
PIIS1878747923014356
PIIS1878747923014356
You might also like
- Myers, S. (2000) - Empathic Listening - Reports On The Experience of Being Heard. Journal of Humanistic Psychology, 40 (2), 148-173.Document26 pagesMyers, S. (2000) - Empathic Listening - Reports On The Experience of Being Heard. Journal of Humanistic Psychology, 40 (2), 148-173.Barbara MirasNo ratings yet
- NURS6035 Guide To Assessment 1 Written Assignment 1 Psychosocial Intervention Theory1-1Document12 pagesNURS6035 Guide To Assessment 1 Written Assignment 1 Psychosocial Intervention Theory1-1Zunaira ArshadNo ratings yet
- Working Together in Clinical SupervisionDocument28 pagesWorking Together in Clinical SupervisionCharleneKronstedt100% (1)
- Personal Counseling Theory PaperDocument9 pagesPersonal Counseling Theory PaperBecky DeatherageNo ratings yet
- EUO NRSG263 FinalDocument17 pagesEUO NRSG263 FinalJosh TuibeoNo ratings yet
- Dialectical Dilemma TherapistDocument3 pagesDialectical Dilemma TherapistRosalie Lotspeich100% (1)
- Chapter 20 - Culturally Adaptive InterviewingDocument94 pagesChapter 20 - Culturally Adaptive InterviewingNaomi LiangNo ratings yet
- Aghababa ProfessionaldevelopmentplanDocument2 pagesAghababa Professionaldevelopmentplanapi-403364756No ratings yet
- 02.therapist Experience and Style As Factors in Co-Therapy - RiceDocument7 pages02.therapist Experience and Style As Factors in Co-Therapy - RiceErnesto ContrerasNo ratings yet
- Nihms917423 PDFDocument14 pagesNihms917423 PDFnoeanisaNo ratings yet
- Testing The Reliability and Validity of The Self-Effica.. PDFDocument13 pagesTesting The Reliability and Validity of The Self-Effica.. PDFnurona azizahNo ratings yet
- The Association Between Benign Fasciculations and Health AnxietyDocument9 pagesThe Association Between Benign Fasciculations and Health AnxietyTravis ReddenNo ratings yet
- A COGNITIVE BEHAVIOURAL THEORY OF ANOREXIA NERVOSA - Fairburn, Cooper, Shafran, 1998 PDFDocument13 pagesA COGNITIVE BEHAVIOURAL THEORY OF ANOREXIA NERVOSA - Fairburn, Cooper, Shafran, 1998 PDFAnonymous yMuS0wINo ratings yet
- 2 - Grazebrook, K & Garland, A. (2005) - What Are Cognitive and - Orbehavioural Psychotherapies - Paper Prepared For UKCP - BACP PDFDocument5 pages2 - Grazebrook, K & Garland, A. (2005) - What Are Cognitive and - Orbehavioural Psychotherapies - Paper Prepared For UKCP - BACP PDFAnastasiya PlohihNo ratings yet
- ASD Document PDFDocument334 pagesASD Document PDFDiana RuicanNo ratings yet
- Abnormal Psychology Practice ExamDocument10 pagesAbnormal Psychology Practice ExamAlistair GordonNo ratings yet
- Pitman 1987 - A Cybernetic Model of OCDDocument10 pagesPitman 1987 - A Cybernetic Model of OCDAndrei PredaNo ratings yet
- Children of Mothers With Borderline Personality Disorder (BPD)Document6 pagesChildren of Mothers With Borderline Personality Disorder (BPD)curiositykillcat100% (1)
- Interpersonal Psychotherapy: Introduction and OverviewDocument22 pagesInterpersonal Psychotherapy: Introduction and OverviewRonald Bartolome100% (1)
- Yoga TherapyDocument3 pagesYoga Therapyvvk639228No ratings yet
- The History & Tranditions of Clinical SupervisionDocument64 pagesThe History & Tranditions of Clinical SupervisionMerlinkevinNo ratings yet
- A Dynamic Group For The ElderlyDocument12 pagesA Dynamic Group For The ElderlyjuaromerNo ratings yet
- Contracting For Group SupervisionDocument5 pagesContracting For Group Supervisionapi-626136134No ratings yet
- REBTDocument5 pagesREBTAlka TripathiNo ratings yet
- Coun 541 Theoretical Orientation PaperDocument9 pagesCoun 541 Theoretical Orientation Paperapi-696100484No ratings yet
- #J199694313 Therapeutic Alliance With Children and FamiliesDocument9 pages#J199694313 Therapeutic Alliance With Children and FamiliesMark SimonNo ratings yet
- Coun523 Final Paper Treatment PlanDocument11 pagesCoun523 Final Paper Treatment Planapi-717187506No ratings yet
