Download as doc, pdf, or txt
You might also like
- PPAP 3rd Edition Check List: PPAPKIT - F01 Rev. A (May - 03)Document6 pagesPPAP 3rd Edition Check List: PPAPKIT - F01 Rev. A (May - 03)api-3832465100% (5)
- APQP ChecklistDocument18 pagesAPQP ChecklistmichaelbarkovicNo ratings yet
- CSSBB Cert Project AffidavitDocument2 pagesCSSBB Cert Project AffidavitJOSE LUISNo ratings yet
- Responsibility Rank of Development: D:/APQP Document/ Special Product and Process CharactesticsDocument4 pagesResponsibility Rank of Development: D:/APQP Document/ Special Product and Process CharactesticsAL BARAKAH GRAINS100% (1)
- IQA Audit ChecklistDocument26 pagesIQA Audit Checklistnorlie100% (1)
- SAP PR Release Strategy Concept and Configuration Guide: A Case StudyFrom EverandSAP PR Release Strategy Concept and Configuration Guide: A Case StudyRating: 4 out of 5 stars4/5 (6)
- This Study Resource Was: Consumer Behavior ExercisesDocument2 pagesThis Study Resource Was: Consumer Behavior ExercisesSebika BoharaNo ratings yet
- The Use of BondsDocument8 pagesThe Use of BondsDarius Rashaud86% (7)
- FM-NM-014 ECN - NoticeDocument1 pageFM-NM-014 ECN - Noticephutthawongdanchai041215No ratings yet
- Corrective and Preventive Action (Capa)Document6 pagesCorrective and Preventive Action (Capa)Nishit SuvaNo ratings yet
- Format 10 - Part Submission Warrant1Document2 pagesFormat 10 - Part Submission Warrant1vijayNo ratings yet
- Part Submission WarrantDocument4 pagesPart Submission WarrantSam AnuNo ratings yet
- Supplier Claim Flow ChecklistDocument1 pageSupplier Claim Flow ChecklistChris GloverNo ratings yet
- Assessment Readiness Review Checklist ISO/IEC 17025:2017Document3 pagesAssessment Readiness Review Checklist ISO/IEC 17025:2017Sarah Jane BroñolaNo ratings yet
- RO-RG80-00031 - Rev H, JPPAP Templates (Jabil Production Part Approval Process)Document38 pagesRO-RG80-00031 - Rev H, JPPAP Templates (Jabil Production Part Approval Process)KM MuiNo ratings yet
- Automatic Account Determination - SCN PDFDocument8 pagesAutomatic Account Determination - SCN PDFKristian SanchezchavezNo ratings yet
- MP EnglishDocument25 pagesMP EnglishDubilio AlfonzoNo ratings yet
- SOP For Change Control - Pharmaceutical GuidelinesDocument4 pagesSOP For Change Control - Pharmaceutical Guidelinesmanspa2014No ratings yet
- New Blank CarsDocument1 pageNew Blank CarsNelianie Bangtuan50% (2)
- Analyser FATDocument25 pagesAnalyser FATGeo Thaliath100% (1)
- Coral Laboratories Limited: Plot No 27-28, Pharmacity, Selaqui, Dehradun 248197 (Uttarakhand) SOP/QA/071 R-02 1 of 2Document2 pagesCoral Laboratories Limited: Plot No 27-28, Pharmacity, Selaqui, Dehradun 248197 (Uttarakhand) SOP/QA/071 R-02 1 of 2QA Doon100% (1)
- Competency Assessment Results Summary-FINALDocument1 pageCompetency Assessment Results Summary-FINALMark Aldwin LopezNo ratings yet
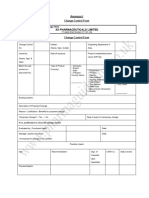
- Annexure I Change Control FormDocument4 pagesAnnexure I Change Control FormSÜMME AÇIKGÖZNo ratings yet
- CTRL Plan TemplateDocument4 pagesCTRL Plan TemplatevishalNo ratings yet
- RFIA Formrev00 (BP02B)Document2 pagesRFIA Formrev00 (BP02B)721917114 47No ratings yet
- SAP Implementation Project Functional Specification - Factura V1.0Document9 pagesSAP Implementation Project Functional Specification - Factura V1.0DamianSpagnulNo ratings yet
- Phased Ps Wwith P Pap Tracking FormDocument3 pagesPhased Ps Wwith P Pap Tracking FormKurt FinkNo ratings yet
- QCC+Application Registration+FormDocument4 pagesQCC+Application Registration+FormrajaabidNo ratings yet
- 04 Supplier Qualification StatementDocument2 pages04 Supplier Qualification StatementSujith KSNo ratings yet
- Engineering Change Order FormDocument1 pageEngineering Change Order Formaborder-06-sonnetNo ratings yet
- NC TemplateDocument1 pageNC TemplateSupun ChanakaNo ratings yet
