
Leishman Register_A3
Leishman Register_A3
You might also like
- List of Pharmaceutical Companies in Ahmedabad WithDocument22 pagesList of Pharmaceutical Companies in Ahmedabad Withsandipsc88% (8)
- Pidsr CifDocument17 pagesPidsr CifAbraham Asto100% (4)
- Soap NoteDocument2 pagesSoap Notetopopirate100% (4)
- Chapter 1 - Introduction To The Food and Beverage IndustryDocument64 pagesChapter 1 - Introduction To The Food and Beverage IndustryPn Firdaus92% (12)
- Laboratory Request FormDocument1 pageLaboratory Request FormEric Nagum100% (2)
- Best 25 Question and Answer For Boiler First and Second Class Operator Viva Examination 2017 - ASKPOWERPLANTDocument32 pagesBest 25 Question and Answer For Boiler First and Second Class Operator Viva Examination 2017 - ASKPOWERPLANTRaju Maity100% (5)
- CASESHEETPHARMDDocument6 pagesCASESHEETPHARMDSai SharathNo ratings yet
- Examination and Result Management System - TutorialsDuniya PDFDocument56 pagesExamination and Result Management System - TutorialsDuniya PDFAishwaryaNo ratings yet
- Instructions For Leishmanises Register: Day / Month / Year (DD/MM/YY) (EC)Document2 pagesInstructions For Leishmanises Register: Day / Month / Year (DD/MM/YY) (EC)Dagnachew MulugetaNo ratings yet
- MOH 405 ANC Register 1Document4 pagesMOH 405 ANC Register 1S DonoughNo ratings yet
- DR TB REGISTER A3 SizeDocument5 pagesDR TB REGISTER A3 Sizeabdullee354No ratings yet
- PNC - A3-1Document5 pagesPNC - A3-1dabashgetNo ratings yet
- Health Center/Clinic/Hospital: Out Patient Department (OPD) RegisterDocument4 pagesHealth Center/Clinic/Hospital: Out Patient Department (OPD) RegisterGetu Tadele100% (2)
- DR Follow up registration_A3Document5 pagesDR Follow up registration_A3abdullee354No ratings yet
- 3.anc A3Document3 pages3.anc A3dabashgetNo ratings yet
- HSTP II HMIS Hospital Heath Centre and Health PostDocument367 pagesHSTP II HMIS Hospital Heath Centre and Health PostDagmawitNo ratings yet
- Unit TB Register A3Document6 pagesUnit TB Register A3abdullee354No ratings yet
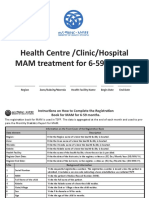
- Health Centre /Clinic/Hospital MAM Treatment For 6-59 MonthsDocument3 pagesHealth Centre /Clinic/Hospital MAM Treatment For 6-59 MonthsAmenti FiromsaNo ratings yet
- CERTIFICATE OF HEALTH (To Be Filled Out by A Physician) - Page 1Document2 pagesCERTIFICATE OF HEALTH (To Be Filled Out by A Physician) - Page 1gnzbdbNo ratings yet
- Health Centre /Clinic/Hospital Family Planning RegisterDocument4 pagesHealth Centre /Clinic/Hospital Family Planning RegisterAnuka YituNo ratings yet
- Form 6a. Drug Susceptible TB RegisterDocument4 pagesForm 6a. Drug Susceptible TB RegisterAllen ChesterNo ratings yet
- Health DeclarationDocument5 pagesHealth Declarationust dol100% (1)
- Health Declaration and Medical Examination Form: Scholarship DivisionDocument5 pagesHealth Declaration and Medical Examination Form: Scholarship Divisionnazrin sarajuddinNo ratings yet
- Clinical Case Study Guideline and TemplateDocument19 pagesClinical Case Study Guideline and TemplateMikhaela Andree MarianoNo ratings yet
- GBV Register Final june20_2021_A3Document3 pagesGBV Register Final june20_2021_A3abdullee354No ratings yet
- Patient 2 Imst AmboDocument4 pagesPatient 2 Imst Amboapi-595102974No ratings yet
- Immediate/Case-based Surveillance Reporting Form IDSR 001ADocument58 pagesImmediate/Case-based Surveillance Reporting Form IDSR 001ASalihu MustaphaNo ratings yet
- PHEM ReportDocument2 pagesPHEM ReportmekuriaNo ratings yet
- Medical Examination: Subang Polyclinic SDN BHDDocument5 pagesMedical Examination: Subang Polyclinic SDN BHDSubang polylinicNo ratings yet
- Certificate of HealthDocument2 pagesCertificate of HealthmohamedydNo ratings yet
- Case Investigation Form - Measles-RubellaDocument2 pagesCase Investigation Form - Measles-Rubellaclaverialc10No ratings yet