- Castonguay+et+al+ 1996Document8 pagesCastonguay+et+al+ 1996Pamela Cortés PeñaNo ratings yet
- MUPS Manual PDFDocument72 pagesMUPS Manual PDFJacob LukaNo ratings yet
- Briefing 217 Talking TherapiesDocument6 pagesBriefing 217 Talking Therapiesmblanco15No ratings yet
- CBT: The Obscuring of Power in The Name of ScienceDocument17 pagesCBT: The Obscuring of Power in The Name of ScienceLinda StupartNo ratings yet
- Strasburger Et Al-2015-PsyCh JournalDocument8 pagesStrasburger Et Al-2015-PsyCh JournalPedro CardosoNo ratings yet
- CBT Pragmatic ApproachDocument10 pagesCBT Pragmatic ApproachMikey StanleyNo ratings yet
- The Hypothesis As Dialogue: An Interview With Paolo BertrandoDocument12 pagesThe Hypothesis As Dialogue: An Interview With Paolo BertrandoFausto Adrián Rodríguez LópezNo ratings yet
- What Is Psychotherapy - OdtDocument3 pagesWhat Is Psychotherapy - Odtsehar arif100% (1)
- Evidence of Efficacy? Margaret Williams 10 March 2008Document7 pagesEvidence of Efficacy? Margaret Williams 10 March 2008fbomxdijzyorNo ratings yet
- Part of The Team Art Therapy With Pre School Children With Developmental Delays and Disabilities in A Children S Treatment Centre SettingDocument11 pagesPart of The Team Art Therapy With Pre School Children With Developmental Delays and Disabilities in A Children S Treatment Centre SettingBusu AndreeaNo ratings yet
- CBTDocument5 pagesCBTJamela Zoe DMNo ratings yet
- Paper 2 Compassion FatigueDocument4 pagesPaper 2 Compassion Fatigueapi-401934380No ratings yet
- Anxiety ScaleDocument19 pagesAnxiety Scaleandreea gheorgheNo ratings yet
- A Baptism of Fire'. A Qualitative InvestigationDocument11 pagesA Baptism of Fire'. A Qualitative InvestigationNichifor Tanase100% (1)
- Group Proposal Final 10.2Document22 pagesGroup Proposal Final 10.2Calvin100% (1)
- Depression in Adults 58302785221Document47 pagesDepression in Adults 58302785221andreNo ratings yet
- What Me Worry 03 Negative Beliefs About Worry UncontrollabilityDocument10 pagesWhat Me Worry 03 Negative Beliefs About Worry UncontrollabilityDaniela AcevedoNo ratings yet
- Critique On Psychoanalytic Theory and Adlerian Therapy RD 011709Document4 pagesCritique On Psychoanalytic Theory and Adlerian Therapy RD 011709Lavelle100% (3)
- 2016 Resilience, Risk, Mental Health and Well-Being Associations and Conceptual DifferencesDocument9 pages2016 Resilience, Risk, Mental Health and Well-Being Associations and Conceptual DifferencesDorin CascavalNo ratings yet
- Theory Use in Counseling Practice: Current Trends: Int J Adv CounsellingDocument16 pagesTheory Use in Counseling Practice: Current Trends: Int J Adv CounsellingWastiti AdiningrumNo ratings yet
- Student Handbook 2020 OnlineDocument11 pagesStudent Handbook 2020 OnlineKidz to Adultz ExhibitionsNo ratings yet
- A Synopsis of Rational-Emotive Behavior Therapy (Rebt), David, Szentagotai, Kallay, MacaveiDocument47 pagesA Synopsis of Rational-Emotive Behavior Therapy (Rebt), David, Szentagotai, Kallay, MacaveiRildoNo ratings yet
- BehaviorismDocument13 pagesBehaviorismJoy Rioflorido AlmonteNo ratings yet
- Clinical Guidelines OverviewDocument36 pagesClinical Guidelines OverviewFatahilah MfNo ratings yet
- Child Case SampleDocument4 pagesChild Case SampleWazeerullah KhanNo ratings yet
- Adherence TheoriesDocument6 pagesAdherence TheoriesmakmgmNo ratings yet
- Role of Attitude in Multicultural Counseling - Minami (2009)Document8 pagesRole of Attitude in Multicultural Counseling - Minami (2009)xiejie22590No ratings yet
- Emdr 2002Document14 pagesEmdr 2002jivinaNo ratings yet
- Final UploadDocument24 pagesFinal Uploadapi-428157976No ratings yet
- Group Therapy PDFDocument2 pagesGroup Therapy PDFma maNo ratings yet
- Complementary TherapiesDocument8 pagesComplementary Therapiestj_sweetgirl100% (2)
- SchizophreniaDocument9 pagesSchizophreniavinodksahuNo ratings yet
- TP and PVT For Print PDFDocument15 pagesTP and PVT For Print PDFVania Aguilera ArriagadaNo ratings yet
