
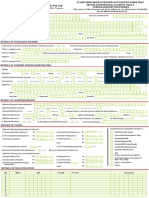
claim form B
claim form B
You might also like
- Motions, Affidavits, Answers, and Commercial Liens - The Book of Effective Sample DocumentsFrom EverandMotions, Affidavits, Answers, and Commercial Liens - The Book of Effective Sample DocumentsRating: 4.5 out of 5 stars4.5/5 (14)
- Medical Billing Training ManualDocument51 pagesMedical Billing Training ManualRadha Raman Sharma100% (1)
- V11.5 (EXE) Release NotesDocument393 pagesV11.5 (EXE) Release NotesB PNo ratings yet
- NHIF Universal Claim Form 2020Document2 pagesNHIF Universal Claim Form 2020joyce akoth74% (34)
- Esv Icd11Document60 pagesEsv Icd11Mohammed Muhidin75% (4)
- Part B - Aditya BirlaDocument4 pagesPart B - Aditya BirlaRainbow Multispeciality HospitalNo ratings yet
- Aditya Birla Health Insurance Co. LimitedDocument4 pagesAditya Birla Health Insurance Co. LimitedAdeep MathurNo ratings yet
- Health Claim Form Part BDocument3 pagesHealth Claim Form Part BShubham PandeyNo ratings yet
- ProHealth V7 ClaimFormB 23oct30Document5 pagesProHealth V7 ClaimFormB 23oct30shailendra.goswamiNo ratings yet
- Reimbursement Claim Form Part BDocument2 pagesReimbursement Claim Form Part BShishir AgrawalNo ratings yet
- ReimbursementFormA B2016Document7 pagesReimbursementFormA B2016DESIGN CGMPNo ratings yet
- Reliance Claim Form BDocument2 pagesReliance Claim Form BAbhay HarkanchiNo ratings yet
- Easy Ways To Speed Up The Claims Process: Manipalcigna Health Insurance Company Ltd. Claim Form - Part BDocument5 pagesEasy Ways To Speed Up The Claims Process: Manipalcigna Health Insurance Company Ltd. Claim Form - Part BRamesh WalkeNo ratings yet
- Claim Form PartBDocument1 pageClaim Form PartBsamarth agarwalNo ratings yet
- Claims FormDocument16 pagesClaims FormPhunsukh WangduNo ratings yet
- Heartbeat Claim Form PDFDocument16 pagesHeartbeat Claim Form PDFAnkitThakkarNo ratings yet
- Heartbeat Claim FormDocument8 pagesHeartbeat Claim Formto.animeshsen604No ratings yet
- Claim Form PartBDocument2 pagesClaim Form PartBbelly4uNo ratings yet
- HDFC ERGO General Insurance Company LimitedDocument6 pagesHDFC ERGO General Insurance Company LimitedShibani DesaiNo ratings yet
- Max Bupa Claims FormDocument16 pagesMax Bupa Claims FormraviNo ratings yet
- Claim Form - Part B: To Be Filled in by The HospitalDocument2 pagesClaim Form - Part B: To Be Filled in by The HospitalAli ArsalaanNo ratings yet
- Uiic Claim Form HospitalDocument2 pagesUiic Claim Form HospitalJagdish GehlothNo ratings yet
- NIC CLAIM FORM Hospital PDFDocument2 pagesNIC CLAIM FORM Hospital PDFAnikendu MaitraNo ratings yet
- Aditya Birla Claim Form Part ADocument8 pagesAditya Birla Claim Form Part Astatus addaNo ratings yet
- Claim Form Part ADocument4 pagesClaim Form Part Ajeparal482No ratings yet
- E Claim FormDocument8 pagesE Claim FormronNo ratings yet
- Cashless FormDocument2 pagesCashless FormHitendra PatelNo ratings yet
- CashlessDocument2 pagesCashlessJames ultraNo ratings yet
- Request For Cashless Hospitalisation For Health Insurance Policy PART C (Revised)Document4 pagesRequest For Cashless Hospitalisation For Health Insurance Policy PART C (Revised)Abhishek MkNo ratings yet
- Cashless Claim FormDocument2 pagesCashless Claim FormSavinNo ratings yet
