
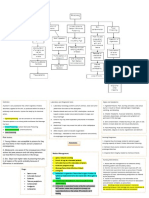
Corrosives (2)
Corrosives (2)
You might also like
- MEDICAL - SURGICAL by John RicafortDocument9 pagesMEDICAL - SURGICAL by John RicafortTazneem Apostol Esmael100% (2)
- Top 200 Sorted by Drug ClassDocument3 pagesTop 200 Sorted by Drug Classthompjo2394100% (7)
- The Cure For HIV and AIDS by Hulda Regehr ClarkDocument612 pagesThe Cure For HIV and AIDS by Hulda Regehr ClarkRobert Glen Murrell Jr100% (3)
- Medical Surgical Nursing With MnemonicsDocument111 pagesMedical Surgical Nursing With MnemonicsChernobyle Tolentino BattadNo ratings yet
- Care Health ProposalDocument12 pagesCare Health ProposalNaldre Phamhinthuan100% (1)
- Arsenic: What Is Arsenicosis ?Document24 pagesArsenic: What Is Arsenicosis ?Wasi OsmanNo ratings yet
- Midterms RLEDocument11 pagesMidterms RLEgungonfiona28No ratings yet
- COPD , RLD , SLD3Document16 pagesCOPD , RLD , SLD342n8whjhrmNo ratings yet
- Vomiting of Gastrointestinal OriginDocument4 pagesVomiting of Gastrointestinal OriginFathimathNo ratings yet
- Organophosphorus PoisoningDocument15 pagesOrganophosphorus PoisoningtaufiAmaneeNo ratings yet
- Paraquot - Organophosphate Poisoning - Short NoteDocument2 pagesParaquot - Organophosphate Poisoning - Short NoteLahiru UpendraNo ratings yet
- Organic AcidsDocument3 pagesOrganic Acidsapi-26123997No ratings yet
- AlkaloidsDocument10 pagesAlkaloidsrazan assadNo ratings yet
- Poisoning & EnvenomationDocument19 pagesPoisoning & EnvenomationVirendra K. GajbhiyeNo ratings yet
- Vih MT#2Document8 pagesVih MT#2cjNo ratings yet
- Phctlec - Topic 3&4 - PrelimsDocument24 pagesPhctlec - Topic 3&4 - PrelimsasdfdjfeonaNo ratings yet
- MS MidtermDocument3 pagesMS MidtermDaphney Ruth LeocadioNo ratings yet
- PneumoniaDocument2 pagesPneumoniama7moud farsNo ratings yet
- 2.drugs Acting On The EyeDocument19 pages2.drugs Acting On The EyeEman MohamedNo ratings yet
- Kerosene PoisonDocument3 pagesKerosene PoisonAfnan ShaikhNo ratings yet
- Pleural Conditions Arf Ards PeDocument4 pagesPleural Conditions Arf Ards PeNoreen PadillaNo ratings yet
- Cardiac Poison: DR Bibek Raj ParajuliDocument23 pagesCardiac Poison: DR Bibek Raj Parajuliranjithreddy916gmailNo ratings yet
- DependenceDocument2 pagesDependenceObaid EllafyNo ratings yet
- Pedia - Intensive PhaseDocument2 pagesPedia - Intensive Phasepasabay270No ratings yet
- ABG NotesDocument2 pagesABG NotesIsland RaeNo ratings yet
- Chapter 14 - General Emergencies and Major TraumaDocument28 pagesChapter 14 - General Emergencies and Major Traumasnowlover boyNo ratings yet
- Handout 5 CardioVascular System Overview (Recovered)Document7 pagesHandout 5 CardioVascular System Overview (Recovered)Orlyn Joy TanaweNo ratings yet
- High Ent YielDocument15 pagesHigh Ent YielJana AldourNo ratings yet
- Indicator HCO:H CO Ratio Cause / Direction Etiology ConditionsDocument1 pageIndicator HCO:H CO Ratio Cause / Direction Etiology ConditionsSalve Rachelle BillenaNo ratings yet
- Compilation of Ms NotesDocument49 pagesCompilation of Ms Noteschoyaks100% (1)
- Cardiovascular Disease NCPDocument6 pagesCardiovascular Disease NCPsprrwgoldenNo ratings yet
- Ammonia Manganese: AstrocytesDocument2 pagesAmmonia Manganese: AstrocytesJULIUS ART VINCENT A. PADINITNo ratings yet
