Download as pdf or txt
You might also like
- Health Assessment NotesDocument40 pagesHealth Assessment NotesShane Tamil100% (8)
- Psychiatric History and ExaminationDocument14 pagesPsychiatric History and ExaminationPaolo Bonifacio100% (15)
- Buddhist Peaceful Means On Conflict Management PDFDocument410 pagesBuddhist Peaceful Means On Conflict Management PDFKarbono AdisanaNo ratings yet
- MY MAXICARE (Brochure) PDFDocument16 pagesMY MAXICARE (Brochure) PDFFeedLab CARNo ratings yet
- BTB Template Er-IntakeDocument3 pagesBTB Template Er-IntakeBoy MadNo ratings yet
- Things To Consider During Patient InterviewDocument2 pagesThings To Consider During Patient InterviewJeffrey Viernes100% (1)
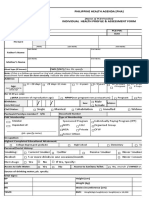
- PHA Individual Health Profile & Assessment Form As of Oct.09, 2017Document8 pagesPHA Individual Health Profile & Assessment Form As of Oct.09, 2017Eden VblagasyNo ratings yet
- Week 1: Item PointsDocument112 pagesWeek 1: Item PointsAngel Lynn YlayaNo ratings yet
- Care Plan Worksheet Mental Health 2022Document3 pagesCare Plan Worksheet Mental Health 2022tahani.mah147No ratings yet
- History Taking FormatDocument10 pagesHistory Taking FormatMuskaan Deep100% (1)
- Comprehensive Health Assessment of The Older Person in Health and Aged CareDocument24 pagesComprehensive Health Assessment of The Older Person in Health and Aged Carenavdeep1133No ratings yet
- Afdal Shamsa w1 Ncm116rleDocument36 pagesAfdal Shamsa w1 Ncm116rleShamsa AfdalNo ratings yet
- Taking A HXDocument2 pagesTaking A HXBuNo ratings yet
- Intake GuideDocument2 pagesIntake GuideronarudoNo ratings yet
- Concept Map #1Document10 pagesConcept Map #1peteNo ratings yet
- Care Plan Format MSNDocument8 pagesCare Plan Format MSNLijoNo ratings yet
- Patient Inclusive Treatment PlanDocument3 pagesPatient Inclusive Treatment Planapi-632710984No ratings yet
- Abdominal Pain With Uterine CrampsDocument8 pagesAbdominal Pain With Uterine CrampsMohamadhizam M. PangcatanNo ratings yet
- Ontario Perinatal Record 2017Document5 pagesOntario Perinatal Record 2017Own VolitionNo ratings yet
- Unfolding Reasoning Dementia Physical AggressionDocument7 pagesUnfolding Reasoning Dementia Physical AggressionnoslendadnarimNo ratings yet
- Behavioral Health Care PlanDocument11 pagesBehavioral Health Care Planapi-520930030No ratings yet
- ICA C 183Document9 pagesICA C 183peachypeachyNo ratings yet
- Cochise Tail Oa Group ProjectDocument13 pagesCochise Tail Oa Group Projectapi-644444841No ratings yet
- Rle CompreDocument132 pagesRle CompremayangernszNo ratings yet
- CSC Proforma - GeneralDocument6 pagesCSC Proforma - General127 Shruthik Patel ThotaNo ratings yet
- Subjective Data Objective Data: Alert Oriented Level of Comprehension Concentration MemoryDocument3 pagesSubjective Data Objective Data: Alert Oriented Level of Comprehension Concentration MemoryclrssNo ratings yet
- MS3 Survival Kit Jan 2012Document22 pagesMS3 Survival Kit Jan 2012Antony Awad100% (1)
- Nursing Care PlanDocument16 pagesNursing Care PlanMelody B. MiguelNo ratings yet
- Resume, Ect, Foll-Up, Kascil, KasbesDocument27 pagesResume, Ect, Foll-Up, Kascil, KasbesHana Nury RahmawatiNo ratings yet