- Group Cognitive Behavioural Therapy For Psychosis in The Asian Context: A Review of The Recent StudiesDocument28 pagesGroup Cognitive Behavioural Therapy For Psychosis in The Asian Context: A Review of The Recent StudiesIka Agitra NingrumNo ratings yet
- Khoury 2013 Mindfulness-Metaanalys PDFDocument9 pagesKhoury 2013 Mindfulness-Metaanalys PDFImanol MendizabalNo ratings yet
- Supervisors Manual Feb 15Document64 pagesSupervisors Manual Feb 15Kiesha BentleyNo ratings yet
- Annual Review of Addictions and Offender Counseling, Volume IV: Best PracticesFrom EverandAnnual Review of Addictions and Offender Counseling, Volume IV: Best PracticesNo ratings yet
- Valproate For Agitation in Critically Ill Patients - A Retrospective Study-2017Document7 pagesValproate For Agitation in Critically Ill Patients - A Retrospective Study-2017Juan ParedesNo ratings yet
- Iatrogenic Opioid Withdrawal in Critically Ill Patients - A Review of Assessment Tools and Management-2017Document13 pagesIatrogenic Opioid Withdrawal in Critically Ill Patients - A Review of Assessment Tools and Management-2017Juan Paredes100% (1)
- A Clinical Pathway To Standardize Care of Children With Delirium in Pediatric Inpatient Settings-2019Document10 pagesA Clinical Pathway To Standardize Care of Children With Delirium in Pediatric Inpatient Settings-2019Juan ParedesNo ratings yet
- The Balint Group and Its Application in Medical Education - A Systematic Review - 2019Document7 pagesThe Balint Group and Its Application in Medical Education - A Systematic Review - 2019Juan ParedesNo ratings yet
- Analgesia, Sedation, and Delirium in Pediatric Surgical Critical Care-2019Document10 pagesAnalgesia, Sedation, and Delirium in Pediatric Surgical Critical Care-2019Juan ParedesNo ratings yet
- Case 18-2017 - An 11-Year-Old Girl With Difficulty Eating After A Choking Incident-2017Document10 pagesCase 18-2017 - An 11-Year-Old Girl With Difficulty Eating After A Choking Incident-2017Juan ParedesNo ratings yet
- Pediatric Delirium - Recognition, Management, and Outcome-2017Document7 pagesPediatric Delirium - Recognition, Management, and Outcome-2017Juan ParedesNo ratings yet
- Alcohol and Other Substance Use Among Medical and Law Students at A UK University - A Cross-Sectional Questionnaire Survey-2017Document6 pagesAlcohol and Other Substance Use Among Medical and Law Students at A UK University - A Cross-Sectional Questionnaire Survey-2017Juan ParedesNo ratings yet
- Differentiation of Delirium, Dementia and Delirium Superimposed On Dementia in The Older Person-2018Document5 pagesDifferentiation of Delirium, Dementia and Delirium Superimposed On Dementia in The Older Person-2018Juan Paredes100% (1)
- Temporal Biomarker Profiles and Their Association With ICU Acquired Delirium - A Cohort Study-2018Document10 pagesTemporal Biomarker Profiles and Their Association With ICU Acquired Delirium - A Cohort Study-2018Juan ParedesNo ratings yet
- Correlations Between Brain Changes and Pain Management After Cognitive and Meditative Therapies - A Systematic Review of Neuroimaging Studies-2018Document9 pagesCorrelations Between Brain Changes and Pain Management After Cognitive and Meditative Therapies - A Systematic Review of Neuroimaging Studies-2018Juan ParedesNo ratings yet
- Efficacy of Problem Solving Therapy For Spouses of Men With Prostate Cancer - A Randomized Controlled Trial-2018Document9 pagesEfficacy of Problem Solving Therapy For Spouses of Men With Prostate Cancer - A Randomized Controlled Trial-2018Juan ParedesNo ratings yet
- Suicide Risk in Chronic Heart Failure Patients and Its Association With Depression, Hopelessness and Self Esteem-2019Document4 pagesSuicide Risk in Chronic Heart Failure Patients and Its Association With Depression, Hopelessness and Self Esteem-2019Juan ParedesNo ratings yet
