Download as pdf or txt
You might also like
- Forensics: 3: Anthropology Lab Name: Section: Objectives: Science: AnatomyDocument6 pagesForensics: 3: Anthropology Lab Name: Section: Objectives: Science: AnatomyMargene SmithNo ratings yet
- Meindl, R.S. Et Al. 1985 Accuracy and Direction of Error in The Sexing of The SkeletonDocument7 pagesMeindl, R.S. Et Al. 1985 Accuracy and Direction of Error in The Sexing of The SkeletonElen FeuerriegelNo ratings yet
- Nature Versus Nurture and The Gender Divide PDFDocument18 pagesNature Versus Nurture and The Gender Divide PDFMishaal100% (1)
- Maxillary Suture Obliteration A Visual Mehtod For Estimating Skeletal AgeDocument9 pagesMaxillary Suture Obliteration A Visual Mehtod For Estimating Skeletal AgeIsolda Alanna RlNo ratings yet
- CARIOLOGYDocument77 pagesCARIOLOGYteklay100% (3)
- Skeletal Remains Determination of Age, SexDocument12 pagesSkeletal Remains Determination of Age, Sexyuraekang994No ratings yet
- Sex Determination From Skeletal Remains - Forensic's BlogDocument10 pagesSex Determination From Skeletal Remains - Forensic's BlogReal AbrasNo ratings yet
- Final Copy Bone DetectivesDocument9 pagesFinal Copy Bone Detectivesapi-313335831No ratings yet
- Forensic AnthrolopogyDocument7 pagesForensic Anthrolopogytmxqgk5cd4No ratings yet
- Sex Redefined - Revista NatureDocument4 pagesSex Redefined - Revista NatureWilliam Harris100% (1)
- Sex Estimation From The Calcaneus and Talus 2019Document20 pagesSex Estimation From The Calcaneus and Talus 2019marjaba2403No ratings yet
- Sex Redefined - The Idea of 2 Sexes Is Overly Simplistic - Scientific AmericanDocument10 pagesSex Redefined - The Idea of 2 Sexes Is Overly Simplistic - Scientific AmericanAndrew ButtressNo ratings yet
- 46, XY PersonsDocument16 pages46, XY Personsagustin cassinoNo ratings yet
- Craniofacial Growth, Maturation, and Change: Teens To MidadulthoodDocument4 pagesCraniofacial Growth, Maturation, and Change: Teens To MidadulthoodOmar DSNo ratings yet
- Walrath Et Al. 2004Document6 pagesWalrath Et Al. 2004Sabine BascurNo ratings yet
- Evidence Supporting The Biological Nature of Gender IdentityDocument6 pagesEvidence Supporting The Biological Nature of Gender IdentityMorgan Atwood100% (2)
- Walker 2008 Cranial SexDocument12 pagesWalker 2008 Cranial SextrutiNo ratings yet
- Technical Note: J. T. Burnham, 1 M - A - Judith Preston-Burnham, ' B.S. and C. R. Fontan, ' B.S., D. CrimDocument3 pagesTechnical Note: J. T. Burnham, 1 M - A - Judith Preston-Burnham, ' B.S. and C. R. Fontan, ' B.S., D. CrimCorina ArmanuNo ratings yet
- Biology Feynman TechniquesDocument9 pagesBiology Feynman TechniquesmuthulaxmiNo ratings yet
- Hecht 2020Document13 pagesHecht 2020api-507790153No ratings yet
- Biological Theories of Gender: HormonesDocument8 pagesBiological Theories of Gender: HormonesDanica De VeraNo ratings yet
- Understanding Genetic, Morphological, and Physiological Variation 1Document11 pagesUnderstanding Genetic, Morphological, and Physiological Variation 1api-265633268No ratings yet
- Sexing The Human Skull Through TheDocument6 pagesSexing The Human Skull Through ThelasaavedraNo ratings yet
- Forensic Anthropology HandoutDocument11 pagesForensic Anthropology HandoutSuzan100% (1)
- Atlas of Developmental Field Anomalies of the Human Skeleton: A Paleopathology PerspectiveFrom EverandAtlas of Developmental Field Anomalies of the Human Skeleton: A Paleopathology PerspectiveNo ratings yet
- Hassel Et Al 1995 CVSMDocument9 pagesHassel Et Al 1995 CVSMVicente ContrerasNo ratings yet
- Measures of Man Exam 2 Study GuideDocument5 pagesMeasures of Man Exam 2 Study GuideKennon RudeNo ratings yet
- Biological Theories of GenderDocument9 pagesBiological Theories of GenderAnalyn MacalaladNo ratings yet
- EVIDENCE SUPPORTING BIO NATURE OF GENDER IDENTITY - Saraswat & SaferDocument20 pagesEVIDENCE SUPPORTING BIO NATURE OF GENDER IDENTITY - Saraswat & Safercrosskeys001No ratings yet