- Chavez TinocomDocument13 pagesChavez Tinocomapi-641827342No ratings yet
- Appendix A - FDocument54 pagesAppendix A - Fbakson college gr. noidaNo ratings yet
- Appendix I: Case FormatDocument9 pagesAppendix I: Case FormatDrAyushi Aggarwal AshiNo ratings yet
- Medical Admission Proforma: Hospital Name Patient DetailsDocument11 pagesMedical Admission Proforma: Hospital Name Patient DetailsAngelus129No ratings yet
- Laboratory Notes 1Document8 pagesLaboratory Notes 1thenalynnloyolaNo ratings yet
- Laguna State Polytechnic University: Republic of The PhilippinesDocument4 pagesLaguna State Polytechnic University: Republic of The PhilippinesAbigael Patricia GutierrezNo ratings yet
- Winter+AoBP+2 2+SMDocument16 pagesWinter+AoBP+2 2+SMJuan Carlos LopezNo ratings yet
- Pa Tool MihpDocument23 pagesPa Tool MihpNassif M. BangcolaNo ratings yet
- History Taking PDFDocument2 pagesHistory Taking PDFaliNo ratings yet
- Short Case Sheet FormDocument3 pagesShort Case Sheet Formrakesh kumarNo ratings yet
- Gedi Body EssentialsDocument71 pagesGedi Body EssentialssenilecornNo ratings yet
- Gedi - Body 1-71Document71 pagesGedi - Body 1-71Ahmed Abdurahman100% (2)
- BLANK Nursing Process PaperDocument10 pagesBLANK Nursing Process PaperSNOOKI513No ratings yet
- PD OSCE GuideDocument19 pagesPD OSCE GuideChorong ParkNo ratings yet
- Garbhini Case PDFDocument5 pagesGarbhini Case PDFBhavya ParmarNo ratings yet
- Sbar 01Document1 pageSbar 01emip100% (2)
- BTB Template Er-IntakeDocument3 pagesBTB Template Er-IntakehectorNo ratings yet
- I. Vital Information: W La Paz, Iloilo CityDocument7 pagesI. Vital Information: W La Paz, Iloilo CityelleNo ratings yet
- NCP, InterviewDocument8 pagesNCP, Interviewim. EliasNo ratings yet
- CASE REPORT-SampleDocument7 pagesCASE REPORT-SampleMuhammad BilalNo ratings yet
- Pediatric History and PE - Dr. LeonesDocument4 pagesPediatric History and PE - Dr. LeonesmedicoNo ratings yet
- General HistoryDocument16 pagesGeneral HistoryjjNo ratings yet
- NCPDocument16 pagesNCPmmlktiNo ratings yet
- Intake Interview FormDocument4 pagesIntake Interview Formrakhee mehtaNo ratings yet
- NR 446 Clinical Packet w8Document10 pagesNR 446 Clinical Packet w8kaurhappy819No ratings yet
- Final Nursing Care PlanDocument12 pagesFinal Nursing Care PlanBerina SelimovicNo ratings yet
- Libro ComplementarioDocument155 pagesLibro ComplementarioKowe xDNo ratings yet
- Patient's Name: Past Medical History: (Cephalocaudal)Document1 pagePatient's Name: Past Medical History: (Cephalocaudal)Strygwyr BloodseekerNo ratings yet
- CONTENTS OF THE RLE WRITTEN REQUIREMENTSDocument8 pagesCONTENTS OF THE RLE WRITTEN REQUIREMENTSGwenn SalazarNo ratings yet
- 229 Thotakura Eknath, Im, 16 Nov 2021, Case 83 - Day 1Document21 pages229 Thotakura Eknath, Im, 16 Nov 2021, Case 83 - Day 1EK NathNo ratings yet
- Contents of The Rle Written RequirementsDocument7 pagesContents of The Rle Written RequirementsElla RetizaNo ratings yet
- Guide to Intellectual Disabilities: A Clinical HandbookFrom EverandGuide to Intellectual Disabilities: A Clinical HandbookJulie P. GentileNo ratings yet