- Key Updates in The Clinical Application of Electroconvulsive Therapy-2017Document10 pagesKey Updates in The Clinical Application of Electroconvulsive Therapy-2017Juan ParedesNo ratings yet
- Delirium in Elderly Patients - Prospective Prevalence Across Hospital Services-2020Document7 pagesDelirium in Elderly Patients - Prospective Prevalence Across Hospital Services-2020Juan ParedesNo ratings yet
- Consultation-Liaison Psychiatry - How Far Have We Come - 2006Document8 pagesConsultation-Liaison Psychiatry - How Far Have We Come - 2006Juan ParedesNo ratings yet
- Signed Off Personality Developent11 q1 m4 Mental Health Well Being and Emotional Intelligence in Middle and Late Adolescence v3 RemovedDocument23 pagesSigned Off Personality Developent11 q1 m4 Mental Health Well Being and Emotional Intelligence in Middle and Late Adolescence v3 RemovedkivenNo ratings yet
- Autism Boarding SchoolDocument5 pagesAutism Boarding SchoolBrian HaraNo ratings yet
- Testimonial Theatre-Making: Establishing or Dissociating The SelfDocument9 pagesTestimonial Theatre-Making: Establishing or Dissociating The SelfLucretia DespinoiuNo ratings yet
- GRADE 7 3rd Quarter TEST PAPERDocument3 pagesGRADE 7 3rd Quarter TEST PAPERBadeth AblaoNo ratings yet
- Case Study FinalDocument4 pagesCase Study Finalapi-308562224No ratings yet
- Epilepsy Fact SheetDocument1 pageEpilepsy Fact SheetAllison SylteNo ratings yet
- Cox and Barnier - Hypnotic Illusions and Clinical Delusions - Hypnosis As A Research MethodDocument32 pagesCox and Barnier - Hypnotic Illusions and Clinical Delusions - Hypnosis As A Research MethodwillyfreddyNo ratings yet
- Obsessive-Compulsive Disorder in Children and Adolescents: Georgina Krebs, Isobel HeymanDocument5 pagesObsessive-Compulsive Disorder in Children and Adolescents: Georgina Krebs, Isobel HeymanRidwan AdiansyahNo ratings yet
- Parental Overprotection ScaleDocument7 pagesParental Overprotection ScaleMartaria Rizky RinaldiNo ratings yet
- MCQsDocument95 pagesMCQsMarcus GrisomNo ratings yet
- Family Interventions For Bipolar DisorderDocument3 pagesFamily Interventions For Bipolar DisorderRanda NurawiNo ratings yet
- CaddraGuidelines2011 ToolkitDocument48 pagesCaddraGuidelines2011 ToolkitYet Barreda Basbas100% (1)
- Hemisphere SpecializationDocument7 pagesHemisphere SpecializationLisa MartinezNo ratings yet
- Talk by DR - Judy JeyakumarDocument5 pagesTalk by DR - Judy JeyakumarKalmunai Mental Health AssociationNo ratings yet
- B08LT728MSDocument501 pagesB08LT728MSSandy FireNo ratings yet
- ADHD Checklist PDFDocument1 pageADHD Checklist PDFCarlo PreciosoNo ratings yet
- Anorexia Nerviosa y Trastornos Del Espectro Autista Investigacion Guiada de Endofenotipos Cognitivos SocialesDocument31 pagesAnorexia Nerviosa y Trastornos Del Espectro Autista Investigacion Guiada de Endofenotipos Cognitivos SocialesCarito Hernandez RodriguezNo ratings yet
- Mental Health Principles and School PracticesDocument13 pagesMental Health Principles and School Practicesclara dupitasNo ratings yet
- What Is BurnoutDocument5 pagesWhat Is BurnoutJona AddatuNo ratings yet
- Name of The Course:-M.Phil, Economics: Result of Delhi University Entrance Test (DUET) - 2018Document5 pagesName of The Course:-M.Phil, Economics: Result of Delhi University Entrance Test (DUET) - 2018Saiganesh RameshNo ratings yet
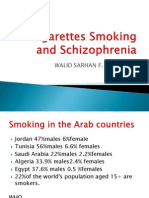
- Walid Sarhan F. R. C. PsychDocument46 pagesWalid Sarhan F. R. C. PsychFree Escort ServiceNo ratings yet
- Presentation On For Communication Studies CapeDocument21 pagesPresentation On For Communication Studies CapeConrod Wayne Smith0% (1)
- Hare Psychopathy ChecklistDocument2 pagesHare Psychopathy ChecklistDJSeidel80% (5)
- 11 Feb CYBER BULLYING CONCEPT PAPER - PPT 6Document32 pages11 Feb CYBER BULLYING CONCEPT PAPER - PPT 6DAVID WAMBUGU88% (8)
- Child Background Information FormDocument5 pagesChild Background Information FormIqbal Baryar100% (2)








































































































