Download as pdf or txt
You might also like
- 1 All Study Guides (600 PAGES) - 231114 - 120241Document601 pages1 All Study Guides (600 PAGES) - 231114 - 120241marwajr2509100% (8)
- Overcoming Crystal Meth AddictionDocument356 pagesOvercoming Crystal Meth AddictionSarah Menz100% (3)
- CHN Skills Lab Module 2020Document138 pagesCHN Skills Lab Module 2020mysterioushumane100% (4)
- NSG Process Approach SeminarDocument15 pagesNSG Process Approach SeminarElsy MayjoNo ratings yet
- (New) Case Study FormatDocument7 pages(New) Case Study FormatSophia Sweet SantosNo ratings yet
- Proforma & Guideline For Case Presentation/Case StudyDocument9 pagesProforma & Guideline For Case Presentation/Case StudySwaraNo ratings yet
- Nursing Process DiagnosisDocument20 pagesNursing Process DiagnosisGabz Gabby100% (1)
- BLANK Nursing Process PaperDocument10 pagesBLANK Nursing Process PaperSNOOKI513No ratings yet
- CP 100 PrelimDocument38 pagesCP 100 PrelimDiana FernandezNo ratings yet
- Nursing Process DiagnosingDocument49 pagesNursing Process DiagnosingAnuchithra100% (2)
- ST JUDE CA2 Day 1 Note Taking GuideDocument4 pagesST JUDE CA2 Day 1 Note Taking Guidefaker than fakeNo ratings yet
- Nursing DXDocument5 pagesNursing DXSheena Marie M. TarleNo ratings yet
- Resume Irena Siska ManaluDocument3 pagesResume Irena Siska ManaluIrena Siska ManaluNo ratings yet
- Purpose: Characteristics of The Nursing ProcessDocument12 pagesPurpose: Characteristics of The Nursing ProcessVanessa Mae IlaganNo ratings yet
- Introduction To Nursing Process (NP) : Presenter:M.Salman Alam Nursing Instructor, RCN Acknowledgement: FON TeamDocument51 pagesIntroduction To Nursing Process (NP) : Presenter:M.Salman Alam Nursing Instructor, RCN Acknowledgement: FON TeamSaqlain M.No ratings yet
- Community AssessmentDocument3 pagesCommunity AssessmentMariah Jane TaladuaNo ratings yet
- NCM 101Document8 pagesNCM 101Anna LaritaNo ratings yet
- NURSING PROCESS FundaDocument26 pagesNURSING PROCESS FundaDELA CRUZ, JENISSE LOUISSENo ratings yet
- Community E ToolDocument5 pagesCommunity E ToolLi mNo ratings yet
- Nursing Process: Nursing Diagnosis: By: Hosnu InayatiDocument10 pagesNursing Process: Nursing Diagnosis: By: Hosnu Inayatihosnu inayatiNo ratings yet
- What Factors Influence Ward Nurses' Recognition of andDocument18 pagesWhat Factors Influence Ward Nurses' Recognition of andPAULA SORAIA CHENNo ratings yet
- Nuph 1-6Document83 pagesNuph 1-6uthayaNo ratings yet
- NRS110 Lecture 1 Care Plan WorkshopDocument14 pagesNRS110 Lecture 1 Care Plan WorkshopsamehNo ratings yet
- M3. Nursing DiagnosisDocument18 pagesM3. Nursing DiagnosisRezalNo ratings yet
- Nursing DiagnosisDocument48 pagesNursing DiagnosisLydia Lopz MsnrncdNo ratings yet
- NCS UpdatedDocument8 pagesNCS UpdatedwalaNo ratings yet
- Learning Objektif IRK Definisi Diagnosa: American Nursing Assosiation/ANA)Document8 pagesLearning Objektif IRK Definisi Diagnosa: American Nursing Assosiation/ANA)yusufNo ratings yet
- Nursing Process EBN Format OB PEDIADocument5 pagesNursing Process EBN Format OB PEDIAChezka Orton Swift BolintiamNo ratings yet
- 2023 Spring - NURS 252-St Data SheetDocument7 pages2023 Spring - NURS 252-St Data SheetmalakajameahNo ratings yet
- Nursing Process EBN Format OB PEDIADocument5 pagesNursing Process EBN Format OB PEDIAAnn Nicole UlitNo ratings yet
- FundaDocument41 pagesFundashawdino03No ratings yet
- Case Study Guidelines Grand CaseDocument12 pagesCase Study Guidelines Grand CaseCLARISSE CLOIE LAMBERTENo ratings yet
