Download as pdf or txt
You might also like
- Pharmacy Calculation Workbook: 250 Questions to Prepare for the NAPLEX and PTCB ExamFrom EverandPharmacy Calculation Workbook: 250 Questions to Prepare for the NAPLEX and PTCB ExamRating: 5 out of 5 stars5/5 (2)
- Critical Care Intravenous Medications ChartDocument2 pagesCritical Care Intravenous Medications ChartMichelle Danielle MolinaNo ratings yet
- ACLS Pocket GuideDocument5 pagesACLS Pocket Guidedragnu100% (1)
- Pediatric Surgery HandbookDocument75 pagesPediatric Surgery HandbookAlex Vătau100% (2)
- Teicoplanin Dosing and Monitoring in AdultsDocument3 pagesTeicoplanin Dosing and Monitoring in Adultsdps_1976No ratings yet
- Guideline: Antibiotic Drug Monitoring: Aminoglycosides and GlycopeptidesDocument8 pagesGuideline: Antibiotic Drug Monitoring: Aminoglycosides and GlycopeptidesKenRodulfReyesVillaruelNo ratings yet
- NICU Drugs GuideDocument49 pagesNICU Drugs GuideArhanNo ratings yet
- Enoxaparin Info SheetDocument7 pagesEnoxaparin Info SheetjafarkassimNo ratings yet
- vanco-2015Document1 pagevanco-2015babyblueoutNo ratings yet
- Notes in Neonates محمد ابراهيم مستشفى قوص قنا.WhiteKnightLoveDocument77 pagesNotes in Neonates محمد ابراهيم مستشفى قوص قنا.WhiteKnightLoveMaRwa IbrahimNo ratings yet
- TroughDocument1 pageTroughlalirmkNo ratings yet
- Recommended Doses of Medications To Treat Children With An Acute Asthma ExacerbaDocument3 pagesRecommended Doses of Medications To Treat Children With An Acute Asthma Exacerbaمعاذ الشريفNo ratings yet
- TDM Practical Guide Part1Document7 pagesTDM Practical Guide Part1Ahmedshaker21100% (1)
- Teicoplanin Prescribing and Therapeutic Drug Monitoring Clinical Guideline V2.0 March 2019Document12 pagesTeicoplanin Prescribing and Therapeutic Drug Monitoring Clinical Guideline V2.0 March 2019nancy voraNo ratings yet
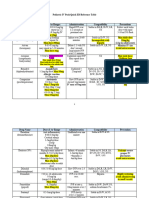
- Guide For Drug Level Monitoring of Commonly Used MedicationsDocument4 pagesGuide For Drug Level Monitoring of Commonly Used MedicationsMohamed HussienNo ratings yet
- Cisplatin-Pemetrexed (NSCLC)Document5 pagesCisplatin-Pemetrexed (NSCLC)Sindu SankarNo ratings yet
- Am Iog Lyco SidesDocument2 pagesAm Iog Lyco Sidesthemega1111No ratings yet
- IV Push List PedsDocument5 pagesIV Push List PedskrizzywhizzyNo ratings yet
- Phenytoin Administration GuideDocument2 pagesPhenytoin Administration GuideNoorHaziqZ1926No ratings yet
- ÷ Weight (KG) Dilute 1 ML (500mcg) of PGE1 With NS/ D5% To Yield The Total Volume From #1Document14 pages÷ Weight (KG) Dilute 1 ML (500mcg) of PGE1 With NS/ D5% To Yield The Total Volume From #1Nesreen G MohammedNo ratings yet
- Tuberculosis Treatment GuidelinesDocument2 pagesTuberculosis Treatment GuidelinesMaverick CaoileNo ratings yet
- Vancomicin Guidelines PICUDocument2 pagesVancomicin Guidelines PICUAnonymous 6iwMFwNo ratings yet
- Kadcyla Trastuzumab Emtansine HER-2 Positive Breast CancerDocument11 pagesKadcyla Trastuzumab Emtansine HER-2 Positive Breast CancersmokkerNo ratings yet
- Lampiran OM & FaringitisDocument6 pagesLampiran OM & FaringitisAdhinyDistiHelmiNo ratings yet
- Huitm Paediatrics Antimicrobial Dosing GuideDocument6 pagesHuitm Paediatrics Antimicrobial Dosing Guidedrnurulhikmah.kkiatuaranNo ratings yet
- Anusha Inotropes 21Document62 pagesAnusha Inotropes 21twister4No ratings yet
- App4 DrugLevelsDocument2 pagesApp4 DrugLevelsDr. DukeNo ratings yet
- Medad TeamDocument18 pagesMedad TeamAxmed MaxamedNo ratings yet
- Medication Administration PolicyDocument76 pagesMedication Administration PolicyJully GaciasNo ratings yet