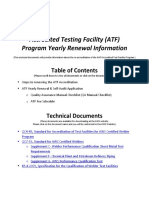
- ATF Yearly Renewal AppDocument7 pagesATF Yearly Renewal AppkumarNo ratings yet
- NABB FORMS WatermarkDocument35 pagesNABB FORMS Watermarkmarjan 01100% (1)
- EFDK908059Document1 pageEFDK908059vinwinchem84No ratings yet
- AC7126-1 Rev B 23-AUG-2016Document26 pagesAC7126-1 Rev B 23-AUG-2016unknown1711No ratings yet
- Sec 8b P Vend InspectDocument6 pagesSec 8b P Vend InspectJagan BoseNo ratings yet
- Job Order and Document Review Format (Document93 pagesJob Order and Document Review Format (Ami AluminiumNo ratings yet
- Docsity Formatos de Apqp para Su Llenado y Aplicado 1Document64 pagesDocsity Formatos de Apqp para Su Llenado y Aplicado 1Alejandro Martinez OrtegaNo ratings yet
- Appendix B - 20100903 - 145453Document25 pagesAppendix B - 20100903 - 145453AkoKhalediNo ratings yet
- APPENDIX-I (Request Sheet)Document2 pagesAPPENDIX-I (Request Sheet)iloveit52252No ratings yet
- Inspection Report BG/QA/FRM-04/13 Rev:00: (Clients/Consultants) Project ManagerDocument1 pageInspection Report BG/QA/FRM-04/13 Rev:00: (Clients/Consultants) Project ManagerYousaf RichuNo ratings yet
- ACC QF 07 Documentary Requirements For Liquidations MOOE PRINTING AND PUBLICATIONSDocument1 pageACC QF 07 Documentary Requirements For Liquidations MOOE PRINTING AND PUBLICATIONSRenabeth GuillermoNo ratings yet
- Apr Form No. 02Document4 pagesApr Form No. 02Francis Gavin Delos ReyesNo ratings yet
- Inspection Test PlanDocument4 pagesInspection Test PlanJay Gaspar Jr.No ratings yet
- General SOP No. 001Document10 pagesGeneral SOP No. 001sohankumar.mahaleNo ratings yet
- ACD-BOA-05 Rev 01 App Form Acc of Individual CPADocument3 pagesACD-BOA-05 Rev 01 App Form Acc of Individual CPAPrinchipe ni BebangNo ratings yet
- SOP For Corrective Action and Preventive Action (CAPA) - Pharmaceutical GuidelinesDocument5 pagesSOP For Corrective Action and Preventive Action (CAPA) - Pharmaceutical GuidelinesAmit KumarNo ratings yet
- Cntlplan 5Document6 pagesCntlplan 5sumeetsaini88No ratings yet
- 8 Borang - Borang (Eps 1 - 9)Document12 pages8 Borang - Borang (Eps 1 - 9)faizal mohdNo ratings yet
- 2 DepedDocument15 pages2 DepedSir Cris CapiliNo ratings yet
- Application Form For Environmental Clearance For Various ActivitiesDocument1 pageApplication Form For Environmental Clearance For Various Activitiesanya Bobadilla (anyaxanyax)No ratings yet
- Final Year Project Title Proposal: Appendix 3-1ADocument26 pagesFinal Year Project Title Proposal: Appendix 3-1ADinnassh GaneshNo ratings yet
- Corrective and Preventive Action (CAPA) Report: Customer: AddressDocument4 pagesCorrective and Preventive Action (CAPA) Report: Customer: Addressnarita purbawanaNo ratings yet
- Apqp Matrix UpdatedDocument2 pagesApqp Matrix Updatedabhishek100% (1)
- 2024 WRFDocument1 page2024 WRFjessecalacorteNo ratings yet
- UC 8000015775 TS NEdM 019 - MM - CONV-Upload Massive ContractsDocument8 pagesUC 8000015775 TS NEdM 019 - MM - CONV-Upload Massive ContractsErick ViteNo ratings yet
- GAD Construction PLC. Material Requisition FormDocument1 pageGAD Construction PLC. Material Requisition FormARSENo ratings yet
- Agency Procurement Request: Please Check ( ) Appropriate Box On Action Requested On The Item/S Listed BelowDocument2 pagesAgency Procurement Request: Please Check ( ) Appropriate Box On Action Requested On The Item/S Listed BelowBrianSantiagoNo ratings yet
- QMS IA Report - NRL C1C2Document10 pagesQMS IA Report - NRL C1C2R Sahadeo ReddyNo ratings yet
- 10 CFR 21 Potential Defect ChecklistDocument6 pages10 CFR 21 Potential Defect ChecklistCharles Bill Eldredge100% (1)
- SOP On Handling of Non-Conformances - Pharma PathwayDocument22 pagesSOP On Handling of Non-Conformances - Pharma Pathwayshaksganeshan100% (1)
- Checklist AcDocument2 pagesChecklist AcMICS TVNo ratings yet
