqanita NurqanitaNo ratings yet
- Pharmaceutical Sciences: Frequency of Pre-Analytical Phase Errors in A Clinical Chemistry LaboratoryDocument4 pagesPharmaceutical Sciences: Frequency of Pre-Analytical Phase Errors in A Clinical Chemistry LaboratoryAyesha MehmoodNo ratings yet
- Ce (Ad) F (Is) Pf1 (Aka SS) Pfa (SS) PN (SS)Document4 pagesCe (Ad) F (Is) Pf1 (Aka SS) Pfa (SS) PN (SS)marvel ecstasyNo ratings yet
- Biomed 24 3 376Document7 pagesBiomed 24 3 376adrianaNo ratings yet
- Effect of Accreditation On Accuracy of Diagnostic Tests in Medical LaboratoriesDocument10 pagesEffect of Accreditation On Accuracy of Diagnostic Tests in Medical LaboratoriesFira Dwi OktavianiNo ratings yet
- Characteristics of Diagnostic Laboratory in IndiaDocument10 pagesCharacteristics of Diagnostic Laboratory in IndiaArun Raj SNo ratings yet
- Especificaciones CliaDocument7 pagesEspecificaciones CliaNi Made KartiniNo ratings yet
- Critical Result ReportingDocument9 pagesCritical Result ReportingSafiqulatif AbdillahNo ratings yet
- A Matrix Model For Phlebotomy Quality AssuranceDocument15 pagesA Matrix Model For Phlebotomy Quality AssuranceandhiNo ratings yet
- POCT and PT by Group6bsmt3bDocument15 pagesPOCT and PT by Group6bsmt3bRuzzelle Mae ParasNo ratings yet
- What Causes Most Errors in Chemical AnalysisDocument2 pagesWhat Causes Most Errors in Chemical AnalysisImmerNo ratings yet
- Quality Control in A Clinical LaboratoryDocument9 pagesQuality Control in A Clinical LaboratoryHenry OseiNo ratings yet
- JOURNAL Errors in Clinical Laboratories or Errors in LaboratoryDocument11 pagesJOURNAL Errors in Clinical Laboratories or Errors in LaboratoryVincent ReyesNo ratings yet
- A Review of Medical Errors in Laboratory Diagnostics and Where We Are TodayDocument7 pagesA Review of Medical Errors in Laboratory Diagnostics and Where We Are TodayRobert MaynardNo ratings yet
- Analysis of Laboratory Critical Value Reporting at A Large Academic Medical CenterDocument7 pagesAnalysis of Laboratory Critical Value Reporting at A Large Academic Medical CenterLevi GasparNo ratings yet
- Practical Laboratory Medicine: Julie L.V. ShawDocument8 pagesPractical Laboratory Medicine: Julie L.V. ShawJamesNo ratings yet
- The Quality of Laboratory Testing TodayDocument13 pagesThe Quality of Laboratory Testing TodaysantoshelapandaNo ratings yet
- TAT Pre AnalitikDocument6 pagesTAT Pre AnalitikPOKJA PPNo ratings yet
- Good Clinical Laboratory Practice (GCLP) : Quality Demanding From Clinical LaboratoriesDocument5 pagesGood Clinical Laboratory Practice (GCLP) : Quality Demanding From Clinical LaboratoriesJaneNo ratings yet
- Quality Control For Chemistry Laboratory - Dynacare Kasper Laboratories ProceduresDocument11 pagesQuality Control For Chemistry Laboratory - Dynacare Kasper Laboratories ProceduresyonisNo ratings yet
- Ajcpath125 0016Document10 pagesAjcpath125 0016Asad AliNo ratings yet
- Quality Assessment of Interpretative Commenting and Competency Comparison of Comment Providers in ChinaDocument6 pagesQuality Assessment of Interpretative Commenting and Competency Comparison of Comment Providers in ChinaamyNo ratings yet
- Ejifcc 26 190Document7 pagesEjifcc 26 190Tiurma SimamoraNo ratings yet
- Defining A Roadmap For Harmonizing QualiDocument11 pagesDefining A Roadmap For Harmonizing QualiSalman AbuzuhairaNo ratings yet
- Tugas 1Document9 pagesTugas 1Ramadhan OlongNo ratings yet
- QC and QA in Molecular LaboratoryDocument20 pagesQC and QA in Molecular LaboratoryMd. Minhazul IslamNo ratings yet
- eJIFCC2023Vol34No3pp203 212Document10 pageseJIFCC2023Vol34No3pp203 212joudi.jou95No ratings yet
- Using Lean Principles To Optimise Inpatient Phlebotomy ServicesDocument7 pagesUsing Lean Principles To Optimise Inpatient Phlebotomy ServicesMuizzuddin MuizNo ratings yet
- PlebaniDocument2 pagesPlebaniGrescia Ramos VegaNo ratings yet
- Errors in Clinical Laboratories or Errors in Laboratory MedicineDocument11 pagesErrors in Clinical Laboratories or Errors in Laboratory MedicineShahid HussainNo ratings yet
- Errors in Clinical Laboratories or Errors in Laboratory Medicine?Document10 pagesErrors in Clinical Laboratories or Errors in Laboratory Medicine?DiegoMaradónNo ratings yet
- Installation and Implementation of Automation and Its Impact On Clinical Chemistry Laboratory ProductivityDocument4 pagesInstallation and Implementation of Automation and Its Impact On Clinical Chemistry Laboratory ProductivityMuhammad Hanzalah AtifNo ratings yet