- Case Study FormatDocument9 pagesCase Study FormatALIZA BAKILNo ratings yet
- Evidence Based Medicine: Hadi Sarosa Bagian Ilmu Faal F.K Unissula SemarangDocument61 pagesEvidence Based Medicine: Hadi Sarosa Bagian Ilmu Faal F.K Unissula SemarangLydia Hapsari SudjonoNo ratings yet
- 1 Nursing ProcessDocument30 pages1 Nursing ProcessCrystal Ann TadiamonNo ratings yet
- Data Interpretation and AnalysisDocument37 pagesData Interpretation and AnalysistdisnahNo ratings yet
- Nursing Process QuestionsDocument12 pagesNursing Process QuestionsSritama Ghosh100% (1)
- Manuscriptm1 203 Grp26 12gDocument61 pagesManuscriptm1 203 Grp26 12gRuthangela GarciaNo ratings yet
- Unit 1 (Introduction To Health Assessment Concepts) - ConverteDocument28 pagesUnit 1 (Introduction To Health Assessment Concepts) - ConverteUmme HabibaNo ratings yet
- NandaDocument28 pagesNandaसपना दाहालNo ratings yet
- N 10 Diagnosing and Planning 2016Document40 pagesN 10 Diagnosing and Planning 2016Immanuel Cris PalasigueNo ratings yet
- Health AssessmentDocument15 pagesHealth AssessmentmeghanaNo ratings yet
- Nursing AssesmentDocument38 pagesNursing AssesmentbbpanickerNo ratings yet
- CHN in House Module 2Document4 pagesCHN in House Module 2Catherine AteradoNo ratings yet
- Health Assessment AssignmentDocument15 pagesHealth Assessment Assignmentpslokesha84No ratings yet
- The Nursing ProcessDocument24 pagesThe Nursing ProcessVea SantiagoNo ratings yet
- Nursing Case Study FormatDocument8 pagesNursing Case Study Formatm74303010No ratings yet
- Nurses Role in Health AssessmentDocument5 pagesNurses Role in Health AssessmentKimberly Jane TogñoNo ratings yet
- Notes (Health Assessment)Document23 pagesNotes (Health Assessment)Sheena Español0% (1)
- Foundations Study Guide FINAL EXAMDocument15 pagesFoundations Study Guide FINAL EXAMigorot89100% (1)
- PDR 978543Document7 pagesPDR 978543Faiz HassanNo ratings yet
- Module 4Document13 pagesModule 4gennemayguzman2004No ratings yet
- Week 1.1Document65 pagesWeek 1.1ginny.mycookiecanNo ratings yet
- Does Nursing Science Exist? A View From SeattleDocument42 pagesDoes Nursing Science Exist? A View From SeattleSri EndriyaniNo ratings yet
- NCP Opst Fdar 2 1 1 1 1Document4 pagesNCP Opst Fdar 2 1 1 1 1dsmagallanesNo ratings yet
- 0 Health Assessment HEENTDocument110 pages0 Health Assessment HEENTSamNo ratings yet
- Research Paper On Withholding The Truth From Dying PatientsDocument6 pagesResearch Paper On Withholding The Truth From Dying PatientsTEHKHUM SULTANALINo ratings yet
- The Five Overlapping Phases of The Nursing Process: AssessingDocument27 pagesThe Five Overlapping Phases of The Nursing Process: AssessingFahad AlmalkiNo ratings yet
- Name: Indriyani Eka Lani Oematan Nim:01.2.17.00609 English Courses ResumeDocument3 pagesName: Indriyani Eka Lani Oematan Nim:01.2.17.00609 English Courses ResumeEka OematanNo ratings yet
- Biostatistician - The Comprehensive Guide: Vanguard ProfessionalsFrom EverandBiostatistician - The Comprehensive Guide: Vanguard ProfessionalsNo ratings yet
- Case 1: Group 4Document26 pagesCase 1: Group 4John Joshua Lacson MedicineNo ratings yet
- Pre-Test Mapeh 6Document5 pagesPre-Test Mapeh 6RANDY ALVARONo ratings yet
- Prognosis and Outcomes Following Sudden Cardiac Arrest in AdultsDocument24 pagesPrognosis and Outcomes Following Sudden Cardiac Arrest in AdultsAnca StanNo ratings yet
