Download as pdf or txt
You might also like
- Key Questions in Cardiac SurgeryDocument522 pagesKey Questions in Cardiac SurgeryRenan Petinelli100% (3)
- Phlebotomy Questions and Answers 2Document16 pagesPhlebotomy Questions and Answers 2emeki20029700100% (2)
- Anatomy and Physiology by Ross and WilsonDocument21 pagesAnatomy and Physiology by Ross and WilsonAnonymous iEjePNZ50% (2)
- Final Exam PracticeDocument6 pagesFinal Exam PracticeErvin T MileNo ratings yet
- Sci9 U1M1 LM v1.0Document27 pagesSci9 U1M1 LM v1.0catherinerenante50% (2)
- Chapter 23Document171 pagesChapter 23Arpit PradhanNo ratings yet
- My Study4Document9 pagesMy Study4محمد العراقيNo ratings yet
- Sistem Sirkulasi Dan RespirasiDocument35 pagesSistem Sirkulasi Dan RespirasiAnityo NugrohoNo ratings yet
- Cardiac Layers: Collage of Medicine Anatomy and Histology Department DR - Hameda A.GahziDocument8 pagesCardiac Layers: Collage of Medicine Anatomy and Histology Department DR - Hameda A.GahziJnn DstNo ratings yet
- Exercise 14 Circulatory SystemDocument9 pagesExercise 14 Circulatory SystemJovelou MihangosNo ratings yet
- Artery of head and neckDocument39 pagesArtery of head and neckJitendra SinhaNo ratings yet
- The circulatory system - Зүрх судасны тогтолцооDocument2 pagesThe circulatory system - Зүрх судасны тогтолцооKhaliun MyagmarNo ratings yet
- Histology of The CvsDocument25 pagesHistology of The CvsroqibniniolaNo ratings yet
- The Circulatory SystemDocument97 pagesThe Circulatory SystemoatcookiesNo ratings yet
- Cardio 2Document5 pagesCardio 2Liam Jacque LapuzNo ratings yet
- Circulatory SystemDocument29 pagesCirculatory Systemjosephsilva112No ratings yet
- Atlas Histology of HeartDocument2 pagesAtlas Histology of HeartYasir HadyNo ratings yet
- Histology of The Circulatory SystemDocument24 pagesHistology of The Circulatory SystemFatima Zehra YusefNo ratings yet
- Blood Vessels 2 PDFDocument25 pagesBlood Vessels 2 PDFVizhiNo ratings yet
- Human HeartDocument10 pagesHuman HeartRAHUL NISHADNo ratings yet
- BLOOD and CIRCULATIONDocument11 pagesBLOOD and CIRCULATIONKert trocioNo ratings yet
- Chapter 19 Anatomy and Physiology NotesDocument11 pagesChapter 19 Anatomy and Physiology NotesZachary WatsonNo ratings yet
- The Circulatory System: Introduction: Endothelium, The Muscular Tissue, and The Connective Tissue, Which IncludesDocument12 pagesThe Circulatory System: Introduction: Endothelium, The Muscular Tissue, and The Connective Tissue, Which IncludesYoussra SelimNo ratings yet
- Histology RCR1 CardioDocument3 pagesHistology RCR1 CardioeamcrawleyNo ratings yet
- Week 8 Assignment PDFDocument3 pagesWeek 8 Assignment PDFShreyasi DongreNo ratings yet
- Cardiovascular SystemDocument22 pagesCardiovascular SystemWadabiNo ratings yet
- 5053922cardiovascular SystemDocument7 pages5053922cardiovascular SystemHasham AhmadNo ratings yet
- Circulatory Sys.Document5 pagesCirculatory Sys.Fadhil Hussam AhmedNo ratings yet
- CVS3 Histo Dr. LinaDocument29 pagesCVS3 Histo Dr. Linamohammedtemes340No ratings yet
- Need For Circulatory SystemsDocument13 pagesNeed For Circulatory SystemsKevin LlorenteNo ratings yet
- Circulatory System PPT - 2022Document94 pagesCirculatory System PPT - 2022Eugene Osei AmoakoNo ratings yet
- Act 14Document9 pagesAct 14ETHELHYN JHANE MACOBNo ratings yet