- Quality Assurance of Laboratory Results: A Challenge in Health Care ManagementDocument6 pagesQuality Assurance of Laboratory Results: A Challenge in Health Care Managementrizkiyah prabawantiNo ratings yet
- A Review of Medical Errors in Laboratory Diagnostics and Where We Are TodayDocument4 pagesA Review of Medical Errors in Laboratory Diagnostics and Where We Are TodayShahid HussainNo ratings yet
- GPP Pipetting Calibration and Technique ENDocument4 pagesGPP Pipetting Calibration and Technique ENveneta gizdakovaNo ratings yet
- Final Printing Version Sept 2009 A Practical Guide To IQC HKAMLDocument48 pagesFinal Printing Version Sept 2009 A Practical Guide To IQC HKAMLMSKNo ratings yet
- Quality Control in HistopathologyDocument30 pagesQuality Control in HistopathologyMuhammad Jamiu Bello78% (9)
- Analytical Method Validation and Instrument Performance VerificationFrom EverandAnalytical Method Validation and Instrument Performance VerificationNo ratings yet
- ENGLISH 9 DLP For DEMODocument9 pagesENGLISH 9 DLP For DEMOMary Joy Corpuz100% (2)
- Mark SheetDocument1 pageMark SheetLokeshNo ratings yet
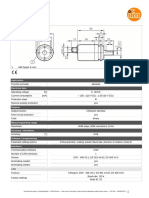
- Multiturn Solid Shaft Encoder: 1 M4 Depth 6 MMDocument2 pagesMultiturn Solid Shaft Encoder: 1 M4 Depth 6 MMSoha EzzaldenNo ratings yet
- CJR FILSAFAT Sem 1Document17 pagesCJR FILSAFAT Sem 1Jesica RaivitaNo ratings yet
- Dashboard Digital VoltmeterDocument7 pagesDashboard Digital VoltmetercrashoveriteNo ratings yet
- Ship Maintenance Planning With NavCadDocument4 pagesShip Maintenance Planning With NavCadtheleepiper8830No ratings yet
- E-Learning Tender RFPDocument41 pagesE-Learning Tender RFPnaidu naga nareshNo ratings yet
- Vdocuments - MX - Toyota 8fg45n Forklift Service Repair Manual 1608089928 PDFDocument23 pagesVdocuments - MX - Toyota 8fg45n Forklift Service Repair Manual 1608089928 PDFGUILHERME SANTOSNo ratings yet
- Design of A Dumping GrateDocument13 pagesDesign of A Dumping GrateABDULLAH MAQBOOL100% (1)
- Metrics For It Service ManagementDocument11 pagesMetrics For It Service ManagementTomas Hernandez100% (1)
- Devops MCQ PDFDocument6 pagesDevops MCQ PDFSaad Mohamed SaadNo ratings yet
- (Adi Kuntsman (Eds.) ) Selfie CitizenshipDocument169 pages(Adi Kuntsman (Eds.) ) Selfie CitizenshipUğur GündüzNo ratings yet
- Scrap Specifications CircularDocument57 pagesScrap Specifications Circulargiám địnhNo ratings yet
- DK Selling StrategiesDocument7 pagesDK Selling StrategiesMilan DzigurskiNo ratings yet
- An Introduction To Augmented Reality Aided ManufacturingDocument29 pagesAn Introduction To Augmented Reality Aided ManufacturingSahilNo ratings yet
- CBT Body of Knowledge - Rev0Document7 pagesCBT Body of Knowledge - Rev0Partha Sarathi Sadhukhan0% (1)
- शिक्षामनोविज्ञानDocument2 pagesशिक्षामनोविज्ञानlalit sharmaNo ratings yet
- Gradlew of ResourcesDocument43 pagesGradlew of ResourceswepehyduNo ratings yet
- Meeting Minutes of 17th Departmental MeetingDocument3 pagesMeeting Minutes of 17th Departmental Meetingmyousafzai67No ratings yet
- Purpose and Objectives of Starting Up A Project ProcessDocument2 pagesPurpose and Objectives of Starting Up A Project ProcessSocrates KontosNo ratings yet
- Water and Slurry Bulkheads in Underground Coal Mines: Design, Monitoring and Safety ConcernsDocument7 pagesWater and Slurry Bulkheads in Underground Coal Mines: Design, Monitoring and Safety ConcernsDinesh dhakarNo ratings yet
- The Roots of Modern Feminism: Mary Wollstonecraft and The French RevolutionDocument16 pagesThe Roots of Modern Feminism: Mary Wollstonecraft and The French RevolutionShirlya LimaNo ratings yet
- Parametric & Non Parametric TestDocument8 pagesParametric & Non Parametric TestAngelica Alejandro100% (1)
- Flight1 DC-9 Power SettingsDocument2 pagesFlight1 DC-9 Power SettingsAlfonso MayaNo ratings yet
- I Series FuserDocument2 pagesI Series FuserxerotecNo ratings yet
- PS GrammarDocument3 pagesPS GrammarMastermind SunnyNo ratings yet
- Self-Efficacy Mediated Spiritual Leadership On Citizenship Behavior Towards The Environment of Employees at Harapan Keluarga HospitalDocument7 pagesSelf-Efficacy Mediated Spiritual Leadership On Citizenship Behavior Towards The Environment of Employees at Harapan Keluarga HospitalInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Project Product DescriptionDocument5 pagesProject Product Descriptionpruebaproiba12No ratings yet