- Universiti Teknologi Mara (Uitm) Puncak Alam Campus Faculty of Health SciencesDocument7 pagesUniversiti Teknologi Mara (Uitm) Puncak Alam Campus Faculty of Health SciencesMOHD MU'IZZ BIN MOHD SHUKRINo ratings yet
- Midterm 1 StudentsDocument9 pagesMidterm 1 Studentswangbusila1No ratings yet
- NU 665 Pediatric Gastrointestinal Case Study - Michelle - StewardDocument10 pagesNU 665 Pediatric Gastrointestinal Case Study - Michelle - StewardMichelle StewardNo ratings yet
- 5.2.2 Drug Therapeutic RecordDocument2 pages5.2.2 Drug Therapeutic Recordjoyrena ochondraNo ratings yet
- Homework: 1) What Does The Respiratory System Do ?Document6 pagesHomework: 1) What Does The Respiratory System Do ?Mariana VasileNo ratings yet
- MM Scope EvolutionDocument53 pagesMM Scope EvolutionSai RevanthNo ratings yet
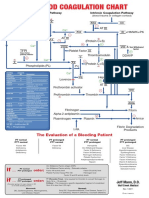
- Blood Clotting ChartDocument1 pageBlood Clotting ChartBianca SimionescuNo ratings yet
- Late Cytomegalovirus (CMV) Infections After Kidney Transplantation Under The Preemptive Strategy: Risk Factors and Clinical AspectsDocument8 pagesLate Cytomegalovirus (CMV) Infections After Kidney Transplantation Under The Preemptive Strategy: Risk Factors and Clinical AspectsQiuju LuNo ratings yet
- Name of Drug Dosage/Frequency/ Timing/Route Mechanism of Action Indication Contraindication Adverse Effect Nursing ResponsibilitiesDocument2 pagesName of Drug Dosage/Frequency/ Timing/Route Mechanism of Action Indication Contraindication Adverse Effect Nursing ResponsibilitieskyleNo ratings yet
- SleepDocument4 pagesSleepBekir Can ÇelikNo ratings yet
- Introduction To Special Education: Taylor-White Elementary SchoolDocument23 pagesIntroduction To Special Education: Taylor-White Elementary SchoolEric D. ValleNo ratings yet
- Case Digest 2Document23 pagesCase Digest 2boks9s.9escaladaNo ratings yet
- Q2-W4-D1 & D2Document6 pagesQ2-W4-D1 & D2LYDIANo ratings yet
- Prevention of Infection After Gynecologic Procedures ACOG 2018Document18 pagesPrevention of Infection After Gynecologic Procedures ACOG 2018Luisa MorenoNo ratings yet
- Auditory DisordersDocument19 pagesAuditory DisordersJobelle AcenaNo ratings yet
- Nishi Gupta - Santosh G. Honavar - Rhino-Orbito-Cerebral Mucormycosis-Springer (2022)Document305 pagesNishi Gupta - Santosh G. Honavar - Rhino-Orbito-Cerebral Mucormycosis-Springer (2022)Khanh Ha NguyenNo ratings yet
- Institutioning Public HealthDocument3 pagesInstitutioning Public HealthAhmed AbbasNo ratings yet
- Problems Associated With Chronic IllnessDocument8 pagesProblems Associated With Chronic IllnessMeryville JacildoNo ratings yet
- Anestesia e Esclerose TuberosaDocument5 pagesAnestesia e Esclerose TuberosaMarina MelekNo ratings yet
- Ayurvedic Nail Analysis: What Do Your Nails Say About Your HealthDocument14 pagesAyurvedic Nail Analysis: What Do Your Nails Say About Your Healthsirrichard1No ratings yet
- 10 1016@j Bpobgyn 2015 11 014Document17 pages10 1016@j Bpobgyn 2015 11 014Marco Julcamoro AsencioNo ratings yet
- Unit 7 Lesson 1 AnglaisDocument6 pagesUnit 7 Lesson 1 AnglaisMoussa FofanaNo ratings yet
- Continuing Education Activity: ObjectivesDocument3 pagesContinuing Education Activity: ObjectivesAnthony LopezNo ratings yet
- Food Safety Module - WorkbookDocument51 pagesFood Safety Module - WorkbookHerman SmitNo ratings yet
- Water Fogging and Misting Systems - Are They A Risk To Human Health?Document2 pagesWater Fogging and Misting Systems - Are They A Risk To Human Health?Rodger OlynNo ratings yet
- PATHOPHYSIOLOGYDocument4 pagesPATHOPHYSIOLOGYJasonlee BaluyotNo ratings yet