- HDFC Group Health Insurance - Claim ManualDocument6 pagesHDFC Group Health Insurance - Claim ManualNeir KrNo ratings yet
- Claim Form - HospitalizationDocument8 pagesClaim Form - HospitalizationNishantShah100% (1)
- Reimbursement A PDFDocument4 pagesReimbursement A PDFAniruddha ShivalNo ratings yet
- Details of Primary Insured: Bajaj Allianz General Insurance Company LimitedDocument3 pagesDetails of Primary Insured: Bajaj Allianz General Insurance Company LimitedBellapu Durga vara prasadNo ratings yet
- IRDA - Claim Form-4Document1 pageIRDA - Claim Form-4Sunny bNo ratings yet
- Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part ADocument7 pagesClaim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part Aharmeet singhNo ratings yet
- Care Claimform PDFDocument2 pagesCare Claimform PDFHitendra PatelNo ratings yet
- Vipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistoryDocument7 pagesVipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistoryChatterjee KushalNo ratings yet
- Reimbursement Claim FormDocument7 pagesReimbursement Claim FormashishladooNo ratings yet
- Claim FormDocument3 pagesClaim FormVediappan Alies RajaNo ratings yet
- Health File3Document9 pagesHealth File3kulbirplusNo ratings yet
- ReimbursementFormA B2016 PDFDocument5 pagesReimbursementFormA B2016 PDFranganathNo ratings yet
- Vipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistoryDocument7 pagesVipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistorySwapnil NageNo ratings yet
- Claim Form - Part A General InsuranceDocument3 pagesClaim Form - Part A General Insurancejignesh vyasNo ratings yet
- Health Assurance Claim FormDocument8 pagesHealth Assurance Claim FormHarmeet MaanNo ratings yet
- Health Insurance Claim FormDocument4 pagesHealth Insurance Claim Formaditya TestNo ratings yet
- Claim Form PDFDocument5 pagesClaim Form PDFmeghaNo ratings yet
- Bajaj Claim FormDocument9 pagesBajaj Claim FormYogi’s iphone No ratings yet
- Claim Form 10 - EditableDocument9 pagesClaim Form 10 - EditableharshiNo ratings yet
- Reimbursement Claim FormDocument4 pagesReimbursement Claim FormhariharanccetNo ratings yet
- IRDAPre Auth FormDocument2 pagesIRDAPre Auth FormAnirban DasguptaNo ratings yet
- VMPL - Claim Form (A)Document3 pagesVMPL - Claim Form (A)Rahul RathodNo ratings yet
- Standard Claim Form HospitalDocument2 pagesStandard Claim Form Hospitalnpatel35No ratings yet
- Claim FormDocument6 pagesClaim Formashu9649No ratings yet
- Vipul Corp TPA PVT LTD.: Details of Insurance HistoryDocument6 pagesVipul Corp TPA PVT LTD.: Details of Insurance HistorybrajendraNo ratings yet
- Vipul Pre - AuthDocument4 pagesVipul Pre - AuthDr SJS RandhawaNo ratings yet
- Claim Form - Part A: To Be Filled in by The InsuredDocument2 pagesClaim Form - Part A: To Be Filled in by The InsuredAli ArsalaanNo ratings yet
- New Claim Form Dhs ReimbursementDocument4 pagesNew Claim Form Dhs Reimbursementamit_bisht2225% (4)
- Claim Reimbursement FormDocument7 pagesClaim Reimbursement FormBagavathi RNo ratings yet
- Easy Ways To Speed Up The Claims Process: Manipalcigna Prohealth Insurance Policy Claim Form ADocument6 pagesEasy Ways To Speed Up The Claims Process: Manipalcigna Prohealth Insurance Policy Claim Form ARamesh WalkeNo ratings yet
