
The COVID 19 Pandemic Bereavement Experiences Bet
The COVID 19 Pandemic Bereavement Experiences Bet
You might also like
- Beginners Guide To Blackwork by Lesley Wilkins2 PDFDocument63 pagesBeginners Guide To Blackwork by Lesley Wilkins2 PDFSCP100% (4)
- Historic CostumesDocument140 pagesHistoric CostumesDivya Manivannan100% (2)
- Open Letter To ICE From Medical Professionals Re COVID-19Document68 pagesOpen Letter To ICE From Medical Professionals Re COVID-19Jesus Garcia0% (1)
- Special Quadrilaterals: Honors GeometryDocument38 pagesSpecial Quadrilaterals: Honors GeometryMuhammad MirzaNo ratings yet
- PIIS0885392420302074Document15 pagesPIIS0885392420302074Félix IGNo ratings yet
- Palliative Care Article CritiqueDocument9 pagesPalliative Care Article Critiqueapi-577388355No ratings yet
- Bereavement Support On The Frontline of COVID 19 - 2020 - Journal of Pain andDocument6 pagesBereavement Support On The Frontline of COVID 19 - 2020 - Journal of Pain andIndiara MartinsNo ratings yet
- Psychiatry Amid COVID-19 The Sri Lankan ExperienceDocument3 pagesPsychiatry Amid COVID-19 The Sri Lankan ExperienceSteveNo ratings yet
- Uncertainty and COVID-19Document6 pagesUncertainty and COVID-19Arthur FernandesNo ratings yet
- Psychological Well-Being of Australian Hospital Clinical Staff During The COVID-19 PandemicDocument9 pagesPsychological Well-Being of Australian Hospital Clinical Staff During The COVID-19 PandemicAugresia Ines ChristianiNo ratings yet
- COVID-19 and Medical Professionalism in A Pandemic: Denis HarkinDocument2 pagesCOVID-19 and Medical Professionalism in A Pandemic: Denis HarkinJordz PlaciNo ratings yet
- The Impact of The COVID-19 Pandemic On The MentalDocument5 pagesThe Impact of The COVID-19 Pandemic On The MentalDAGOBERTO COPETE MOSQUERANo ratings yet
- Untold Stories of A Person With A Relative Who Died From Covid 19 Upon Death and On Upon DiagnosisDocument53 pagesUntold Stories of A Person With A Relative Who Died From Covid 19 Upon Death and On Upon DiagnosisMiss OpinionatedNo ratings yet
- Coronavirus On The Inpatient Unit: A New Challenge For Psychiatry - MDedge PsychiatryDocument3 pagesCoronavirus On The Inpatient Unit: A New Challenge For Psychiatry - MDedge PsychiatryAKNTAI002No ratings yet
- Journal Reading - Palliative CareDocument3 pagesJournal Reading - Palliative CareCZAR VINCENT WAYNE SEVANDAL BAYLONNo ratings yet
- Coping With Drug Resistant Tuberculosis AlongsideDocument18 pagesCoping With Drug Resistant Tuberculosis AlongsideDoc Tor StrangeNo ratings yet
- Chapter 1 PR1Document11 pagesChapter 1 PR1Nanami MumuzunoNo ratings yet
- Grief During The COVID-19 Pandemic: Considerations For Palliative Care ProvidersDocument7 pagesGrief During The COVID-19 Pandemic: Considerations For Palliative Care ProvidersKarla Patricia Serrano IriasNo ratings yet
- Jamda: EditorialDocument4 pagesJamda: Editorialzaenal abidinNo ratings yet
- Evaluating Risk To People With Epilepsy During The COVID-19 Pandemic Preliminary Findings From The COV-E StudyDocument10 pagesEvaluating Risk To People With Epilepsy During The COVID-19 Pandemic Preliminary Findings From The COV-E StudyDezha DetiroNo ratings yet
- The Role of Family Doctor in Covid 19 PandemicDocument11 pagesThe Role of Family Doctor in Covid 19 PandemicAdsoni IndoNo ratings yet
- Ajbsr MS Id 001564Document3 pagesAjbsr MS Id 001564Rodrigo AlpizarNo ratings yet