- Body System II 4 Cardio 1Document49 pagesBody System II 4 Cardio 1rrq8cwk2gnNo ratings yet
- Classification of Blood VesselsDocument8 pagesClassification of Blood Vesselspioneergloria51No ratings yet
- 1.2 CVS Histology-1Document41 pages1.2 CVS Histology-1noorfaris6704No ratings yet
- Lec 4 HistologyDocument37 pagesLec 4 Histologyأ. علي محمدNo ratings yet
- Blood Vessels Structure and Function: Blok 8 Kardiovaskuler, Psik Fkik Umy Skenario 4Document15 pagesBlood Vessels Structure and Function: Blok 8 Kardiovaskuler, Psik Fkik Umy Skenario 4Hida HarisNo ratings yet
- Blood Vessels, AnatomyDocument20 pagesBlood Vessels, AnatomyAbu BakarNo ratings yet
- The Blood VesselsDocument6 pagesThe Blood VesselsLast AccNo ratings yet
- Histology of The Cardiovascular System#Document36 pagesHistology of The Cardiovascular System#DonaldNo ratings yet
- Cardiovascular System Blood VesselsDocument30 pagesCardiovascular System Blood VesselsNova BadongenNo ratings yet
- Circulatory SystemDocument14 pagesCirculatory Systemferdinand padillaNo ratings yet
- Cardiovascular SystemDocument8 pagesCardiovascular SystemBushra AlkaqaniNo ratings yet
- The Cardiovascular System: Blood Vessels: I. Overview of Blood Vessel Structure and FunctionDocument7 pagesThe Cardiovascular System: Blood Vessels: I. Overview of Blood Vessel Structure and FunctionAdam ButterworthNo ratings yet
- Physio SyllabusDocument28 pagesPhysio Syllabusaammarayyaz49No ratings yet
- Weeks 12-16 Learning ObjectivesDocument14 pagesWeeks 12-16 Learning ObjectivesAmber DavisNo ratings yet
- Blood Vessel - WikipediaDocument9 pagesBlood Vessel - Wikipediab mochiiNo ratings yet
- HeartyyDocument3 pagesHeartyyfdbp42kfs6No ratings yet
- Special CirculationDocument19 pagesSpecial Circulationapi-19824701No ratings yet
- Module 11 Blood VesselsDocument9 pagesModule 11 Blood VesselsMisha WilliamsNo ratings yet
- The Circulatory System 2021 Power PointDocument30 pagesThe Circulatory System 2021 Power PointHHHNo ratings yet
- 13 +the+Circulatory+SystemDocument77 pages13 +the+Circulatory+SystemAbi AntonyNo ratings yet
- Cardiac Muscle: Cardiac Muscle (Heart Muscle) Is One of The Three Major Types of MuscleDocument3 pagesCardiac Muscle: Cardiac Muscle (Heart Muscle) Is One of The Three Major Types of MuscleKim PayawalNo ratings yet
- Histology of The Cardiovascular System-t22-HDocument22 pagesHistology of The Cardiovascular System-t22-HSekry EyaNo ratings yet
- Cardiovascular System-Blood VesselsDocument21 pagesCardiovascular System-Blood Vesselshi1281011No ratings yet
- Circulatory SystemDocument14 pagesCirculatory Systemferdinand padillaNo ratings yet
- Circulatory System: Dr. AmtulDocument46 pagesCirculatory System: Dr. Amtulbravestone974No ratings yet
- Histology of Heart: Dr.M.Irfan Ashraf MBBS, MCPS, FcpsDocument24 pagesHistology of Heart: Dr.M.Irfan Ashraf MBBS, MCPS, FcpsDr-Arsalan ZahidNo ratings yet
- Coronary Artery Disease Cerebrovascular Disease Peripheral Artery DiseaseDocument59 pagesCoronary Artery Disease Cerebrovascular Disease Peripheral Artery DiseaseAdi Teruna EffendiNo ratings yet
- Blood VesselDocument3 pagesBlood VesselJo Louis CamiguingNo ratings yet
- Cardiovascular System From Veterinary Histology PRDocument28 pagesCardiovascular System From Veterinary Histology PRImran100% (1)