Download as pdf or txt
You might also like
- Myers, S. (2000) - Empathic Listening - Reports On The Experience of Being Heard. Journal of Humanistic Psychology, 40 (2), 148-173.Document26 pagesMyers, S. (2000) - Empathic Listening - Reports On The Experience of Being Heard. Journal of Humanistic Psychology, 40 (2), 148-173.Barbara MirasNo ratings yet
- NURS6035 Guide To Assessment 1 Written Assignment 1 Psychosocial Intervention Theory1-1Document12 pagesNURS6035 Guide To Assessment 1 Written Assignment 1 Psychosocial Intervention Theory1-1Zunaira ArshadNo ratings yet
- Working Together in Clinical SupervisionDocument28 pagesWorking Together in Clinical SupervisionCharleneKronstedt100% (1)
- Personal Counseling Theory PaperDocument9 pagesPersonal Counseling Theory PaperBecky DeatherageNo ratings yet
- EUO NRSG263 FinalDocument17 pagesEUO NRSG263 FinalJosh TuibeoNo ratings yet
- Dialectical Dilemma TherapistDocument3 pagesDialectical Dilemma TherapistRosalie Lotspeich100% (1)
- Chapter 20 - Culturally Adaptive InterviewingDocument94 pagesChapter 20 - Culturally Adaptive InterviewingNaomi LiangNo ratings yet
- Aghababa ProfessionaldevelopmentplanDocument2 pagesAghababa Professionaldevelopmentplanapi-403364756No ratings yet
- 02.therapist Experience and Style As Factors in Co-Therapy - RiceDocument7 pages02.therapist Experience and Style As Factors in Co-Therapy - RiceErnesto ContrerasNo ratings yet
- Nihms917423 PDFDocument14 pagesNihms917423 PDFnoeanisaNo ratings yet
- Testing The Reliability and Validity of The Self-Effica.. PDFDocument13 pagesTesting The Reliability and Validity of The Self-Effica.. PDFnurona azizahNo ratings yet
- The Association Between Benign Fasciculations and Health AnxietyDocument9 pagesThe Association Between Benign Fasciculations and Health AnxietyTravis ReddenNo ratings yet
- A COGNITIVE BEHAVIOURAL THEORY OF ANOREXIA NERVOSA - Fairburn, Cooper, Shafran, 1998 PDFDocument13 pagesA COGNITIVE BEHAVIOURAL THEORY OF ANOREXIA NERVOSA - Fairburn, Cooper, Shafran, 1998 PDFAnonymous yMuS0wINo ratings yet
- 2 - Grazebrook, K & Garland, A. (2005) - What Are Cognitive and - Orbehavioural Psychotherapies - Paper Prepared For UKCP - BACP PDFDocument5 pages2 - Grazebrook, K & Garland, A. (2005) - What Are Cognitive and - Orbehavioural Psychotherapies - Paper Prepared For UKCP - BACP PDFAnastasiya PlohihNo ratings yet
- ASD Document PDFDocument334 pagesASD Document PDFDiana RuicanNo ratings yet
- Abnormal Psychology Practice ExamDocument10 pagesAbnormal Psychology Practice ExamAlistair GordonNo ratings yet
- Pitman 1987 - A Cybernetic Model of OCDDocument10 pagesPitman 1987 - A Cybernetic Model of OCDAndrei PredaNo ratings yet
- Children of Mothers With Borderline Personality Disorder (BPD)Document6 pagesChildren of Mothers With Borderline Personality Disorder (BPD)curiositykillcat100% (1)
- Interpersonal Psychotherapy: Introduction and OverviewDocument22 pagesInterpersonal Psychotherapy: Introduction and OverviewRonald Bartolome100% (1)
- Yoga TherapyDocument3 pagesYoga Therapyvvk639228No ratings yet
- The History & Tranditions of Clinical SupervisionDocument64 pagesThe History & Tranditions of Clinical SupervisionMerlinkevinNo ratings yet
- A Dynamic Group For The ElderlyDocument12 pagesA Dynamic Group For The ElderlyjuaromerNo ratings yet
- Contracting For Group SupervisionDocument5 pagesContracting For Group Supervisionapi-626136134No ratings yet
- REBTDocument5 pagesREBTAlka TripathiNo ratings yet
- Coun 541 Theoretical Orientation PaperDocument9 pagesCoun 541 Theoretical Orientation Paperapi-696100484No ratings yet
- #J199694313 Therapeutic Alliance With Children and FamiliesDocument9 pages#J199694313 Therapeutic Alliance With Children and FamiliesMark SimonNo ratings yet
- Coun523 Final Paper Treatment PlanDocument11 pagesCoun523 Final Paper Treatment Planapi-717187506No ratings yet