- Greenhalgh Shridar Open Letter To CMOs PDFDocument3 pagesGreenhalgh Shridar Open Letter To CMOs PDFThe Guardian100% (4)
- Diebolt Award 23oct-13 PDFDocument115 pagesDiebolt Award 23oct-13 PDFRodMickleburghNo ratings yet
- 307 - Final Paper 2Document8 pages307 - Final Paper 2api-544244860No ratings yet
- Primarna Zdravstvena Zaćštita CovidDocument6 pagesPrimarna Zdravstvena Zaćštita CovidPetar PanNo ratings yet
- Introduction To Hospice and Palliative CareDocument16 pagesIntroduction To Hospice and Palliative Carepahat75252No ratings yet
- The Business Case To Care For Persons With Serious.9Document7 pagesThe Business Case To Care For Persons With Serious.9enfaraujoNo ratings yet
- Coronavirus Disease 2019 and Vaccination of Children and Adolescents - Prospects and Challenges - (ENG)Document6 pagesCoronavirus Disease 2019 and Vaccination of Children and Adolescents - Prospects and Challenges - (ENG)Handoko MuhammadNo ratings yet
- Group 4 Prelim Assignment 1Document5 pagesGroup 4 Prelim Assignment 1Angel Alexa Del MundoNo ratings yet
- Summary of Brian Tyson, George Fareed & Mathew Crawford's Overcoming the COVID DarknessFrom EverandSummary of Brian Tyson, George Fareed & Mathew Crawford's Overcoming the COVID DarknessNo ratings yet
- Covid 19 ResearchDocument1 pageCovid 19 ResearchAngel Alyza SisonNo ratings yet
- Substance Use Disorders and Telehealth in The COVID-19 Pandemic Era: A New OutlookDocument10 pagesSubstance Use Disorders and Telehealth in The COVID-19 Pandemic Era: A New OutlookRo M OyarzúnNo ratings yet
- Triumph and Sadness: Ness Acelle B. Cruz Grade 12-tvl A 09-28-21Document2 pagesTriumph and Sadness: Ness Acelle B. Cruz Grade 12-tvl A 09-28-21Ness Acelle CruzNo ratings yet
- Perspectives of Cancer Patients and Their Health During The COVID-19 PandemicDocument10 pagesPerspectives of Cancer Patients and Their Health During The COVID-19 PandemicMatheus de AssisNo ratings yet
- Stress-Level-and-Psychological Well-BeingDocument37 pagesStress-Level-and-Psychological Well-BeingRafael RetubisNo ratings yet
- Psychological Distress, Coping Behaviors, and Preferences For Support Among New York Healthcare Workers During The COVID-19 PandemicDocument36 pagesPsychological Distress, Coping Behaviors, and Preferences For Support Among New York Healthcare Workers During The COVID-19 PandemicArgenis SalinasNo ratings yet
- Maximizing The Calm Before The Storm: Tiered Surgical Response Plan For Novel Coronavirus (COVID-19)Document31 pagesMaximizing The Calm Before The Storm: Tiered Surgical Response Plan For Novel Coronavirus (COVID-19)drwagnerzaoNo ratings yet
- Experiences That Were Encoiuntered by Fronline WokersDocument5 pagesExperiences That Were Encoiuntered by Fronline WokersNcube BonganiNo ratings yet
- Clinical Practice Guideline For The Evaluation of Fever and Infection in Older Adult Residents of Long-Term Care Facilities - 2008 Update by The Infectious Diseases Society of AmericaDocument23 pagesClinical Practice Guideline For The Evaluation of Fever and Infection in Older Adult Residents of Long-Term Care Facilities - 2008 Update by The Infectious Diseases Society of AmericaReyner LeonNo ratings yet
- Ne NR 2021-10-01 Response Vaccine Concerns MisinformationDocument8 pagesNe NR 2021-10-01 Response Vaccine Concerns MisinformationCTV CalgaryNo ratings yet
- Eccleston Covid 19 TR PAIN in PressDocument21 pagesEccleston Covid 19 TR PAIN in PressAhsan AzamNo ratings yet