- Oleh Arif Yahya, DR., Mkes Laboratorium Histologi Program Pendidikan Dokter Universitas Islam MalangDocument74 pagesOleh Arif Yahya, DR., Mkes Laboratorium Histologi Program Pendidikan Dokter Universitas Islam MalangDenna Refnaldi SatryaNo ratings yet
- CVSDocument58 pagesCVSDoina SvetNo ratings yet
- Histo CVS Pro KGDocument96 pagesHisto CVS Pro KGADE DWINATA SUSILO PUTRINo ratings yet
- Microcirculation in Cardiovascular DiseasesFrom EverandMicrocirculation in Cardiovascular DiseasesEnrico Agabiti-RoseiNo ratings yet
- Congestive Heart Failure (CHF) Pathophysiology, Nursing, Treatment, Symptoms Heart Failure Part 1Document6 pagesCongestive Heart Failure (CHF) Pathophysiology, Nursing, Treatment, Symptoms Heart Failure Part 1ParallelNo ratings yet
- Reviewer Science Grade 9Document43 pagesReviewer Science Grade 9Earl AndreiNo ratings yet
- Acog Practice Bulletin: Pregnancy and Heart DiseaseDocument37 pagesAcog Practice Bulletin: Pregnancy and Heart Diseasereham mohamedNo ratings yet
- Arrows Consele PDFDocument221 pagesArrows Consele PDFIsai Lara OsoriaNo ratings yet
- Rule: P Waves From The SA Node Are UprightDocument13 pagesRule: P Waves From The SA Node Are UprightredroseeeeeeNo ratings yet
- Pharmacokinetics and Pharmacodynamics PDFDocument166 pagesPharmacokinetics and Pharmacodynamics PDFCarolina PosadaNo ratings yet
- KS4 Physical Education: The Circulatory SystemDocument36 pagesKS4 Physical Education: The Circulatory SystemAjay Pal NattNo ratings yet
- Edexcel IAL Biology Unit 1 NotesDocument27 pagesEdexcel IAL Biology Unit 1 NotesJoey Chan100% (3)
- Embryology Notes emDocument25 pagesEmbryology Notes emAnonymous IwWT90VyNo ratings yet
- 1 s2.0 S0735109722056030 MainDocument15 pages1 s2.0 S0735109722056030 MainAkhmad HidayatNo ratings yet
- Congestive Cardiac Failure PDFDocument28 pagesCongestive Cardiac Failure PDFNANDHINI S100% (1)
- Interpretation Chest X RayDocument127 pagesInterpretation Chest X RayVimal NishadNo ratings yet
- Life Process - TransportationDocument20 pagesLife Process - TransportationAARTI1012100% (1)
- HeartDocument22 pagesHeartNunoAlmeidaNo ratings yet
- Anaph111 - FinalsDocument7 pagesAnaph111 - FinalsUwen NalpNo ratings yet
- Current Management of Ebstein's Anomaly in The AdultDocument9 pagesCurrent Management of Ebstein's Anomaly in The AdultRJMNo ratings yet
- Daftar Singkatan SMF JAntungDocument5 pagesDaftar Singkatan SMF JAntungBobby RahmantoNo ratings yet
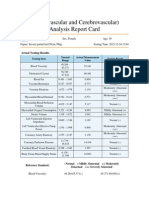
- Cardiovascular and CerebrovascularDocument6 pagesCardiovascular and CerebrovascularJoshelle B. Bancilo0% (1)
- 11.1 Multiple Choice Part I Questions: Chapter 11 The Cardiovascular SystemDocument33 pages11.1 Multiple Choice Part I Questions: Chapter 11 The Cardiovascular SystemmuryumNo ratings yet
- Cardiovascular MCQsDocument17 pagesCardiovascular MCQsRamadan PhysiologyNo ratings yet
- DextronixCatalog 0113bDocument15 pagesDextronixCatalog 0113bRóbert ŽuffaNo ratings yet
- Science (086) Set 31 2 2 Class X Marking Scheme 2020Document10 pagesScience (086) Set 31 2 2 Class X Marking Scheme 2020MeersNo ratings yet
- Research Paper On The Human HeartDocument5 pagesResearch Paper On The Human Heartfysfs7g3100% (1)
- Biology Questions and Answers Form 2Document41 pagesBiology Questions and Answers Form 2Zubin Jammaa FulaniNo ratings yet
- June 2016 Mark Scheme 41 PDFDocument10 pagesJune 2016 Mark Scheme 41 PDFediealiNo ratings yet