- NCM 116 - Neurologic Disorders (MODULE 1)Document6 pagesNCM 116 - Neurologic Disorders (MODULE 1)Meryville JacildoNo ratings yet
- Oral RevalidaDocument14 pagesOral RevalidaAyaBasilioNo ratings yet
- OXYGINATION FUNDA LEC BebeDocument8 pagesOXYGINATION FUNDA LEC BebediarosedoloresbsncNo ratings yet
- PoisoningDocument2 pagesPoisoninggoyaNo ratings yet
- Cinchona - Quinin PoisoningDocument7 pagesCinchona - Quinin PoisoninghariniNo ratings yet
- Oxygen, Nutri, ElimDocument74 pagesOxygen, Nutri, ElimNina Anne ParacadNo ratings yet
- Inhalation Injury and Systemic IntoxicationDocument7 pagesInhalation Injury and Systemic IntoxicationDaniel LesmanaNo ratings yet
- Scleroderma (Harrison's Principle of Internal Medicine)Document3 pagesScleroderma (Harrison's Principle of Internal Medicine)Pia Therese NatividadNo ratings yet
- Local AnestheticsgfhgjhkjlkDocument3 pagesLocal AnestheticsgfhgjhkjlkMuhammed BarznjiNo ratings yet
- General Examination (COMPLEXION) by Dr. Rana Moustafa AlsayedDocument18 pagesGeneral Examination (COMPLEXION) by Dr. Rana Moustafa AlsayedAbdulla1999 AshrafNo ratings yet
- Hypoxia: Lori HolmesDocument5 pagesHypoxia: Lori HolmesDanson Githinji ENo ratings yet
- Thyroid Gland OSCE ExaminationDocument13 pagesThyroid Gland OSCE ExaminationkylieverNo ratings yet
- Phctlec - Topic 3 - PrelimsDocument10 pagesPhctlec - Topic 3 - PrelimsasdfdjfeonaNo ratings yet
- Copd - Midterm NotesDocument2 pagesCopd - Midterm NotesInday BertaNo ratings yet
- Diabetes MellitusDocument3 pagesDiabetes MellitusShan NaseoulNo ratings yet
- Drug StudyDocument7 pagesDrug StudyAlliah OrdanNo ratings yet
- PBL 2 GBMS 3 YR1Document39 pagesPBL 2 GBMS 3 YR1i4136357No ratings yet
- Endocrine Disorders Cont... (For ADRENAL GLAND)Document4 pagesEndocrine Disorders Cont... (For ADRENAL GLAND)Ernie G. Bautista II, RN, MD100% (3)
- 2 - Summary (A)Document3 pages2 - Summary (A)shougNo ratings yet
- ElectrolyteDocument4 pagesElectrolyteRon Vien'sNo ratings yet
- Alcohols Ethanol, MethanolDocument55 pagesAlcohols Ethanol, MethanoljayNo ratings yet
- NCM 106: Self Directed Learning Activity Name and Section: John Michael O. Villanueva BSN 2 ADocument4 pagesNCM 106: Self Directed Learning Activity Name and Section: John Michael O. Villanueva BSN 2 AKaye PatriarcaNo ratings yet
- Agricultural PoisonDocument25 pagesAgricultural Poisons.shreevarshiniNo ratings yet
- CN 118 - Assessment (Reviewer)Document5 pagesCN 118 - Assessment (Reviewer)Camille SanguyoNo ratings yet
- Drug TabulationDocument22 pagesDrug TabulationJam CorrosNo ratings yet
- Gastrointestinal: Nclex-Rn ReviewerDocument34 pagesGastrointestinal: Nclex-Rn ReviewerJohnasse Sebastian NavalNo ratings yet
- Ha Lab ReviewerDocument3 pagesHa Lab ReviewerzabalaiiirogeliopaclibarNo ratings yet
- NCLEX SampleDocument12 pagesNCLEX SampleYasser AhmedNo ratings yet
- Organophosphate PoisoningDocument19 pagesOrganophosphate PoisoningapokawNo ratings yet
- Syncope, A Simple Guide to the Condition, Treatment and Related DiseasesFrom EverandSyncope, A Simple Guide to the Condition, Treatment and Related DiseasesNo ratings yet
- Snoring, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandSnoring, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- HFN Mag Nov2019 Digital Pages 1Document84 pagesHFN Mag Nov2019 Digital Pages 1Sumanth Gundeti100% (1)