- Psychiatry Research: A B C B D e F G BDocument5 pagesPsychiatry Research: A B C B D e F G BSandi Rizki ArdiantoNo ratings yet
- Kid 0004662020Document8 pagesKid 0004662020Rian KurniawanNo ratings yet
- Opn 12362Document10 pagesOpn 12362Argonne Robert AblanqueNo ratings yet
- Palliative Care For The Geriatric Anesthesiologist: Allen N. Gustin JR,, Rebecca A. AslaksonDocument12 pagesPalliative Care For The Geriatric Anesthesiologist: Allen N. Gustin JR,, Rebecca A. AslaksonAyu Diah Sri Krisnayanti PutuNo ratings yet
- Critical Care Nurse Burnout, Moral Distress, and Mental Health During The COVID-19 Pandemic - A United States SurveyDocument8 pagesCritical Care Nurse Burnout, Moral Distress, and Mental Health During The COVID-19 Pandemic - A United States SurveyBiblioteca Médica CDS -HGZcMF-1No ratings yet
- Covid-19: Clinical and Public Health Implications of Sars-Cov-2 ImmunologyDocument2 pagesCovid-19: Clinical and Public Health Implications of Sars-Cov-2 ImmunologysilviaNo ratings yet
- Prioritizing COVID 19 Vaccination For People With Severe Mental IllnessDocument3 pagesPrioritizing COVID 19 Vaccination For People With Severe Mental IllnessshishichanNo ratings yet
- DCCN 40 156Document8 pagesDCCN 40 156liyana SyatirahNo ratings yet
- LTCcovid Country Reports - Canada - June 4 2020Document18 pagesLTCcovid Country Reports - Canada - June 4 2020Nancy FloresNo ratings yet
- Current Scenario For Management On Covid-19 - A Global Review Indra S, Vijayasankari A, Kalpana SDocument5 pagesCurrent Scenario For Management On Covid-19 - A Global Review Indra S, Vijayasankari A, Kalpana Snithish krishnaNo ratings yet
- LONG COVID CallardDocument5 pagesLONG COVID CallardIchlasul MadriddistaNo ratings yet
- Advancing Palliative Care As A Human RightDocument8 pagesAdvancing Palliative Care As A Human Rightw89qyccn6sNo ratings yet
- AvaDocument13 pagesAvaapi-609535917No ratings yet
- Senator Hall Letterto Gov Abbotton COVIDTreatmentDocument4 pagesSenator Hall Letterto Gov Abbotton COVIDTreatmentThe TexanNo ratings yet
- 17 FullDocument8 pages17 FullcharmyshkuNo ratings yet
- Covid 19 and Indigenous ChildrenDocument3 pagesCovid 19 and Indigenous ChildrenJenny Vieb CaspilloNo ratings yet
- Humanism in The Age of COVID-19Document5 pagesHumanism in The Age of COVID-19Jhoelis SalazarNo ratings yet
- A Pain-Free' Death: Fiona Hicks and Elizabeth ReesDocument19 pagesA Pain-Free' Death: Fiona Hicks and Elizabeth Reesbdalcin5512No ratings yet
- 1 s2.0 S0002934320302072 MainDocument3 pages1 s2.0 S0002934320302072 Mainambi bidullahNo ratings yet
- BROKEN: How the Global Pandemic Uncovered a Nursing Home System in Need of Repair and the Heroic Staff Fighting for ChangeFrom EverandBROKEN: How the Global Pandemic Uncovered a Nursing Home System in Need of Repair and the Heroic Staff Fighting for ChangeNo ratings yet
- The Impact of Advance Care Planning on HealthcareDocument15 pagesThe Impact of Advance Care Planning on HealthcareDwi NovitasariNo ratings yet
- Dwi YuniartiDocument8 pagesDwi YuniartiDwi NovitasariNo ratings yet
- Ayu Oktaviani 202313032Document12 pagesAyu Oktaviani 202313032Dwi NovitasariNo ratings yet
- Dwi NovvvDocument18 pagesDwi NovvvDwi NovitasariNo ratings yet
- The Cold War: DétenteDocument20 pagesThe Cold War: Détentebye hiNo ratings yet
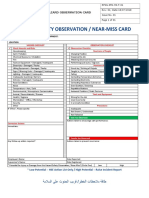