- TMH 22 Road Asset Management Manual SummaryDocument31 pagesTMH 22 Road Asset Management Manual SummaryTawandaNo ratings yet
- Tecewn 3002Document589 pagesTecewn 3002Cristea CalinNo ratings yet
- Element 2Document2 pagesElement 2Wafula RobertNo ratings yet
- Financial Statements Analysis - An IntroductionDocument19 pagesFinancial Statements Analysis - An Introductionbiniam meazanehNo ratings yet
- SAGRADA ORDEN DE PREDICADORES DEL SANTISIMO ROSARIO DE FILIPINAS vs. National Coconut CorporationDocument2 pagesSAGRADA ORDEN DE PREDICADORES DEL SANTISIMO ROSARIO DE FILIPINAS vs. National Coconut CorporationRiza AkkangNo ratings yet
- Philippine Taxation and The History of The Bureau of Internal RevenueDocument8 pagesPhilippine Taxation and The History of The Bureau of Internal RevenuejohnNo ratings yet
- PWC News Alert 6 May 2015 Chennai Properties Investments LimitedDocument3 pagesPWC News Alert 6 May 2015 Chennai Properties Investments LimitedSunil SinghNo ratings yet
- Effect of Product Quality, Price, and Promotion To Purchase DecisionDocument14 pagesEffect of Product Quality, Price, and Promotion To Purchase DecisionCeline HaNo ratings yet
- SKF Training Solutions Catalogue: Dates and Locations PreviewDocument48 pagesSKF Training Solutions Catalogue: Dates and Locations PreviewEDI PRASETYONo ratings yet
- SQF Quality Code Ed 8.1Document49 pagesSQF Quality Code Ed 8.1Luis GallegosNo ratings yet
- Aa Aca 01 PDFDocument2 pagesAa Aca 01 PDFKaren Brioso FajardoNo ratings yet
- Machinery and Machine Guarding ProgramDocument35 pagesMachinery and Machine Guarding ProgramBenson Harison MajabeNo ratings yet
- Mohsin Hassan Bba Iib BUS-19F-044 Principle of AccountingDocument7 pagesMohsin Hassan Bba Iib BUS-19F-044 Principle of AccountingMohsin HassanNo ratings yet
- CH 6Document32 pagesCH 6Vince Kristofer P. BrilNo ratings yet
- CHP 8: Managerial Accounting Edisi 11 by Hilton & PlattDocument44 pagesCHP 8: Managerial Accounting Edisi 11 by Hilton & Plattayu umyanaNo ratings yet
- HDFC Bank - Salary Account Offer Letter - Premium With Millennia DebitDocument16 pagesHDFC Bank - Salary Account Offer Letter - Premium With Millennia DebitSrinivasan candbNo ratings yet
- Math 10-3 Unit 1.4 Worksheet - Sales 2018-19 W - KEYDocument8 pagesMath 10-3 Unit 1.4 Worksheet - Sales 2018-19 W - KEYBob SmynameNo ratings yet
- Implications of The Coming Capex in Coal - Fundoo ProfessorDocument1 pageImplications of The Coming Capex in Coal - Fundoo ProfessorSubham JainNo ratings yet
- Supply Chain Management: Dr. Sunil SharmaDocument15 pagesSupply Chain Management: Dr. Sunil SharmaAmit Halder 2020-22No ratings yet
- Stvep Entrep Grade9 Qtr4 Module2-Lesson3-4Document13 pagesStvep Entrep Grade9 Qtr4 Module2-Lesson3-4Poseidon NipNo ratings yet
- EUROUZ Market Report On Uzbekistan For May 2022Document34 pagesEUROUZ Market Report On Uzbekistan For May 2022Adhithya MuthusamyNo ratings yet
- Ultra Modern Commercial Complex: WWW - Shrivinayaka.inDocument18 pagesUltra Modern Commercial Complex: WWW - Shrivinayaka.inSurendra SharmaNo ratings yet
- CW Catalogue IN EN 2012Document64 pagesCW Catalogue IN EN 2012emiliano ZappaterraNo ratings yet
- Aayushi Verma ResumeDocument2 pagesAayushi Verma ResumeAman ChoudharyNo ratings yet
- The Future of Knowledge WorkDocument18 pagesThe Future of Knowledge WorkAnand VermaNo ratings yet
- Mixed Model Assembly: by Quarterman Lee, P.E. Strategos, IncDocument27 pagesMixed Model Assembly: by Quarterman Lee, P.E. Strategos, IncTushar Ballabh BMLNo ratings yet
- Conducting Marketing Research and Forecasting DemandDocument56 pagesConducting Marketing Research and Forecasting DemandMark Allan Meriales100% (1)
- "Sales & Marketing": Stainless Steel Kichen SinksDocument5 pages"Sales & Marketing": Stainless Steel Kichen SinksDEEPAKNo ratings yet