- Morbid Anxiety As A Risk Factor in Patients With Somatic Diseases A Review of Recent FindingsDocument9 pagesMorbid Anxiety As A Risk Factor in Patients With Somatic Diseases A Review of Recent FindingsAdelina AndritoiNo ratings yet
- Corticosteroid Injections - Their Use and AbuseDocument8 pagesCorticosteroid Injections - Their Use and AbuseSergiu PlescaNo ratings yet
- Is It Sjogren's Syndrome or Burning Mouth SyndromeDocument25 pagesIs It Sjogren's Syndrome or Burning Mouth SyndromeGentianaNo ratings yet
- 8-Human Health and Disease Extra Questions-1Document14 pages8-Human Health and Disease Extra Questions-1Poonam PathakNo ratings yet
- Palatal Fistula: Dr. Amru Sungkar, SPB-SPBPDocument48 pagesPalatal Fistula: Dr. Amru Sungkar, SPB-SPBPlukhoriNo ratings yet
- Personal View: Anita Thapar, Miriam Cooper, Michael Rutter FrcpsychDocument8 pagesPersonal View: Anita Thapar, Miriam Cooper, Michael Rutter FrcpsychRaul Morales VillegasNo ratings yet
- 51 Diseases of Ruminants - Dr. SulaDocument92 pages51 Diseases of Ruminants - Dr. SulaCholid MawardiNo ratings yet
- Endocrine Disorders Worksheetanskey2012-1Document5 pagesEndocrine Disorders Worksheetanskey2012-1mezuniga1100% (1)
- Intermediate 3 - Alp Project: Option 3: (For Pair or Group Presentations)Document2 pagesIntermediate 3 - Alp Project: Option 3: (For Pair or Group Presentations)Gary Yauri MayorcaNo ratings yet
- A Brief Review of Remedial Uses of Saussurea LappaDocument8 pagesA Brief Review of Remedial Uses of Saussurea LappaTuan NguyenNo ratings yet
- 3 CJ's Informed Consent FormDocument4 pages3 CJ's Informed Consent FormCleonJosephNo ratings yet
- Diabetes Information BookletDocument28 pagesDiabetes Information BookletheenamodiNo ratings yet
- Nursing Care Plan - HyperDocument4 pagesNursing Care Plan - HyperJennalyn Casapao100% (1)
- NF - DR - Concept Map - Week 11Document3 pagesNF - DR - Concept Map - Week 11Kyra Bianca R. FamacionNo ratings yet
- Physicalfitness 110622070341 Phpapp02Document19 pagesPhysicalfitness 110622070341 Phpapp02Judylyn Miana BanataoNo ratings yet
- NRCM0112 - Handout - Chronic IllnessDocument2 pagesNRCM0112 - Handout - Chronic IllnessYuuki Chitose (tai-kun)No ratings yet
- Anxiety and Sports Performance in Young FemalesDocument11 pagesAnxiety and Sports Performance in Young FemalesGuille monsterNo ratings yet
- Due 6 March 2018, 9:30am Attached To Bcourses: PH150E/CP117AC: Community Health - HW Assignment #3 Spring 2018Document7 pagesDue 6 March 2018, 9:30am Attached To Bcourses: PH150E/CP117AC: Community Health - HW Assignment #3 Spring 2018Megha BanerjeeNo ratings yet
- Cognitive and Psychopathological Aspects of Ehlers DanlosDocument5 pagesCognitive and Psychopathological Aspects of Ehlers DanlosKarel GuevaraNo ratings yet
- CBQDocument14 pagesCBQHamad RayhanNo ratings yet
- SK 2 ClassDocument11 pagesSK 2 ClasshcbbNo ratings yet
- Brain Herniation SyndromeDocument28 pagesBrain Herniation SyndromeSarahScandy100% (4)
- Causes of ObesityDocument3 pagesCauses of ObesityKaren Chambre100% (1)
- CPLD 2019Document10 pagesCPLD 2019sriNo ratings yet
- S O C R A T E S: History TakingDocument5 pagesS O C R A T E S: History Takingsnanan100% (1)
- A Accentuated Premorbid TraitsDocument50 pagesA Accentuated Premorbid TraitsJohnNo ratings yet
























































