- Passing the Uniform Bar Exam: Outlines and Cases to Help You Pass the Bar in New York and Twenty-Three Other States: Professional Examination Success Guides, #1From EverandPassing the Uniform Bar Exam: Outlines and Cases to Help You Pass the Bar in New York and Twenty-Three Other States: Professional Examination Success Guides, #1Rating: 2.5 out of 5 stars2.5/5 (3)
- Iran-United States Claims Arbitration: Debates on Commercial and Public International LawFrom EverandIran-United States Claims Arbitration: Debates on Commercial and Public International LawNo ratings yet
- FPQP Practice Question Workbook: 1,000 Comprehensive Practice Questions (2024 Edition)From EverandFPQP Practice Question Workbook: 1,000 Comprehensive Practice Questions (2024 Edition)No ratings yet
- PRERNA INDUSTRIES - QUOTATIONDocument1 pagePRERNA INDUSTRIES - QUOTATIONManoj VasoyaNo ratings yet
- UniqueDocument2 pagesUniqueManoj VasoyaNo ratings yet
- Subsidy DocumentsDocument1 pageSubsidy DocumentsManoj VasoyaNo ratings yet
- IgnotDocument28 pagesIgnotManoj VasoyaNo ratings yet
- BilletDocument17 pagesBilletManoj VasoyaNo ratings yet
- Tma 1 Prep & Block 1 Intro SlidesDocument64 pagesTma 1 Prep & Block 1 Intro SlidesashleygvieiraNo ratings yet
- Mdscan - An Explainable Artificial Intelligence Artifact For MentaDocument13 pagesMdscan - An Explainable Artificial Intelligence Artifact For Mentahegde247No ratings yet
- Kaiser Permanente DOJ ComplaintDocument96 pagesKaiser Permanente DOJ ComplaintKevin TruongNo ratings yet
- A Guide For Bachelor of Science (Nursing) Licensing ExaminationDocument185 pagesA Guide For Bachelor of Science (Nursing) Licensing ExaminationEVERYTHING TvNo ratings yet
- Nys Medicaid Pre-Adjudication Crosswalk For Health Care ClaimsDocument4 pagesNys Medicaid Pre-Adjudication Crosswalk For Health Care ClaimsTeresaNo ratings yet
- Transmission of Mental Disorders in Adolescent Peer NetworksDocument7 pagesTransmission of Mental Disorders in Adolescent Peer NetworksstrillenNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance PolicypawanNo ratings yet
- Medical Coding Resume ExamplesDocument6 pagesMedical Coding Resume Examplesfsjqj9qh100% (1)
- Larsen, J.K. (2017)Document8 pagesLarsen, J.K. (2017)Ale ValenciaNo ratings yet
- Medicash Claim FormDocument6 pagesMedicash Claim Formwaran RMNo ratings yet
- TMD 1Document75 pagesTMD 1pianistgirl99No ratings yet
- Trends in US Emergency Department Visits For Mental Health, Overdose, and Violence Outcomes Before and During The COVID-19 Pandemic (2021)Document8 pagesTrends in US Emergency Department Visits For Mental Health, Overdose, and Violence Outcomes Before and During The COVID-19 Pandemic (2021)Kenmaster WirelessNo ratings yet
- Underlying Medical Conditions and Severe Illness Among 540,667 Adults Hospitalized With COVID-19, March 2020-March 2021Document12 pagesUnderlying Medical Conditions and Severe Illness Among 540,667 Adults Hospitalized With COVID-19, March 2020-March 2021Michael DriscollNo ratings yet
- Dody Firmanda 2020 - Displin Profesi Kedokteran (Dari Hulu Ke Hilir - Pendidikan, Layanan, Penelitian & Pengabdian)Document153 pagesDody Firmanda 2020 - Displin Profesi Kedokteran (Dari Hulu Ke Hilir - Pendidikan, Layanan, Penelitian & Pengabdian)Dody FirmandaNo ratings yet
- MS PsychologyDocument48 pagesMS PsychologyAimen MurtazaNo ratings yet