- RPSG-IMS-HS-F - 01 - Hazard Observation CardDocument2 pagesRPSG-IMS-HS-F - 01 - Hazard Observation CardRocky BisNo ratings yet
- I. Read The Text Carefully, Then Answer The Questions!Document5 pagesI. Read The Text Carefully, Then Answer The Questions!Herry SusiloNo ratings yet
- Procedures For Rapid Deployment, Redeployment, and Retrograde Small ArmsDocument24 pagesProcedures For Rapid Deployment, Redeployment, and Retrograde Small ArmsC.A. MonroeNo ratings yet
- 18 Pros and Cons of Being An Employee vs. An Entrepreneur - The LaddersDocument6 pages18 Pros and Cons of Being An Employee vs. An Entrepreneur - The Laddersهيثم سميرNo ratings yet
- Corrosion Prevention and ControlDocument19 pagesCorrosion Prevention and ControlJosa FatyNo ratings yet
- Cape Sewing - Industrial Sewing TechnologyDocument33 pagesCape Sewing - Industrial Sewing TechnologyMonika GadgilNo ratings yet
- The Power of Faith Confession & WorshipDocument38 pagesThe Power of Faith Confession & WorshipLarryDelaCruz100% (1)
- DIGITAL MARKETING (Unit 4)Document9 pagesDIGITAL MARKETING (Unit 4)sharmapranav780No ratings yet
- Mutiple Choice Question For Satellite CommunicationDocument4 pagesMutiple Choice Question For Satellite CommunicationRaja Pirian67% (3)
- Bajaj Electricals Limited Vs Metals & Allied Products and Anr. On 4 August, 1987Document8 pagesBajaj Electricals Limited Vs Metals & Allied Products and Anr. On 4 August, 1987RajesureshNo ratings yet
- Aadarsh Nayak Chemistry ProjectDocument14 pagesAadarsh Nayak Chemistry ProjectExtra 2020No ratings yet
- Contoh Presentasi Bahasa Inggris Tentang Makanan 2Document4 pagesContoh Presentasi Bahasa Inggris Tentang Makanan 2ardian noorNo ratings yet
- Knowledge Management & Specialized Information SystemsDocument21 pagesKnowledge Management & Specialized Information SystemsAntonyNo ratings yet
- Part A: Grammar: (60 Marks)Document68 pagesPart A: Grammar: (60 Marks)RakibsowadNo ratings yet
- Kahit Maputi Na Ang Buhok KoDocument13 pagesKahit Maputi Na Ang Buhok KoLouie Kem Anthony Babaran100% (1)
- Chapter 8 - Memory Storage Devices Question AnswersDocument4 pagesChapter 8 - Memory Storage Devices Question AnswersAditya MalhotraNo ratings yet
- Early Journal Content On JSTOR, Free To Anyone in The WorldDocument52 pagesEarly Journal Content On JSTOR, Free To Anyone in The Worldmarc millisNo ratings yet
- Photo Essay PDFDocument2 pagesPhoto Essay PDFMartha Glorie Manalo WallisNo ratings yet
- Plaaf Trainng PhilosophyDocument46 pagesPlaaf Trainng Philosophyneetin vatsya100% (1)
- Raj'a (Returning) : Sermon of Amir Ul-MomineenDocument3 pagesRaj'a (Returning) : Sermon of Amir Ul-Momineentausif mewawalaNo ratings yet
- GPS World - January 2017Document77 pagesGPS World - January 2017Diego Franco100% (2)
- Clutch Palte - 1Document48 pagesClutch Palte - 1pramo_dassNo ratings yet
- PETRONAS RETAILER Price List - W.E.F 10-10-23Document2 pagesPETRONAS RETAILER Price List - W.E.F 10-10-23Mujeeb SiddiqueNo ratings yet
- Blog Profile: Activity A. " ". Complete El Perfil Con Su Información Personal en Los Espacios Indicados "Document5 pagesBlog Profile: Activity A. " ". Complete El Perfil Con Su Información Personal en Los Espacios Indicados "El dominadorNo ratings yet
- Deloitte Part-2 Task-2Document5 pagesDeloitte Part-2 Task-2Nelikondi RakeshNo ratings yet
- Strasser The Rational Basis of Trademark Protection RevisitedDocument58 pagesStrasser The Rational Basis of Trademark Protection RevisitedfedericosilvaNo ratings yet




























































