- Castonguay+et+al+ 1996Document8 pagesCastonguay+et+al+ 1996Pamela Cortés PeñaNo ratings yet
- MUPS Manual PDFDocument72 pagesMUPS Manual PDFJacob LukaNo ratings yet
- Briefing 217 Talking TherapiesDocument6 pagesBriefing 217 Talking Therapiesmblanco15No ratings yet
- CBT: The Obscuring of Power in The Name of ScienceDocument17 pagesCBT: The Obscuring of Power in The Name of ScienceLinda StupartNo ratings yet
- Strasburger Et Al-2015-PsyCh JournalDocument8 pagesStrasburger Et Al-2015-PsyCh JournalPedro CardosoNo ratings yet
- CBT Pragmatic ApproachDocument10 pagesCBT Pragmatic ApproachMikey StanleyNo ratings yet
- The Hypothesis As Dialogue: An Interview With Paolo BertrandoDocument12 pagesThe Hypothesis As Dialogue: An Interview With Paolo BertrandoFausto Adrián Rodríguez LópezNo ratings yet
- What Is Psychotherapy - OdtDocument3 pagesWhat Is Psychotherapy - Odtsehar arif100% (1)
- Evidence of Efficacy? Margaret Williams 10 March 2008Document7 pagesEvidence of Efficacy? Margaret Williams 10 March 2008fbomxdijzyorNo ratings yet
- Part of The Team Art Therapy With Pre School Children With Developmental Delays and Disabilities in A Children S Treatment Centre SettingDocument11 pagesPart of The Team Art Therapy With Pre School Children With Developmental Delays and Disabilities in A Children S Treatment Centre SettingBusu AndreeaNo ratings yet
- CBTDocument5 pagesCBTJamela Zoe DMNo ratings yet
- Paper 2 Compassion FatigueDocument4 pagesPaper 2 Compassion Fatigueapi-401934380No ratings yet
- Anxiety ScaleDocument19 pagesAnxiety Scaleandreea gheorgheNo ratings yet
- A Baptism of Fire'. A Qualitative InvestigationDocument11 pagesA Baptism of Fire'. A Qualitative InvestigationNichifor Tanase100% (1)
- Group Proposal Final 10.2Document22 pagesGroup Proposal Final 10.2Calvin100% (1)
- Depression in Adults 58302785221Document47 pagesDepression in Adults 58302785221andreNo ratings yet
- What Me Worry 03 Negative Beliefs About Worry UncontrollabilityDocument10 pagesWhat Me Worry 03 Negative Beliefs About Worry UncontrollabilityDaniela AcevedoNo ratings yet
- Critique On Psychoanalytic Theory and Adlerian Therapy RD 011709Document4 pagesCritique On Psychoanalytic Theory and Adlerian Therapy RD 011709Lavelle100% (3)
- 2016 Resilience, Risk, Mental Health and Well-Being Associations and Conceptual DifferencesDocument9 pages2016 Resilience, Risk, Mental Health and Well-Being Associations and Conceptual DifferencesDorin CascavalNo ratings yet
- Theory Use in Counseling Practice: Current Trends: Int J Adv CounsellingDocument16 pagesTheory Use in Counseling Practice: Current Trends: Int J Adv CounsellingWastiti AdiningrumNo ratings yet
- Student Handbook 2020 OnlineDocument11 pagesStudent Handbook 2020 OnlineKidz to Adultz ExhibitionsNo ratings yet
- A Synopsis of Rational-Emotive Behavior Therapy (Rebt), David, Szentagotai, Kallay, MacaveiDocument47 pagesA Synopsis of Rational-Emotive Behavior Therapy (Rebt), David, Szentagotai, Kallay, MacaveiRildoNo ratings yet
- BehaviorismDocument13 pagesBehaviorismJoy Rioflorido AlmonteNo ratings yet
- Clinical Guidelines OverviewDocument36 pagesClinical Guidelines OverviewFatahilah MfNo ratings yet
- Child Case SampleDocument4 pagesChild Case SampleWazeerullah KhanNo ratings yet
- Adherence TheoriesDocument6 pagesAdherence TheoriesmakmgmNo ratings yet
- Role of Attitude in Multicultural Counseling - Minami (2009)Document8 pagesRole of Attitude in Multicultural Counseling - Minami (2009)xiejie22590No ratings yet
- Emdr 2002Document14 pagesEmdr 2002jivinaNo ratings yet
- Final UploadDocument24 pagesFinal Uploadapi-428157976No ratings yet
- Group Therapy PDFDocument2 pagesGroup Therapy PDFma maNo ratings yet
- Complementary TherapiesDocument8 pagesComplementary Therapiestj_sweetgirl100% (2)
- SchizophreniaDocument9 pagesSchizophreniavinodksahuNo ratings yet