Download as pdf or txt
You might also like
- MEDICAL - SURGICAL by John RicafortDocument9 pagesMEDICAL - SURGICAL by John RicafortTazneem Apostol Esmael100% (2)
- Top 200 Sorted by Drug ClassDocument3 pagesTop 200 Sorted by Drug Classthompjo2394100% (7)
- The Cure For HIV and AIDS by Hulda Regehr ClarkDocument612 pagesThe Cure For HIV and AIDS by Hulda Regehr ClarkRobert Glen Murrell Jr100% (3)
- Medical Surgical Nursing With MnemonicsDocument111 pagesMedical Surgical Nursing With MnemonicsChernobyle Tolentino BattadNo ratings yet
- Care Health ProposalDocument12 pagesCare Health ProposalNaldre Phamhinthuan100% (1)
- Arsenic: What Is Arsenicosis ?Document24 pagesArsenic: What Is Arsenicosis ?Wasi OsmanNo ratings yet
- Midterms RLEDocument11 pagesMidterms RLEgungonfiona28No ratings yet
- COPD , RLD , SLD3Document16 pagesCOPD , RLD , SLD342n8whjhrmNo ratings yet
- Vomiting of Gastrointestinal OriginDocument4 pagesVomiting of Gastrointestinal OriginFathimathNo ratings yet
- Organophosphorus PoisoningDocument15 pagesOrganophosphorus PoisoningtaufiAmaneeNo ratings yet
- Paraquot - Organophosphate Poisoning - Short NoteDocument2 pagesParaquot - Organophosphate Poisoning - Short NoteLahiru UpendraNo ratings yet
- Organic AcidsDocument3 pagesOrganic Acidsapi-26123997No ratings yet
- AlkaloidsDocument10 pagesAlkaloidsrazan assadNo ratings yet
- Poisoning & EnvenomationDocument19 pagesPoisoning & EnvenomationVirendra K. GajbhiyeNo ratings yet
- Vih MT#2Document8 pagesVih MT#2cjNo ratings yet
- Phctlec - Topic 3&4 - PrelimsDocument24 pagesPhctlec - Topic 3&4 - PrelimsasdfdjfeonaNo ratings yet
- MS MidtermDocument3 pagesMS MidtermDaphney Ruth LeocadioNo ratings yet
- PneumoniaDocument2 pagesPneumoniama7moud farsNo ratings yet
- 2.drugs Acting On The EyeDocument19 pages2.drugs Acting On The EyeEman MohamedNo ratings yet
- Kerosene PoisonDocument3 pagesKerosene PoisonAfnan ShaikhNo ratings yet
- Pleural Conditions Arf Ards PeDocument4 pagesPleural Conditions Arf Ards PeNoreen PadillaNo ratings yet
- Cardiac Poison: DR Bibek Raj ParajuliDocument23 pagesCardiac Poison: DR Bibek Raj Parajuliranjithreddy916gmailNo ratings yet
- DependenceDocument2 pagesDependenceObaid EllafyNo ratings yet
- Pedia - Intensive PhaseDocument2 pagesPedia - Intensive Phasepasabay270No ratings yet
- ABG NotesDocument2 pagesABG NotesIsland RaeNo ratings yet
- Chapter 14 - General Emergencies and Major TraumaDocument28 pagesChapter 14 - General Emergencies and Major Traumasnowlover boyNo ratings yet
- Handout 5 CardioVascular System Overview (Recovered)Document7 pagesHandout 5 CardioVascular System Overview (Recovered)Orlyn Joy TanaweNo ratings yet
- High Ent YielDocument15 pagesHigh Ent YielJana AldourNo ratings yet
- Indicator HCO:H CO Ratio Cause / Direction Etiology ConditionsDocument1 pageIndicator HCO:H CO Ratio Cause / Direction Etiology ConditionsSalve Rachelle BillenaNo ratings yet
- Compilation of Ms NotesDocument49 pagesCompilation of Ms Noteschoyaks100% (1)
- Cardiovascular Disease NCPDocument6 pagesCardiovascular Disease NCPsprrwgoldenNo ratings yet
- Ammonia Manganese: AstrocytesDocument2 pagesAmmonia Manganese: AstrocytesJULIUS ART VINCENT A. PADINITNo ratings yet