Download as pdf or txt
You might also like
- Beginners Guide To Blackwork by Lesley Wilkins2 PDFDocument63 pagesBeginners Guide To Blackwork by Lesley Wilkins2 PDFSCP100% (4)
- Historic CostumesDocument140 pagesHistoric CostumesDivya Manivannan100% (2)
- Open Letter To ICE From Medical Professionals Re COVID-19Document68 pagesOpen Letter To ICE From Medical Professionals Re COVID-19Jesus Garcia0% (1)
- Special Quadrilaterals: Honors GeometryDocument38 pagesSpecial Quadrilaterals: Honors GeometryMuhammad MirzaNo ratings yet
- PIIS0885392420302074Document15 pagesPIIS0885392420302074Félix IGNo ratings yet
- Palliative Care Article CritiqueDocument9 pagesPalliative Care Article Critiqueapi-577388355No ratings yet
- Bereavement Support On The Frontline of COVID 19 - 2020 - Journal of Pain andDocument6 pagesBereavement Support On The Frontline of COVID 19 - 2020 - Journal of Pain andIndiara MartinsNo ratings yet
- Psychiatry Amid COVID-19 The Sri Lankan ExperienceDocument3 pagesPsychiatry Amid COVID-19 The Sri Lankan ExperienceSteveNo ratings yet
- Uncertainty and COVID-19Document6 pagesUncertainty and COVID-19Arthur FernandesNo ratings yet
- Psychological Well-Being of Australian Hospital Clinical Staff During The COVID-19 PandemicDocument9 pagesPsychological Well-Being of Australian Hospital Clinical Staff During The COVID-19 PandemicAugresia Ines ChristianiNo ratings yet
- COVID-19 and Medical Professionalism in A Pandemic: Denis HarkinDocument2 pagesCOVID-19 and Medical Professionalism in A Pandemic: Denis HarkinJordz PlaciNo ratings yet
- The Impact of The COVID-19 Pandemic On The MentalDocument5 pagesThe Impact of The COVID-19 Pandemic On The MentalDAGOBERTO COPETE MOSQUERANo ratings yet
- Untold Stories of A Person With A Relative Who Died From Covid 19 Upon Death and On Upon DiagnosisDocument53 pagesUntold Stories of A Person With A Relative Who Died From Covid 19 Upon Death and On Upon DiagnosisMiss OpinionatedNo ratings yet
- Coronavirus On The Inpatient Unit: A New Challenge For Psychiatry - MDedge PsychiatryDocument3 pagesCoronavirus On The Inpatient Unit: A New Challenge For Psychiatry - MDedge PsychiatryAKNTAI002No ratings yet
- Journal Reading - Palliative CareDocument3 pagesJournal Reading - Palliative CareCZAR VINCENT WAYNE SEVANDAL BAYLONNo ratings yet
- Coping With Drug Resistant Tuberculosis AlongsideDocument18 pagesCoping With Drug Resistant Tuberculosis AlongsideDoc Tor StrangeNo ratings yet
- Chapter 1 PR1Document11 pagesChapter 1 PR1Nanami MumuzunoNo ratings yet
- Grief During The COVID-19 Pandemic: Considerations For Palliative Care ProvidersDocument7 pagesGrief During The COVID-19 Pandemic: Considerations For Palliative Care ProvidersKarla Patricia Serrano IriasNo ratings yet
- Jamda: EditorialDocument4 pagesJamda: Editorialzaenal abidinNo ratings yet
- Evaluating Risk To People With Epilepsy During The COVID-19 Pandemic Preliminary Findings From The COV-E StudyDocument10 pagesEvaluating Risk To People With Epilepsy During The COVID-19 Pandemic Preliminary Findings From The COV-E StudyDezha DetiroNo ratings yet
- The Role of Family Doctor in Covid 19 PandemicDocument11 pagesThe Role of Family Doctor in Covid 19 PandemicAdsoni IndoNo ratings yet
- Ajbsr MS Id 001564Document3 pagesAjbsr MS Id 001564Rodrigo AlpizarNo ratings yet