- TP and PVT For Print PDFDocument15 pagesTP and PVT For Print PDFVania Aguilera ArriagadaNo ratings yet
- Group Cognitive Behavioural Therapy For Psychosis in The Asian Context: A Review of The Recent StudiesDocument28 pagesGroup Cognitive Behavioural Therapy For Psychosis in The Asian Context: A Review of The Recent StudiesIka Agitra NingrumNo ratings yet
- Khoury 2013 Mindfulness-Metaanalys PDFDocument9 pagesKhoury 2013 Mindfulness-Metaanalys PDFImanol MendizabalNo ratings yet
- Supervisors Manual Feb 15Document64 pagesSupervisors Manual Feb 15Kiesha BentleyNo ratings yet
- Annual Review of Addictions and Offender Counseling, Volume IV: Best PracticesFrom EverandAnnual Review of Addictions and Offender Counseling, Volume IV: Best PracticesNo ratings yet
- Valproate For Agitation in Critically Ill Patients - A Retrospective Study-2017Document7 pagesValproate For Agitation in Critically Ill Patients - A Retrospective Study-2017Juan ParedesNo ratings yet
- Iatrogenic Opioid Withdrawal in Critically Ill Patients - A Review of Assessment Tools and Management-2017Document13 pagesIatrogenic Opioid Withdrawal in Critically Ill Patients - A Review of Assessment Tools and Management-2017Juan Paredes100% (1)
- A Clinical Pathway To Standardize Care of Children With Delirium in Pediatric Inpatient Settings-2019Document10 pagesA Clinical Pathway To Standardize Care of Children With Delirium in Pediatric Inpatient Settings-2019Juan ParedesNo ratings yet
- The Balint Group and Its Application in Medical Education - A Systematic Review - 2019Document7 pagesThe Balint Group and Its Application in Medical Education - A Systematic Review - 2019Juan ParedesNo ratings yet
- Analgesia, Sedation, and Delirium in Pediatric Surgical Critical Care-2019Document10 pagesAnalgesia, Sedation, and Delirium in Pediatric Surgical Critical Care-2019Juan ParedesNo ratings yet
- Case 18-2017 - An 11-Year-Old Girl With Difficulty Eating After A Choking Incident-2017Document10 pagesCase 18-2017 - An 11-Year-Old Girl With Difficulty Eating After A Choking Incident-2017Juan ParedesNo ratings yet
- Pediatric Delirium - Recognition, Management, and Outcome-2017Document7 pagesPediatric Delirium - Recognition, Management, and Outcome-2017Juan ParedesNo ratings yet
- Alcohol and Other Substance Use Among Medical and Law Students at A UK University - A Cross-Sectional Questionnaire Survey-2017Document6 pagesAlcohol and Other Substance Use Among Medical and Law Students at A UK University - A Cross-Sectional Questionnaire Survey-2017Juan ParedesNo ratings yet
- Differentiation of Delirium, Dementia and Delirium Superimposed On Dementia in The Older Person-2018Document5 pagesDifferentiation of Delirium, Dementia and Delirium Superimposed On Dementia in The Older Person-2018Juan Paredes100% (1)
- Temporal Biomarker Profiles and Their Association With ICU Acquired Delirium - A Cohort Study-2018Document10 pagesTemporal Biomarker Profiles and Their Association With ICU Acquired Delirium - A Cohort Study-2018Juan ParedesNo ratings yet
- Correlations Between Brain Changes and Pain Management After Cognitive and Meditative Therapies - A Systematic Review of Neuroimaging Studies-2018Document9 pagesCorrelations Between Brain Changes and Pain Management After Cognitive and Meditative Therapies - A Systematic Review of Neuroimaging Studies-2018Juan ParedesNo ratings yet
- Efficacy of Problem Solving Therapy For Spouses of Men With Prostate Cancer - A Randomized Controlled Trial-2018Document9 pagesEfficacy of Problem Solving Therapy For Spouses of Men With Prostate Cancer - A Randomized Controlled Trial-2018Juan ParedesNo ratings yet
- Suicide Risk in Chronic Heart Failure Patients and Its Association With Depression, Hopelessness and Self Esteem-2019Document4 pagesSuicide Risk in Chronic Heart Failure Patients and Its Association With Depression, Hopelessness and Self Esteem-2019Juan ParedesNo ratings yet