- Medical Office Manager Resume SamplesDocument8 pagesMedical Office Manager Resume Samplesxdkankjbf100% (2)
- Impact of Type 1 Versus Type 2 Diabetes On Developing Herpes Zoster and Post-Herpetic Neuralgia: A Population-Based Cohort StudyDocument6 pagesImpact of Type 1 Versus Type 2 Diabetes On Developing Herpes Zoster and Post-Herpetic Neuralgia: A Population-Based Cohort StudyStella SulartoNo ratings yet
- Mental Health Literature ReviewDocument5 pagesMental Health Literature Reviewfat1kifywel3100% (1)
- Prevalence of Chronic Health ConditionsDocument27 pagesPrevalence of Chronic Health ConditionsЯковлев АлександрNo ratings yet
- Professional Psychology: Research and PracticeDocument14 pagesProfessional Psychology: Research and PracticeRodica FloreaNo ratings yet
- NPMP Parivar Claim FormDocument6 pagesNPMP Parivar Claim FormArun Prabhakaran PNo ratings yet
- Contemporary Issues in Yin Yang TheoryDocument109 pagesContemporary Issues in Yin Yang TheoryRudolph Antony ThomasNo ratings yet
- Medical Records, Insurance, and ContractsDocument24 pagesMedical Records, Insurance, and ContractsBernard Kwaku OkaiNo ratings yet
- Imperial Collage of Medical and Helth SciencesDocument21 pagesImperial Collage of Medical and Helth SciencesbonfaceNo ratings yet
- Topic: Major Depression: Symptoms and SignsDocument16 pagesTopic: Major Depression: Symptoms and SignsnaviNo ratings yet
- FY10 ICD-9-CM Procedure Codes Linked To NHSN Operative Procedure CategoriesDocument22 pagesFY10 ICD-9-CM Procedure Codes Linked To NHSN Operative Procedure CategoriesYohan Julian Mega NandaNo ratings yet





























































































Download as pdf or txt
You might also like
- Motions, Affidavits, Answers, and Commercial Liens - The Book of Effective Sample DocumentsFrom EverandMotions, Affidavits, Answers, and Commercial Liens - The Book of Effective Sample DocumentsRating: 4.5 out of 5 stars4.5/5 (14)
- Medical Billing Training ManualDocument51 pagesMedical Billing Training ManualRadha Raman Sharma100% (1)
- V11.5 (EXE) Release NotesDocument393 pagesV11.5 (EXE) Release NotesB PNo ratings yet
- NHIF Universal Claim Form 2020Document2 pagesNHIF Universal Claim Form 2020joyce akoth74% (34)
- Esv Icd11Document60 pagesEsv Icd11Mohammed Muhidin75% (4)
- Part B - Aditya BirlaDocument4 pagesPart B - Aditya BirlaRainbow Multispeciality HospitalNo ratings yet
- Aditya Birla Health Insurance Co. LimitedDocument4 pagesAditya Birla Health Insurance Co. LimitedAdeep MathurNo ratings yet
- Health Claim Form Part BDocument3 pagesHealth Claim Form Part BShubham PandeyNo ratings yet
- ProHealth V7 ClaimFormB 23oct30Document5 pagesProHealth V7 ClaimFormB 23oct30shailendra.goswamiNo ratings yet
- Reimbursement Claim Form Part BDocument2 pagesReimbursement Claim Form Part BShishir AgrawalNo ratings yet
- ReimbursementFormA B2016Document7 pagesReimbursementFormA B2016DESIGN CGMPNo ratings yet
- Reliance Claim Form BDocument2 pagesReliance Claim Form BAbhay HarkanchiNo ratings yet
- Easy Ways To Speed Up The Claims Process: Manipalcigna Health Insurance Company Ltd. Claim Form - Part BDocument5 pagesEasy Ways To Speed Up The Claims Process: Manipalcigna Health Insurance Company Ltd. Claim Form - Part BRamesh WalkeNo ratings yet