- Greenhalgh Shridar Open Letter To CMOs PDFDocument3 pagesGreenhalgh Shridar Open Letter To CMOs PDFThe Guardian100% (4)
- Diebolt Award 23oct-13 PDFDocument115 pagesDiebolt Award 23oct-13 PDFRodMickleburghNo ratings yet
- 307 - Final Paper 2Document8 pages307 - Final Paper 2api-544244860No ratings yet
- Primarna Zdravstvena Zaćštita CovidDocument6 pagesPrimarna Zdravstvena Zaćštita CovidPetar PanNo ratings yet
- Introduction To Hospice and Palliative CareDocument16 pagesIntroduction To Hospice and Palliative Carepahat75252No ratings yet
- The Business Case To Care For Persons With Serious.9Document7 pagesThe Business Case To Care For Persons With Serious.9enfaraujoNo ratings yet
- Coronavirus Disease 2019 and Vaccination of Children and Adolescents - Prospects and Challenges - (ENG)Document6 pagesCoronavirus Disease 2019 and Vaccination of Children and Adolescents - Prospects and Challenges - (ENG)Handoko MuhammadNo ratings yet
- Group 4 Prelim Assignment 1Document5 pagesGroup 4 Prelim Assignment 1Angel Alexa Del MundoNo ratings yet
- Summary of Brian Tyson, George Fareed & Mathew Crawford's Overcoming the COVID DarknessFrom EverandSummary of Brian Tyson, George Fareed & Mathew Crawford's Overcoming the COVID DarknessNo ratings yet
- Covid 19 ResearchDocument1 pageCovid 19 ResearchAngel Alyza SisonNo ratings yet
- Substance Use Disorders and Telehealth in The COVID-19 Pandemic Era: A New OutlookDocument10 pagesSubstance Use Disorders and Telehealth in The COVID-19 Pandemic Era: A New OutlookRo M OyarzúnNo ratings yet
- Triumph and Sadness: Ness Acelle B. Cruz Grade 12-tvl A 09-28-21Document2 pagesTriumph and Sadness: Ness Acelle B. Cruz Grade 12-tvl A 09-28-21Ness Acelle CruzNo ratings yet
- Perspectives of Cancer Patients and Their Health During The COVID-19 PandemicDocument10 pagesPerspectives of Cancer Patients and Their Health During The COVID-19 PandemicMatheus de AssisNo ratings yet
- Stress-Level-and-Psychological Well-BeingDocument37 pagesStress-Level-and-Psychological Well-BeingRafael RetubisNo ratings yet
- Psychological Distress, Coping Behaviors, and Preferences For Support Among New York Healthcare Workers During The COVID-19 PandemicDocument36 pagesPsychological Distress, Coping Behaviors, and Preferences For Support Among New York Healthcare Workers During The COVID-19 PandemicArgenis SalinasNo ratings yet
- Maximizing The Calm Before The Storm: Tiered Surgical Response Plan For Novel Coronavirus (COVID-19)Document31 pagesMaximizing The Calm Before The Storm: Tiered Surgical Response Plan For Novel Coronavirus (COVID-19)drwagnerzaoNo ratings yet
- Experiences That Were Encoiuntered by Fronline WokersDocument5 pagesExperiences That Were Encoiuntered by Fronline WokersNcube BonganiNo ratings yet
- Clinical Practice Guideline For The Evaluation of Fever and Infection in Older Adult Residents of Long-Term Care Facilities - 2008 Update by The Infectious Diseases Society of AmericaDocument23 pagesClinical Practice Guideline For The Evaluation of Fever and Infection in Older Adult Residents of Long-Term Care Facilities - 2008 Update by The Infectious Diseases Society of AmericaReyner LeonNo ratings yet
- Ne NR 2021-10-01 Response Vaccine Concerns MisinformationDocument8 pagesNe NR 2021-10-01 Response Vaccine Concerns MisinformationCTV CalgaryNo ratings yet
- Eccleston Covid 19 TR PAIN in PressDocument21 pagesEccleston Covid 19 TR PAIN in PressAhsan AzamNo ratings yet