- Key Updates in The Clinical Application of Electroconvulsive Therapy-2017Document10 pagesKey Updates in The Clinical Application of Electroconvulsive Therapy-2017Juan ParedesNo ratings yet
- Delirium in Elderly Patients - Prospective Prevalence Across Hospital Services-2020Document7 pagesDelirium in Elderly Patients - Prospective Prevalence Across Hospital Services-2020Juan ParedesNo ratings yet
- Consultation-Liaison Psychiatry - How Far Have We Come - 2006Document8 pagesConsultation-Liaison Psychiatry - How Far Have We Come - 2006Juan ParedesNo ratings yet
- Signed Off Personality Developent11 q1 m4 Mental Health Well Being and Emotional Intelligence in Middle and Late Adolescence v3 RemovedDocument23 pagesSigned Off Personality Developent11 q1 m4 Mental Health Well Being and Emotional Intelligence in Middle and Late Adolescence v3 RemovedkivenNo ratings yet
- Autism Boarding SchoolDocument5 pagesAutism Boarding SchoolBrian HaraNo ratings yet
- Testimonial Theatre-Making: Establishing or Dissociating The SelfDocument9 pagesTestimonial Theatre-Making: Establishing or Dissociating The SelfLucretia DespinoiuNo ratings yet
- GRADE 7 3rd Quarter TEST PAPERDocument3 pagesGRADE 7 3rd Quarter TEST PAPERBadeth AblaoNo ratings yet
- Case Study FinalDocument4 pagesCase Study Finalapi-308562224No ratings yet
- Epilepsy Fact SheetDocument1 pageEpilepsy Fact SheetAllison SylteNo ratings yet
- Cox and Barnier - Hypnotic Illusions and Clinical Delusions - Hypnosis As A Research MethodDocument32 pagesCox and Barnier - Hypnotic Illusions and Clinical Delusions - Hypnosis As A Research MethodwillyfreddyNo ratings yet
- Obsessive-Compulsive Disorder in Children and Adolescents: Georgina Krebs, Isobel HeymanDocument5 pagesObsessive-Compulsive Disorder in Children and Adolescents: Georgina Krebs, Isobel HeymanRidwan AdiansyahNo ratings yet
- Parental Overprotection ScaleDocument7 pagesParental Overprotection ScaleMartaria Rizky RinaldiNo ratings yet
- MCQsDocument95 pagesMCQsMarcus GrisomNo ratings yet
- Family Interventions For Bipolar DisorderDocument3 pagesFamily Interventions For Bipolar DisorderRanda NurawiNo ratings yet
- CaddraGuidelines2011 ToolkitDocument48 pagesCaddraGuidelines2011 ToolkitYet Barreda Basbas100% (1)
- Hemisphere SpecializationDocument7 pagesHemisphere SpecializationLisa MartinezNo ratings yet
- Talk by DR - Judy JeyakumarDocument5 pagesTalk by DR - Judy JeyakumarKalmunai Mental Health AssociationNo ratings yet
- B08LT728MSDocument501 pagesB08LT728MSSandy FireNo ratings yet
- ADHD Checklist PDFDocument1 pageADHD Checklist PDFCarlo PreciosoNo ratings yet
- Anorexia Nerviosa y Trastornos Del Espectro Autista Investigacion Guiada de Endofenotipos Cognitivos SocialesDocument31 pagesAnorexia Nerviosa y Trastornos Del Espectro Autista Investigacion Guiada de Endofenotipos Cognitivos SocialesCarito Hernandez RodriguezNo ratings yet
- Mental Health Principles and School PracticesDocument13 pagesMental Health Principles and School Practicesclara dupitasNo ratings yet
- What Is BurnoutDocument5 pagesWhat Is BurnoutJona AddatuNo ratings yet
- Name of The Course:-M.Phil, Economics: Result of Delhi University Entrance Test (DUET) - 2018Document5 pagesName of The Course:-M.Phil, Economics: Result of Delhi University Entrance Test (DUET) - 2018Saiganesh RameshNo ratings yet
- Walid Sarhan F. R. C. PsychDocument46 pagesWalid Sarhan F. R. C. PsychFree Escort ServiceNo ratings yet
- Presentation On For Communication Studies CapeDocument21 pagesPresentation On For Communication Studies CapeConrod Wayne Smith0% (1)
- Hare Psychopathy ChecklistDocument2 pagesHare Psychopathy ChecklistDJSeidel80% (5)
- 11 Feb CYBER BULLYING CONCEPT PAPER - PPT 6Document32 pages11 Feb CYBER BULLYING CONCEPT PAPER - PPT 6DAVID WAMBUGU88% (8)
- Child Background Information FormDocument5 pagesChild Background Information FormIqbal Baryar100% (2)