- 6 A Human Craniofacial Life-Course Cross-Sectionalmorphological Covariations During Postnatal Growth, Adolescence, and AgingDocument19 pages6 A Human Craniofacial Life-Course Cross-Sectionalmorphological Covariations During Postnatal Growth, Adolescence, and AgingSebastian GuevaraNo ratings yet
- Sexual Selection Final DraftDocument10 pagesSexual Selection Final DraftntankardNo ratings yet
- Homosexual Orientation. The Search For A Biological Basis.: References ReprintsDocument5 pagesHomosexual Orientation. The Search For A Biological Basis.: References ReprintsMaria Isabel Montañez RestrepoNo ratings yet
- Biological Theories of Gender: HormonesDocument8 pagesBiological Theories of Gender: HormonesMaeNo ratings yet
- Alternative Methods For Identifiying SexDocument16 pagesAlternative Methods For Identifiying SexFaizan Rashid LoneNo ratings yet
- Kamasutra in Practice The Use of Sexual Positions in The CzechDocument10 pagesKamasutra in Practice The Use of Sexual Positions in The CzechYoga PrabawaNo ratings yet
- Psychology Today Male Brain, Female Brain The Hidden Difference Gender Does Affect How Our Brains Work - But in Surprising WaysDocument3 pagesPsychology Today Male Brain, Female Brain The Hidden Difference Gender Does Affect How Our Brains Work - But in Surprising WaysMichael HubbertNo ratings yet
- Man - WikipediaDocument11 pagesMan - WikipediaChaudhary TamannaNo ratings yet
- Ex Differences Brain: in TheDocument6 pagesEx Differences Brain: in TheAnibel VilchezNo ratings yet
- Xy Sex Determination SystemDocument7 pagesXy Sex Determination Systemafricano cregNo ratings yet
- A Morphometric Study of The Human Mandible in The Indian Population For Sex DeterminationDocument5 pagesA Morphometric Study of The Human Mandible in The Indian Population For Sex DeterminationBRYAN JESÚSNo ratings yet
- History of Commercializing Sexed Semen FDocument10 pagesHistory of Commercializing Sexed Semen FNikson Rafael AmosNo ratings yet
- Ch9 GaygeneDocument10 pagesCh9 GaygeneMbiami HermanNo ratings yet
- Sex Determination: Why So Many Ways of Doing It?: EssayDocument13 pagesSex Determination: Why So Many Ways of Doing It?: EssayCippalippaNo ratings yet
- Schutkowski 1993Document8 pagesSchutkowski 1993MilosFrostRadovicNo ratings yet
- Brain Structure Changes Associated With Sexual OrientationDocument10 pagesBrain Structure Changes Associated With Sexual Orientationdbozturk05No ratings yet
- Why Sex Hormones Matter For NeuroscienceDocument10 pagesWhy Sex Hormones Matter For NeuroscienceМакар РогатковNo ratings yet
- Sex & Vision I: Spatio-Temporal Resolution: Research Open AccessDocument14 pagesSex & Vision I: Spatio-Temporal Resolution: Research Open AccesstiganiadaNo ratings yet
- Metodo de BruzekDocument35 pagesMetodo de BruzekosteologyNo ratings yet
- 03 Rusyad - Dimorfisme Seksual - Editan Tyas MdaDocument19 pages03 Rusyad - Dimorfisme Seksual - Editan Tyas MdaWimo Dwi MurtopoNo ratings yet
- Sexual Dimorphism in Adult Human Mandible of North Indian OriginDocument7 pagesSexual Dimorphism in Adult Human Mandible of North Indian OriginMatheus CorreaNo ratings yet
- Mapping Sexual Dimorphism Signal in The Human CraniumDocument11 pagesMapping Sexual Dimorphism Signal in The Human CraniumAntonio ProficoNo ratings yet
- Selection and Separation of X - and Y - Chromosome-Bearing Mammalian Sperm.Document19 pagesSelection and Separation of X - and Y - Chromosome-Bearing Mammalian Sperm.Joel JohnNo ratings yet
- Omani Inventions 1Document8 pagesOmani Inventions 1Nichole TurkNo ratings yet
- Endo 2937Document11 pagesEndo 2937Corina ElenaNo ratings yet
- Fetal Testosterone and Sex Differences: Rebecca Christine Knickmeyer, Simon Baron-CohenDocument6 pagesFetal Testosterone and Sex Differences: Rebecca Christine Knickmeyer, Simon Baron-CohenPollich-Pap ZsuzsannaNo ratings yet
- Naturalizing As An Error-Type in Biology: Douglas AllchinDocument23 pagesNaturalizing As An Error-Type in Biology: Douglas AllchinWillyans MacielNo ratings yet