- NCM 116 - Neurologic Disorders (MODULE 1)Document6 pagesNCM 116 - Neurologic Disorders (MODULE 1)Meryville JacildoNo ratings yet
- Oral RevalidaDocument14 pagesOral RevalidaAyaBasilioNo ratings yet
- OXYGINATION FUNDA LEC BebeDocument8 pagesOXYGINATION FUNDA LEC BebediarosedoloresbsncNo ratings yet
- PoisoningDocument2 pagesPoisoninggoyaNo ratings yet
- Cinchona - Quinin PoisoningDocument7 pagesCinchona - Quinin PoisoninghariniNo ratings yet
- Oxygen, Nutri, ElimDocument74 pagesOxygen, Nutri, ElimNina Anne ParacadNo ratings yet
- Inhalation Injury and Systemic IntoxicationDocument7 pagesInhalation Injury and Systemic IntoxicationDaniel LesmanaNo ratings yet
- Scleroderma (Harrison's Principle of Internal Medicine)Document3 pagesScleroderma (Harrison's Principle of Internal Medicine)Pia Therese NatividadNo ratings yet
- Local AnestheticsgfhgjhkjlkDocument3 pagesLocal AnestheticsgfhgjhkjlkMuhammed BarznjiNo ratings yet
- General Examination (COMPLEXION) by Dr. Rana Moustafa AlsayedDocument18 pagesGeneral Examination (COMPLEXION) by Dr. Rana Moustafa AlsayedAbdulla1999 AshrafNo ratings yet
- Hypoxia: Lori HolmesDocument5 pagesHypoxia: Lori HolmesDanson Githinji ENo ratings yet
- Thyroid Gland OSCE ExaminationDocument13 pagesThyroid Gland OSCE ExaminationkylieverNo ratings yet
- Phctlec - Topic 3 - PrelimsDocument10 pagesPhctlec - Topic 3 - PrelimsasdfdjfeonaNo ratings yet
- Copd - Midterm NotesDocument2 pagesCopd - Midterm NotesInday BertaNo ratings yet
- Diabetes MellitusDocument3 pagesDiabetes MellitusShan NaseoulNo ratings yet
- Drug StudyDocument7 pagesDrug StudyAlliah OrdanNo ratings yet
- PBL 2 GBMS 3 YR1Document39 pagesPBL 2 GBMS 3 YR1i4136357No ratings yet
- Endocrine Disorders Cont... (For ADRENAL GLAND)Document4 pagesEndocrine Disorders Cont... (For ADRENAL GLAND)Ernie G. Bautista II, RN, MD100% (3)
- 2 - Summary (A)Document3 pages2 - Summary (A)shougNo ratings yet
- ElectrolyteDocument4 pagesElectrolyteRon Vien'sNo ratings yet
- Alcohols Ethanol, MethanolDocument55 pagesAlcohols Ethanol, MethanoljayNo ratings yet
- NCM 106: Self Directed Learning Activity Name and Section: John Michael O. Villanueva BSN 2 ADocument4 pagesNCM 106: Self Directed Learning Activity Name and Section: John Michael O. Villanueva BSN 2 AKaye PatriarcaNo ratings yet
- Agricultural PoisonDocument25 pagesAgricultural Poisons.shreevarshiniNo ratings yet
- CN 118 - Assessment (Reviewer)Document5 pagesCN 118 - Assessment (Reviewer)Camille SanguyoNo ratings yet
- Drug TabulationDocument22 pagesDrug TabulationJam CorrosNo ratings yet
- Gastrointestinal: Nclex-Rn ReviewerDocument34 pagesGastrointestinal: Nclex-Rn ReviewerJohnasse Sebastian NavalNo ratings yet
- Ha Lab ReviewerDocument3 pagesHa Lab ReviewerzabalaiiirogeliopaclibarNo ratings yet
- NCLEX SampleDocument12 pagesNCLEX SampleYasser AhmedNo ratings yet
- Organophosphate PoisoningDocument19 pagesOrganophosphate PoisoningapokawNo ratings yet
- Syncope, A Simple Guide to the Condition, Treatment and Related DiseasesFrom EverandSyncope, A Simple Guide to the Condition, Treatment and Related DiseasesNo ratings yet
- Snoring, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandSnoring, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- HFN Mag Nov2019 Digital Pages 1Document84 pagesHFN Mag Nov2019 Digital Pages 1Sumanth Gundeti100% (1)