- Psychiatry Research: A B C B D e F G BDocument5 pagesPsychiatry Research: A B C B D e F G BSandi Rizki ArdiantoNo ratings yet
- Kid 0004662020Document8 pagesKid 0004662020Rian KurniawanNo ratings yet
- Opn 12362Document10 pagesOpn 12362Argonne Robert AblanqueNo ratings yet
- Palliative Care For The Geriatric Anesthesiologist: Allen N. Gustin JR,, Rebecca A. AslaksonDocument12 pagesPalliative Care For The Geriatric Anesthesiologist: Allen N. Gustin JR,, Rebecca A. AslaksonAyu Diah Sri Krisnayanti PutuNo ratings yet
- Critical Care Nurse Burnout, Moral Distress, and Mental Health During The COVID-19 Pandemic - A United States SurveyDocument8 pagesCritical Care Nurse Burnout, Moral Distress, and Mental Health During The COVID-19 Pandemic - A United States SurveyBiblioteca Médica CDS -HGZcMF-1No ratings yet
- Covid-19: Clinical and Public Health Implications of Sars-Cov-2 ImmunologyDocument2 pagesCovid-19: Clinical and Public Health Implications of Sars-Cov-2 ImmunologysilviaNo ratings yet
- Prioritizing COVID 19 Vaccination For People With Severe Mental IllnessDocument3 pagesPrioritizing COVID 19 Vaccination For People With Severe Mental IllnessshishichanNo ratings yet
- DCCN 40 156Document8 pagesDCCN 40 156liyana SyatirahNo ratings yet
- LTCcovid Country Reports - Canada - June 4 2020Document18 pagesLTCcovid Country Reports - Canada - June 4 2020Nancy FloresNo ratings yet
- Current Scenario For Management On Covid-19 - A Global Review Indra S, Vijayasankari A, Kalpana SDocument5 pagesCurrent Scenario For Management On Covid-19 - A Global Review Indra S, Vijayasankari A, Kalpana Snithish krishnaNo ratings yet
- LONG COVID CallardDocument5 pagesLONG COVID CallardIchlasul MadriddistaNo ratings yet
- Advancing Palliative Care As A Human RightDocument8 pagesAdvancing Palliative Care As A Human Rightw89qyccn6sNo ratings yet
- AvaDocument13 pagesAvaapi-609535917No ratings yet
- Senator Hall Letterto Gov Abbotton COVIDTreatmentDocument4 pagesSenator Hall Letterto Gov Abbotton COVIDTreatmentThe TexanNo ratings yet
- 17 FullDocument8 pages17 FullcharmyshkuNo ratings yet
- Covid 19 and Indigenous ChildrenDocument3 pagesCovid 19 and Indigenous ChildrenJenny Vieb CaspilloNo ratings yet
- Humanism in The Age of COVID-19Document5 pagesHumanism in The Age of COVID-19Jhoelis SalazarNo ratings yet
- A Pain-Free' Death: Fiona Hicks and Elizabeth ReesDocument19 pagesA Pain-Free' Death: Fiona Hicks and Elizabeth Reesbdalcin5512No ratings yet
- 1 s2.0 S0002934320302072 MainDocument3 pages1 s2.0 S0002934320302072 Mainambi bidullahNo ratings yet
- BROKEN: How the Global Pandemic Uncovered a Nursing Home System in Need of Repair and the Heroic Staff Fighting for ChangeFrom EverandBROKEN: How the Global Pandemic Uncovered a Nursing Home System in Need of Repair and the Heroic Staff Fighting for ChangeNo ratings yet
- The Impact of Advance Care Planning on HealthcareDocument15 pagesThe Impact of Advance Care Planning on HealthcareDwi NovitasariNo ratings yet
- Dwi YuniartiDocument8 pagesDwi YuniartiDwi NovitasariNo ratings yet
- Ayu Oktaviani 202313032Document12 pagesAyu Oktaviani 202313032Dwi NovitasariNo ratings yet
- Dwi NovvvDocument18 pagesDwi NovvvDwi NovitasariNo ratings yet
- The Cold War: DétenteDocument20 pagesThe Cold War: Détentebye hiNo ratings yet
- RPSG-IMS-HS-F - 01 - Hazard Observation CardDocument2 pagesRPSG-IMS-HS-F - 01 - Hazard Observation CardRocky BisNo ratings yet