- Claim Form PartBDocument1 pageClaim Form PartBsamarth agarwalNo ratings yet
- Claims FormDocument16 pagesClaims FormPhunsukh WangduNo ratings yet
- Heartbeat Claim Form PDFDocument16 pagesHeartbeat Claim Form PDFAnkitThakkarNo ratings yet
- Heartbeat Claim FormDocument8 pagesHeartbeat Claim Formto.animeshsen604No ratings yet
- Claim Form PartBDocument2 pagesClaim Form PartBbelly4uNo ratings yet
- HDFC ERGO General Insurance Company LimitedDocument6 pagesHDFC ERGO General Insurance Company LimitedShibani DesaiNo ratings yet
- Max Bupa Claims FormDocument16 pagesMax Bupa Claims FormraviNo ratings yet
- Claim Form - Part B: To Be Filled in by The HospitalDocument2 pagesClaim Form - Part B: To Be Filled in by The HospitalAli ArsalaanNo ratings yet
- Uiic Claim Form HospitalDocument2 pagesUiic Claim Form HospitalJagdish GehlothNo ratings yet
- NIC CLAIM FORM Hospital PDFDocument2 pagesNIC CLAIM FORM Hospital PDFAnikendu MaitraNo ratings yet
- Aditya Birla Claim Form Part ADocument8 pagesAditya Birla Claim Form Part Astatus addaNo ratings yet
- Claim Form Part ADocument4 pagesClaim Form Part Ajeparal482No ratings yet
- E Claim FormDocument8 pagesE Claim FormronNo ratings yet
- Cashless FormDocument2 pagesCashless FormHitendra PatelNo ratings yet
- CashlessDocument2 pagesCashlessJames ultraNo ratings yet
- Request For Cashless Hospitalisation For Health Insurance Policy PART C (Revised)Document4 pagesRequest For Cashless Hospitalisation For Health Insurance Policy PART C (Revised)Abhishek MkNo ratings yet
- Cashless Claim FormDocument2 pagesCashless Claim FormSavinNo ratings yet
- HDFC Group Health Insurance - Claim ManualDocument6 pagesHDFC Group Health Insurance - Claim ManualNeir KrNo ratings yet
- Claim Form - HospitalizationDocument8 pagesClaim Form - HospitalizationNishantShah100% (1)
- Reimbursement A PDFDocument4 pagesReimbursement A PDFAniruddha ShivalNo ratings yet
- Details of Primary Insured: Bajaj Allianz General Insurance Company LimitedDocument3 pagesDetails of Primary Insured: Bajaj Allianz General Insurance Company LimitedBellapu Durga vara prasadNo ratings yet
- IRDA - Claim Form-4Document1 pageIRDA - Claim Form-4Sunny bNo ratings yet
- Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part ADocument7 pagesClaim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part Aharmeet singhNo ratings yet
- Care Claimform PDFDocument2 pagesCare Claimform PDFHitendra PatelNo ratings yet
- Vipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistoryDocument7 pagesVipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistoryChatterjee KushalNo ratings yet
- Reimbursement Claim FormDocument7 pagesReimbursement Claim FormashishladooNo ratings yet
- Claim FormDocument3 pagesClaim FormVediappan Alies RajaNo ratings yet
- Health File3Document9 pagesHealth File3kulbirplusNo ratings yet
- ReimbursementFormA B2016 PDFDocument5 pagesReimbursementFormA B2016 PDFranganathNo ratings yet
- Vipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistoryDocument7 pagesVipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistorySwapnil NageNo ratings yet
- Claim Form - Part A General InsuranceDocument3 pagesClaim Form - Part A General Insurancejignesh vyasNo ratings yet