- Odysseus' Labours: A Rehabilitation and Recovery Guide for Those Who Have a Mental Illness and Their CarersFrom EverandOdysseus' Labours: A Rehabilitation and Recovery Guide for Those Who Have a Mental Illness and Their CarersNo ratings yet
- Daily Regimen Ant TB TreatmentDocument37 pagesDaily Regimen Ant TB TreatmentVidya Mohan KrithikanandNo ratings yet
- Indirect Calorimetry in Critical Illness A New.3Document10 pagesIndirect Calorimetry in Critical Illness A New.3gjk5q24qrqNo ratings yet
- CDC Mask MandateDocument3 pagesCDC Mask MandateFOX 17 NewsNo ratings yet
- Jover JC PEGfilgrastimDocument7 pagesJover JC PEGfilgrastimCheli GarciaNo ratings yet
- Nimotuzumab A Novel anti-EGFR Monoclonal PDFDocument8 pagesNimotuzumab A Novel anti-EGFR Monoclonal PDFAkbar SuuryoNo ratings yet
- CC Lab ActDocument3 pagesCC Lab ActTrisha IbarraNo ratings yet
- THT 4Document7 pagesTHT 4michelleruthnNo ratings yet
- Meehleib, Rachelle Ayn S. Pepino, Stephanie Kate ADocument16 pagesMeehleib, Rachelle Ayn S. Pepino, Stephanie Kate ARachelle AynNo ratings yet
- MDI 2019 Streszczenia AbstractsDocument254 pagesMDI 2019 Streszczenia AbstractsShruti GehlotNo ratings yet
- Liceo de Cagayan University College of Nursing: ST ND RDDocument3 pagesLiceo de Cagayan University College of Nursing: ST ND RDPAUL MICHAEL G. BAGUHINNo ratings yet
- Making Better Use of Pharmacy: Chair: Donal Markey, Head of Primary Care Commissioning, NHS England (London Region)Document45 pagesMaking Better Use of Pharmacy: Chair: Donal Markey, Head of Primary Care Commissioning, NHS England (London Region)Noor AliNo ratings yet
- FNCP 1 - DiabetesDocument3 pagesFNCP 1 - DiabetesBianca Joy GonzalesNo ratings yet
- 2 Pharma ModuleDocument227 pages2 Pharma ModuleCielina BatangNo ratings yet
- PRC Vs de GuzmanDocument14 pagesPRC Vs de GuzmanSamFerrerNo ratings yet
- Tugas Bahasa InggrisDocument3 pagesTugas Bahasa Inggrisenaf fantiahNo ratings yet
- Daftar Pustaka BioklinDocument4 pagesDaftar Pustaka BioklinRichoco SapoetraNo ratings yet
- 1 - MCCDDocument26 pages1 - MCCDAnupam SarkarNo ratings yet
- 4 Intraoperative PhaseDocument12 pages4 Intraoperative PhaseDarlyn AmplayoNo ratings yet
- Maxillary Sinus Augmentation: Tarun Kumar A.B, Ullas AnandDocument13 pagesMaxillary Sinus Augmentation: Tarun Kumar A.B, Ullas Anandyuan.nisaratNo ratings yet
- FAME Prioritizing Mental Health Residential Facilities For COVID VaccineDocument2 pagesFAME Prioritizing Mental Health Residential Facilities For COVID VaccineWCTV Digital TeamNo ratings yet
- Class Presentation ON Acute Tubular NecrosisDocument39 pagesClass Presentation ON Acute Tubular NecrosisDeeksha RajputNo ratings yet
- Youth and Yoga PDFDocument472 pagesYouth and Yoga PDFAleksandra Ristic0% (1)
- Rheumatology Diseases Group CDocument73 pagesRheumatology Diseases Group CDiana NurulNo ratings yet
- RugiDocument6 pagesRugiLisa PutriNo ratings yet
- How To Maintain Eye HealthDocument2 pagesHow To Maintain Eye HealthFani PranidasariNo ratings yet
- Tran-Eportfolio Cover LetterDocument1 pageTran-Eportfolio Cover Letterapi-335042704No ratings yet
- Executive13 Order BhertDocument2 pagesExecutive13 Order Bhertchelle100% (1)
- Final NCP AppendicitisDocument4 pagesFinal NCP AppendicitisCha Ry100% (1)