- I. Read The Text Carefully, Then Answer The Questions!Document5 pagesI. Read The Text Carefully, Then Answer The Questions!Herry SusiloNo ratings yet
- Procedures For Rapid Deployment, Redeployment, and Retrograde Small ArmsDocument24 pagesProcedures For Rapid Deployment, Redeployment, and Retrograde Small ArmsC.A. MonroeNo ratings yet
- 18 Pros and Cons of Being An Employee vs. An Entrepreneur - The LaddersDocument6 pages18 Pros and Cons of Being An Employee vs. An Entrepreneur - The Laddersهيثم سميرNo ratings yet
- Corrosion Prevention and ControlDocument19 pagesCorrosion Prevention and ControlJosa FatyNo ratings yet
- Cape Sewing - Industrial Sewing TechnologyDocument33 pagesCape Sewing - Industrial Sewing TechnologyMonika GadgilNo ratings yet
- The Power of Faith Confession & WorshipDocument38 pagesThe Power of Faith Confession & WorshipLarryDelaCruz100% (1)
- DIGITAL MARKETING (Unit 4)Document9 pagesDIGITAL MARKETING (Unit 4)sharmapranav780No ratings yet
- Mutiple Choice Question For Satellite CommunicationDocument4 pagesMutiple Choice Question For Satellite CommunicationRaja Pirian67% (3)
- Bajaj Electricals Limited Vs Metals & Allied Products and Anr. On 4 August, 1987Document8 pagesBajaj Electricals Limited Vs Metals & Allied Products and Anr. On 4 August, 1987RajesureshNo ratings yet
- Aadarsh Nayak Chemistry ProjectDocument14 pagesAadarsh Nayak Chemistry ProjectExtra 2020No ratings yet
- Contoh Presentasi Bahasa Inggris Tentang Makanan 2Document4 pagesContoh Presentasi Bahasa Inggris Tentang Makanan 2ardian noorNo ratings yet
- Knowledge Management & Specialized Information SystemsDocument21 pagesKnowledge Management & Specialized Information SystemsAntonyNo ratings yet
- Part A: Grammar: (60 Marks)Document68 pagesPart A: Grammar: (60 Marks)RakibsowadNo ratings yet
- Kahit Maputi Na Ang Buhok KoDocument13 pagesKahit Maputi Na Ang Buhok KoLouie Kem Anthony Babaran100% (1)
- Chapter 8 - Memory Storage Devices Question AnswersDocument4 pagesChapter 8 - Memory Storage Devices Question AnswersAditya MalhotraNo ratings yet
- Early Journal Content On JSTOR, Free To Anyone in The WorldDocument52 pagesEarly Journal Content On JSTOR, Free To Anyone in The Worldmarc millisNo ratings yet
- Photo Essay PDFDocument2 pagesPhoto Essay PDFMartha Glorie Manalo WallisNo ratings yet
- Plaaf Trainng PhilosophyDocument46 pagesPlaaf Trainng Philosophyneetin vatsya100% (1)
- Raj'a (Returning) : Sermon of Amir Ul-MomineenDocument3 pagesRaj'a (Returning) : Sermon of Amir Ul-Momineentausif mewawalaNo ratings yet
- GPS World - January 2017Document77 pagesGPS World - January 2017Diego Franco100% (2)
- Clutch Palte - 1Document48 pagesClutch Palte - 1pramo_dassNo ratings yet
- PETRONAS RETAILER Price List - W.E.F 10-10-23Document2 pagesPETRONAS RETAILER Price List - W.E.F 10-10-23Mujeeb SiddiqueNo ratings yet
- Blog Profile: Activity A. " ". Complete El Perfil Con Su Información Personal en Los Espacios Indicados "Document5 pagesBlog Profile: Activity A. " ". Complete El Perfil Con Su Información Personal en Los Espacios Indicados "El dominadorNo ratings yet
- Deloitte Part-2 Task-2Document5 pagesDeloitte Part-2 Task-2Nelikondi RakeshNo ratings yet
- Strasser The Rational Basis of Trademark Protection RevisitedDocument58 pagesStrasser The Rational Basis of Trademark Protection RevisitedfedericosilvaNo ratings yet