- Versed (Midazolam) Dosing, Indications, Interactions, Adverse Effects, and MoreDocument2 pagesVersed (Midazolam) Dosing, Indications, Interactions, Adverse Effects, and MoreRiski DohartuaNo ratings yet
- Drug Therapy For PicuDocument32 pagesDrug Therapy For PicuNeethu Mariya MathewNo ratings yet
- Symptom Management Obstruksi BowelDocument5 pagesSymptom Management Obstruksi BowelPutri Mega PetasiNo ratings yet
- EC-DH Epirubicin Cyclophosphamide Followed by Docetaxel With Trastuzumab Protocol V1.1Document11 pagesEC-DH Epirubicin Cyclophosphamide Followed by Docetaxel With Trastuzumab Protocol V1.1smokkerNo ratings yet
- FentanylDocument1 pageFentanyldoctormussieaberraNo ratings yet
- Drug: Milrinone Presentation: Action & Indication:: 30 WeeksDocument1 pageDrug: Milrinone Presentation: Action & Indication:: 30 WeeksSIDHARTH GOYALNo ratings yet
- Infusions 1Document4 pagesInfusions 1Mohammed IbrahimNo ratings yet
- TDMGUIDEDocument1 pageTDMGUIDEJoanna MarieNo ratings yet
- Fukkm 1 2020 PDFDocument346 pagesFukkm 1 2020 PDFIan ChoongNo ratings yet
- Pain Pocket GuideDocument2 pagesPain Pocket Guidebtalera100% (2)
- Morphine Titration GuideDocument1 pageMorphine Titration GuideDaniel Jonathan LimNo ratings yet
- Castration-Recurrent Prostate Cancer First-Line Therapy: No Visceral MetastasesDocument2 pagesCastration-Recurrent Prostate Cancer First-Line Therapy: No Visceral Metastasesalberto cabelloNo ratings yet
- Aminoglycoside & VancomycinDocument10 pagesAminoglycoside & VancomycinKhor Chin PooNo ratings yet
- Cardiology Doses: WhiteknightloveDocument3 pagesCardiology Doses: WhiteknightloveSelim TarekNo ratings yet
- PICU Drug Boluses: Drug Dose /KG Range Administration NotesDocument5 pagesPICU Drug Boluses: Drug Dose /KG Range Administration NotesMaria BudnicNo ratings yet
- Midazolam (RX) : Dosing & UsesDocument4 pagesMidazolam (RX) : Dosing & Usesintrovert ikonNo ratings yet
- PICU Drug Infusions: Drug Add To 50ml Notes Dose Range 1ml/hrDocument2 pagesPICU Drug Infusions: Drug Add To 50ml Notes Dose Range 1ml/hrNeethu Mariya MathewNo ratings yet
- Paediatricshouseofficerguidehospitalkulim 151026150042 Lva1 App6891Document14 pagesPaediatricshouseofficerguidehospitalkulim 151026150042 Lva1 App6891Nadia SalwaniNo ratings yet
- Disaster Lecture MidtermsDocument8 pagesDisaster Lecture MidtermsMae Arra Lecobu-anNo ratings yet
- AmiDocument4 pagesAmipurushothama reddyNo ratings yet
- Medication Conversion ChartDocument2 pagesMedication Conversion ChartIlinca mirnoviciNo ratings yet
- BendamustineDocument2 pagesBendamustineagusjatNo ratings yet
- Guidelines For Nurse Controlled and Patient Controlled Analgesia Morphine InfusionDocument2 pagesGuidelines For Nurse Controlled and Patient Controlled Analgesia Morphine Infusionfinchan IrawanNo ratings yet
- Brentuximab-Vedotin NHS RegimenDocument6 pagesBrentuximab-Vedotin NHS RegimenLuana MNo ratings yet
- Kitty MagicDocument3 pagesKitty MagicIordana StoicaNo ratings yet
- Vancomycin IV IntermittentDocument2 pagesVancomycin IV Intermittentsereyvatanasao19No ratings yet
- 2013 Vancomycin Do Sing GuideDocument1 page2013 Vancomycin Do Sing GuideaLPHA1No ratings yet
- Pediatric IV Push Quick ED Reference TableDocument4 pagesPediatric IV Push Quick ED Reference TableTayyab RazaNo ratings yet
- Critical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsNo ratings yet
- Dimensional Analysis For Nursing StudentsFrom EverandDimensional Analysis For Nursing StudentsNo ratings yet
- Nag2019 PDFDocument288 pagesNag2019 PDFmashupNo ratings yet