- DNA ChangesDocument4 pagesDNA Changesskymate64No ratings yet
- NANTHINIDocument28 pagesNANTHINIADHITHIYA VNo ratings yet
- Age-And Gender-Related Variations in Morphometric Characteristics of Thoracic Spine Pedicle: A Study of 4,800 PediclesDocument10 pagesAge-And Gender-Related Variations in Morphometric Characteristics of Thoracic Spine Pedicle: A Study of 4,800 PediclesLê Xuân SangNo ratings yet
- Legal Med FinalDocument56 pagesLegal Med Finalvishnu SNo ratings yet
- Vitt & Vangilder (1983) - Ecology of Snake Community in The Northeastern BrazilDocument24 pagesVitt & Vangilder (1983) - Ecology of Snake Community in The Northeastern BrazilEd MyersNo ratings yet
- Nanotechnology Optical Tweezers ReportDocument13 pagesNanotechnology Optical Tweezers ReportDaria RomanNo ratings yet
- Teal Sheets Addendum 02 - 2008Document2 pagesTeal Sheets Addendum 02 - 2008joséNo ratings yet
- Cerebral PalsyDocument511 pagesCerebral PalsyDwi Nilamsari100% (2)
- DISLIPIDEMIA112Document20 pagesDISLIPIDEMIA112Apotek TribrataNo ratings yet
- Heterospory in PteridophytesDocument4 pagesHeterospory in PteridophytesTANMOY SARKARNo ratings yet
- David M. Buss, Joshua D. Duntley (Auth.), Todd K. Shackelford, Ranald D. Hansen (Eds.) - The Evolution of Violence-Springer-Verlag New York (2014)Document250 pagesDavid M. Buss, Joshua D. Duntley (Auth.), Todd K. Shackelford, Ranald D. Hansen (Eds.) - The Evolution of Violence-Springer-Verlag New York (2014)supernezNo ratings yet
- Relevance of Menarche, Menopause, and Other Bioevent To FertilityDocument3 pagesRelevance of Menarche, Menopause, and Other Bioevent To FertilitydattaniranjanNo ratings yet
- Maternal Notes 1Document34 pagesMaternal Notes 1Mica Campoy CabinongNo ratings yet
- Biofertilizer Part 2Document20 pagesBiofertilizer Part 2Garima BartariyaNo ratings yet
- Second MessengersDocument42 pagesSecond MessengersYunonNo ratings yet
- 8725-300 Psa Xs Accubind Elisa Rev 0Document2 pages8725-300 Psa Xs Accubind Elisa Rev 0dr madhusudhan reddyNo ratings yet
- Pex 08 01Document4 pagesPex 08 01Rafi SalimNo ratings yet
- Transport in PlantsDocument12 pagesTransport in PlantsMEME KA GHANTANo ratings yet
- Detection of AdulterationDocument21 pagesDetection of AdulterationDR.U.Srinivasa0% (1)
- Tenebrio MolitorDocument9 pagesTenebrio Molitorじょしら フィアンナNo ratings yet
- EMBL-EBI Train OnlineDocument19 pagesEMBL-EBI Train OnlineThyagoNo ratings yet
- H3C - Abstract Book 12302014-V2Document204 pagesH3C - Abstract Book 12302014-V2AAPI ConventionNo ratings yet
- The Biological Revolution: Periodicals of Engineering and Natural Sciences Vol. 3 No. 1 (2015) Available Online atDocument2 pagesThe Biological Revolution: Periodicals of Engineering and Natural Sciences Vol. 3 No. 1 (2015) Available Online atAngel TaylorNo ratings yet
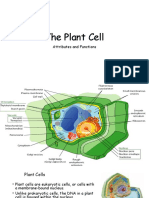
- The Plant CellDocument30 pagesThe Plant CellMichael GentilesNo ratings yet
- Management of Palm Oil PestDocument11 pagesManagement of Palm Oil PestMohamad Syu'ib SyaukatNo ratings yet
- Bio-FIT Book EN PDFDocument256 pagesBio-FIT Book EN PDFCesar Augusto Colorado RamirezNo ratings yet
- Lecture2 GranulopoiesisDocument9 pagesLecture2 GranulopoiesisAfifa Prima GittaNo ratings yet
- Questionbank EST IMPDocument12 pagesQuestionbank EST IMPSaquibh Shaikh0% (1)
- MacMillan Science Library - Animal Sciences Vol. 3 - Hab-PepDocument240 pagesMacMillan Science Library - Animal Sciences Vol. 3 - Hab-PepBLUECOMANCHE50% (2)
- EcoCRM A Recombinant CRM197 Carrier ProteinDocument1 pageEcoCRM A Recombinant CRM197 Carrier ProteinRamakrishnaNo ratings yet
- Laju Respirasi Hewan With Cover Page v2Document8 pagesLaju Respirasi Hewan With Cover Page v2Rhian AlfiansyahNo ratings yet
- The Semantics of Morphological RelationsDocument65 pagesThe Semantics of Morphological RelationsDương Bùi100% (1)
- Chronic Leukemia HerfindalDocument40 pagesChronic Leukemia HerfindalAanshi ShahNo ratings yet