- Health Assurance Claim FormDocument8 pagesHealth Assurance Claim FormHarmeet MaanNo ratings yet
- Health Insurance Claim FormDocument4 pagesHealth Insurance Claim Formaditya TestNo ratings yet
- Claim Form PDFDocument5 pagesClaim Form PDFmeghaNo ratings yet
- Bajaj Claim FormDocument9 pagesBajaj Claim FormYogi’s iphone No ratings yet
- Claim Form 10 - EditableDocument9 pagesClaim Form 10 - EditableharshiNo ratings yet
- Reimbursement Claim FormDocument4 pagesReimbursement Claim FormhariharanccetNo ratings yet
- IRDAPre Auth FormDocument2 pagesIRDAPre Auth FormAnirban DasguptaNo ratings yet
- VMPL - Claim Form (A)Document3 pagesVMPL - Claim Form (A)Rahul RathodNo ratings yet
- Standard Claim Form HospitalDocument2 pagesStandard Claim Form Hospitalnpatel35No ratings yet
- Claim FormDocument6 pagesClaim Formashu9649No ratings yet
- Vipul Corp TPA PVT LTD.: Details of Insurance HistoryDocument6 pagesVipul Corp TPA PVT LTD.: Details of Insurance HistorybrajendraNo ratings yet
- Vipul Pre - AuthDocument4 pagesVipul Pre - AuthDr SJS RandhawaNo ratings yet
- Claim Form - Part A: To Be Filled in by The InsuredDocument2 pagesClaim Form - Part A: To Be Filled in by The InsuredAli ArsalaanNo ratings yet
- New Claim Form Dhs ReimbursementDocument4 pagesNew Claim Form Dhs Reimbursementamit_bisht2225% (4)
- Claim Reimbursement FormDocument7 pagesClaim Reimbursement FormBagavathi RNo ratings yet
- Easy Ways To Speed Up The Claims Process: Manipalcigna Prohealth Insurance Policy Claim Form ADocument6 pagesEasy Ways To Speed Up The Claims Process: Manipalcigna Prohealth Insurance Policy Claim Form ARamesh WalkeNo ratings yet
- Passing the Uniform Bar Exam: Outlines and Cases to Help You Pass the Bar in New York and Twenty-Three Other States: Professional Examination Success Guides, #1From EverandPassing the Uniform Bar Exam: Outlines and Cases to Help You Pass the Bar in New York and Twenty-Three Other States: Professional Examination Success Guides, #1Rating: 2.5 out of 5 stars2.5/5 (3)
- Iran-United States Claims Arbitration: Debates on Commercial and Public International LawFrom EverandIran-United States Claims Arbitration: Debates on Commercial and Public International LawNo ratings yet
- FPQP Practice Question Workbook: 1,000 Comprehensive Practice Questions (2024 Edition)From EverandFPQP Practice Question Workbook: 1,000 Comprehensive Practice Questions (2024 Edition)No ratings yet
- PRERNA INDUSTRIES - QUOTATIONDocument1 pagePRERNA INDUSTRIES - QUOTATIONManoj VasoyaNo ratings yet
- UniqueDocument2 pagesUniqueManoj VasoyaNo ratings yet
- Subsidy DocumentsDocument1 pageSubsidy DocumentsManoj VasoyaNo ratings yet
- IgnotDocument28 pagesIgnotManoj VasoyaNo ratings yet
- BilletDocument17 pagesBilletManoj VasoyaNo ratings yet
- Tma 1 Prep & Block 1 Intro SlidesDocument64 pagesTma 1 Prep & Block 1 Intro SlidesashleygvieiraNo ratings yet
- Mdscan - An Explainable Artificial Intelligence Artifact For MentaDocument13 pagesMdscan - An Explainable Artificial Intelligence Artifact For Mentahegde247No ratings yet
- Kaiser Permanente DOJ ComplaintDocument96 pagesKaiser Permanente DOJ ComplaintKevin TruongNo ratings yet
- A Guide For Bachelor of Science (Nursing) Licensing ExaminationDocument185 pagesA Guide For Bachelor of Science (Nursing) Licensing ExaminationEVERYTHING TvNo ratings yet