- Morbid Anxiety As A Risk Factor in Patients With Somatic Diseases A Review of Recent FindingsDocument9 pagesMorbid Anxiety As A Risk Factor in Patients With Somatic Diseases A Review of Recent FindingsAdelina AndritoiNo ratings yet
- Corticosteroid Injections - Their Use and AbuseDocument8 pagesCorticosteroid Injections - Their Use and AbuseSergiu PlescaNo ratings yet
- Is It Sjogren's Syndrome or Burning Mouth SyndromeDocument25 pagesIs It Sjogren's Syndrome or Burning Mouth SyndromeGentianaNo ratings yet
- 8-Human Health and Disease Extra Questions-1Document14 pages8-Human Health and Disease Extra Questions-1Poonam PathakNo ratings yet
- Palatal Fistula: Dr. Amru Sungkar, SPB-SPBPDocument48 pagesPalatal Fistula: Dr. Amru Sungkar, SPB-SPBPlukhoriNo ratings yet
- Personal View: Anita Thapar, Miriam Cooper, Michael Rutter FrcpsychDocument8 pagesPersonal View: Anita Thapar, Miriam Cooper, Michael Rutter FrcpsychRaul Morales VillegasNo ratings yet
- 51 Diseases of Ruminants - Dr. SulaDocument92 pages51 Diseases of Ruminants - Dr. SulaCholid MawardiNo ratings yet
- Endocrine Disorders Worksheetanskey2012-1Document5 pagesEndocrine Disorders Worksheetanskey2012-1mezuniga1100% (1)
- Intermediate 3 - Alp Project: Option 3: (For Pair or Group Presentations)Document2 pagesIntermediate 3 - Alp Project: Option 3: (For Pair or Group Presentations)Gary Yauri MayorcaNo ratings yet
- A Brief Review of Remedial Uses of Saussurea LappaDocument8 pagesA Brief Review of Remedial Uses of Saussurea LappaTuan NguyenNo ratings yet
- 3 CJ's Informed Consent FormDocument4 pages3 CJ's Informed Consent FormCleonJosephNo ratings yet
- Diabetes Information BookletDocument28 pagesDiabetes Information BookletheenamodiNo ratings yet
- Nursing Care Plan - HyperDocument4 pagesNursing Care Plan - HyperJennalyn Casapao100% (1)
- NF - DR - Concept Map - Week 11Document3 pagesNF - DR - Concept Map - Week 11Kyra Bianca R. FamacionNo ratings yet
- Physicalfitness 110622070341 Phpapp02Document19 pagesPhysicalfitness 110622070341 Phpapp02Judylyn Miana BanataoNo ratings yet
- NRCM0112 - Handout - Chronic IllnessDocument2 pagesNRCM0112 - Handout - Chronic IllnessYuuki Chitose (tai-kun)No ratings yet
- Anxiety and Sports Performance in Young FemalesDocument11 pagesAnxiety and Sports Performance in Young FemalesGuille monsterNo ratings yet
- Due 6 March 2018, 9:30am Attached To Bcourses: PH150E/CP117AC: Community Health - HW Assignment #3 Spring 2018Document7 pagesDue 6 March 2018, 9:30am Attached To Bcourses: PH150E/CP117AC: Community Health - HW Assignment #3 Spring 2018Megha BanerjeeNo ratings yet
- Cognitive and Psychopathological Aspects of Ehlers DanlosDocument5 pagesCognitive and Psychopathological Aspects of Ehlers DanlosKarel GuevaraNo ratings yet
- CBQDocument14 pagesCBQHamad RayhanNo ratings yet
- SK 2 ClassDocument11 pagesSK 2 ClasshcbbNo ratings yet
- Brain Herniation SyndromeDocument28 pagesBrain Herniation SyndromeSarahScandy100% (4)
- Causes of ObesityDocument3 pagesCauses of ObesityKaren Chambre100% (1)
- CPLD 2019Document10 pagesCPLD 2019sriNo ratings yet
- S O C R A T E S: History TakingDocument5 pagesS O C R A T E S: History Takingsnanan100% (1)
- A Accentuated Premorbid TraitsDocument50 pagesA Accentuated Premorbid TraitsJohnNo ratings yet