- Avance de Trabajo Final InglesDocument5 pagesAvance de Trabajo Final InglesAri CaldNo ratings yet
- Acidosis Alkalosis BiochemistryDocument28 pagesAcidosis Alkalosis BiochemistryDocSam048No ratings yet
- Anthrax Attacks 1210348955921185 9Document21 pagesAnthrax Attacks 1210348955921185 9adhikaNo ratings yet
- Malaria Prevention Practices and Associated Factors Among Households of Hawassa City Administration, Southern Ethiopia, 2020Document12 pagesMalaria Prevention Practices and Associated Factors Among Households of Hawassa City Administration, Southern Ethiopia, 2020yowan wandikboNo ratings yet
- Lower Respiratory Tract InfectionDocument21 pagesLower Respiratory Tract InfectionJohn Vincent Dy OcampoNo ratings yet
- Pathlab PDFDocument22 pagesPathlab PDFNicole HoNo ratings yet
- IATF Resolution No. 118-ADocument7 pagesIATF Resolution No. 118-AMetroStaycationNo ratings yet
- Vsim - Edited Clinical WorksheetsDocument8 pagesVsim - Edited Clinical WorksheetsTedra FloydNo ratings yet
- Nutritional Terms: Nama: Rini Suvia Nababan Prodi: D-III Sem-IIDocument2 pagesNutritional Terms: Nama: Rini Suvia Nababan Prodi: D-III Sem-IIRini Suvia NababanNo ratings yet
- Food Allergomics Based On High-Throughput and Bioinformatics TechnologiesDocument10 pagesFood Allergomics Based On High-Throughput and Bioinformatics TechnologiesGus PolentaNo ratings yet
- Sales Invoice: Graha Megatama Indonesia, PTDocument1 pageSales Invoice: Graha Megatama Indonesia, PTPaul Wendy DasilvaNo ratings yet
- Psychiatric Nursing Bullets Neurotransmission TheoryDocument4 pagesPsychiatric Nursing Bullets Neurotransmission TheoryDefensor Pison Gringgo100% (1)
- CashewDocument18 pagesCashewAloy Dela CruzNo ratings yet
- Principles of MicrobiologyDocument301 pagesPrinciples of MicrobiologyBenjamin A. Ujlaki76% (17)
- Case Analysis PaperDocument2 pagesCase Analysis PaperKukugirl DavisNo ratings yet
- Ipmat Indore 2021 PaperDocument8 pagesIpmat Indore 2021 PaperdivyanshjoshidpsjkpNo ratings yet
- Esoteric HealingDocument12 pagesEsoteric HealingWitchtopia Realm100% (5)
- Prognosis of Permanent Teeth With Internal Resorption - A Clinical ReviewDocument8 pagesPrognosis of Permanent Teeth With Internal Resorption - A Clinical ReviewFlorin IonescuNo ratings yet
- Mosquitoes: Amal Almuhanna 2012Document54 pagesMosquitoes: Amal Almuhanna 2012Stefani A rachmaNo ratings yet
- Diet Readiness QuestionnaireDocument3 pagesDiet Readiness Questionnairesavvy_as_98100% (1)
- Aimee M. Abide, Catherine Margaret Kuza, Michael T. Vest - Self-Assessment in Adult Multiprofessional Critical Care (2022, Society of Critical Care Medicine) - Libgen - Li 2Document360 pagesAimee M. Abide, Catherine Margaret Kuza, Michael T. Vest - Self-Assessment in Adult Multiprofessional Critical Care (2022, Society of Critical Care Medicine) - Libgen - Li 2Gibran HolmesNo ratings yet
- Bio01 Co2 PPT - Cell CycleDocument120 pagesBio01 Co2 PPT - Cell CycleMarc Ronald de LeonNo ratings yet
- Immunohistochemical Characterization of Urethral Polyps in WomenDocument4 pagesImmunohistochemical Characterization of Urethral Polyps in WomenCentral Asian StudiesNo ratings yet
- Communicable and Non-Communicable DiseaseDocument44 pagesCommunicable and Non-Communicable DiseaseSajida Bibi NoonariNo ratings yet
- 11 cсынып емтихан сурактарыDocument6 pages11 cсынып емтихан сурактарыakzharNo ratings yet
- Reishi MushroomDocument5 pagesReishi Mushroomjunver100% (4)
- Stress: and The IndividualDocument9 pagesStress: and The Individualsamon sumulongNo ratings yet
- Divine Light (Akhand Jyoti)Document48 pagesDivine Light (Akhand Jyoti)sksuman100% (13)