- Nys Medicaid Pre-Adjudication Crosswalk For Health Care ClaimsDocument4 pagesNys Medicaid Pre-Adjudication Crosswalk For Health Care ClaimsTeresaNo ratings yet
- Transmission of Mental Disorders in Adolescent Peer NetworksDocument7 pagesTransmission of Mental Disorders in Adolescent Peer NetworksstrillenNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance PolicypawanNo ratings yet
- Medical Coding Resume ExamplesDocument6 pagesMedical Coding Resume Examplesfsjqj9qh100% (1)
- Larsen, J.K. (2017)Document8 pagesLarsen, J.K. (2017)Ale ValenciaNo ratings yet
- Medicash Claim FormDocument6 pagesMedicash Claim Formwaran RMNo ratings yet
- TMD 1Document75 pagesTMD 1pianistgirl99No ratings yet
- Trends in US Emergency Department Visits For Mental Health, Overdose, and Violence Outcomes Before and During The COVID-19 Pandemic (2021)Document8 pagesTrends in US Emergency Department Visits For Mental Health, Overdose, and Violence Outcomes Before and During The COVID-19 Pandemic (2021)Kenmaster WirelessNo ratings yet
- Underlying Medical Conditions and Severe Illness Among 540,667 Adults Hospitalized With COVID-19, March 2020-March 2021Document12 pagesUnderlying Medical Conditions and Severe Illness Among 540,667 Adults Hospitalized With COVID-19, March 2020-March 2021Michael DriscollNo ratings yet
- Dody Firmanda 2020 - Displin Profesi Kedokteran (Dari Hulu Ke Hilir - Pendidikan, Layanan, Penelitian & Pengabdian)Document153 pagesDody Firmanda 2020 - Displin Profesi Kedokteran (Dari Hulu Ke Hilir - Pendidikan, Layanan, Penelitian & Pengabdian)Dody FirmandaNo ratings yet
- MS PsychologyDocument48 pagesMS PsychologyAimen MurtazaNo ratings yet
- Medical Office Manager Resume SamplesDocument8 pagesMedical Office Manager Resume Samplesxdkankjbf100% (2)
- Impact of Type 1 Versus Type 2 Diabetes On Developing Herpes Zoster and Post-Herpetic Neuralgia: A Population-Based Cohort StudyDocument6 pagesImpact of Type 1 Versus Type 2 Diabetes On Developing Herpes Zoster and Post-Herpetic Neuralgia: A Population-Based Cohort StudyStella SulartoNo ratings yet
- Mental Health Literature ReviewDocument5 pagesMental Health Literature Reviewfat1kifywel3100% (1)
- Prevalence of Chronic Health ConditionsDocument27 pagesPrevalence of Chronic Health ConditionsЯковлев АлександрNo ratings yet
- Professional Psychology: Research and PracticeDocument14 pagesProfessional Psychology: Research and PracticeRodica FloreaNo ratings yet
- NPMP Parivar Claim FormDocument6 pagesNPMP Parivar Claim FormArun Prabhakaran PNo ratings yet
- Contemporary Issues in Yin Yang TheoryDocument109 pagesContemporary Issues in Yin Yang TheoryRudolph Antony ThomasNo ratings yet
- Medical Records, Insurance, and ContractsDocument24 pagesMedical Records, Insurance, and ContractsBernard Kwaku OkaiNo ratings yet
- Imperial Collage of Medical and Helth SciencesDocument21 pagesImperial Collage of Medical and Helth SciencesbonfaceNo ratings yet
- Topic: Major Depression: Symptoms and SignsDocument16 pagesTopic: Major Depression: Symptoms and SignsnaviNo ratings yet
- FY10 ICD-9-CM Procedure Codes Linked To NHSN Operative Procedure CategoriesDocument22 pagesFY10 ICD-9-CM Procedure Codes Linked To NHSN Operative Procedure CategoriesYohan Julian Mega NandaNo ratings yet