- Influenza FormDocument2 pagesInfluenza FormDipendra PoudelNo ratings yet
- LacernaDocument1 pageLacernaKaren AdamraNo ratings yet
- OSCE-Checklist-Measuring-Basic-Observations-Vital-SignsDocument2 pagesOSCE-Checklist-Measuring-Basic-Observations-Vital-SignsZamir KhanNo ratings yet
- 2019 Certificate of Health Letter SizeDocument1 page2019 Certificate of Health Letter SizeAnonymous YG4TA3No ratings yet
- 01.17bmQT10 Health Examination ReportDocument6 pages01.17bmQT10 Health Examination ReportKita 09No ratings yet
- PFIZER 5 17 All in 1 FormDocument3 pagesPFIZER 5 17 All in 1 Formrenz jNo ratings yet
- Dohs, Edcd Disease Recording/Reporting Form Hospital Name Email Current AddressDocument4 pagesDohs, Edcd Disease Recording/Reporting Form Hospital Name Email Current AddressPrasanna LamaNo ratings yet
- Typhoid Fever Surveillance ReportDocument2 pagesTyphoid Fever Surveillance ReportMarketing HydNo ratings yet
- Sample Form - New Pre-Employment - MEDEX 001Document3 pagesSample Form - New Pre-Employment - MEDEX 001Helmi C MahadyNo ratings yet
- Nigeria ART Program Evaluation Data Extraction TooDocument9 pagesNigeria ART Program Evaluation Data Extraction TooALEMAYEHU SHIFERAWNo ratings yet
- (FORM) Medical Report AllDocument2 pages(FORM) Medical Report AllIndah AcphNo ratings yet
- Standard Medical Report TemplateDocument3 pagesStandard Medical Report TemplateAlvin WongNo ratings yet
- Afp 2013Document2 pagesAfp 2013rhu silagoNo ratings yet
- Kolej Teknologi Darulnaim: Darulnaim College of TechnologyDocument5 pagesKolej Teknologi Darulnaim: Darulnaim College of TechnologyDaryanto SutejiNo ratings yet
- Out-Patient Department (OPD) Register: Health Information System 3.0 MorbidityDocument5 pagesOut-Patient Department (OPD) Register: Health Information System 3.0 Morbidityhelawi'sNo ratings yet
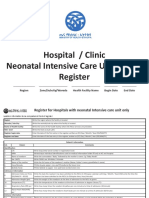
- NICU Register - A3 29008Document5 pagesNICU Register - A3 29008MesfinNo ratings yet
- Declaration of Good Health Form - With Covid QDocument2 pagesDeclaration of Good Health Form - With Covid QRajnish YadavNo ratings yet
- Week 05 - CLINICAL - STUDIES - DIAGNOSISDocument12 pagesWeek 05 - CLINICAL - STUDIES - DIAGNOSISEduard-Gabor HanțigNo ratings yet
- ISARIC COVID-19 CRF V1.3 24feb2020Document12 pagesISARIC COVID-19 CRF V1.3 24feb2020ARINTA DWI KOMALANo ratings yet
- MARCH NEWBORN.CENSUS 2023.csvDocument2 pagesMARCH NEWBORN.CENSUS 2023.csvPunsalan ChecaNo ratings yet
- NICU Register - A3Document5 pagesNICU Register - A3dabashgetNo ratings yet
- Botulism Toolkit: Emergency Recognition, Response and Anti Terrorism Training Associates (ERRATA, LLC.)Document18 pagesBotulism Toolkit: Emergency Recognition, Response and Anti Terrorism Training Associates (ERRATA, LLC.)Joko YantoNo ratings yet
- PEDIA PGI Endorsement Made by August Sept 2022 InternsDocument20 pagesPEDIA PGI Endorsement Made by August Sept 2022 InternsTrisNo ratings yet
- HM Medical Checkups at Project Sites Medical CampsDocument2 pagesHM Medical Checkups at Project Sites Medical Campsraj kumariNo ratings yet
- Anthrax CifDocument2 pagesAnthrax CifMary Anne Grace GarridoNo ratings yet
- Nursing Antenatal Activity TemplateDocument12 pagesNursing Antenatal Activity TemplateSteven ConejosNo ratings yet
- The Evaluation of Hematologic Screening and Perioperative Management in Patients With Noonan Syndrome: A Retrospective Chart ReviewDocument11 pagesThe Evaluation of Hematologic Screening and Perioperative Management in Patients With Noonan Syndrome: A Retrospective Chart ReviewMariaNo ratings yet
- Or 32 6 2836 PDFDocument9 pagesOr 32 6 2836 PDFJose SirittNo ratings yet
- Case Study Paper Template 11-12-23Document9 pagesCase Study Paper Template 11-12-23Syed Shams Haider MashhadiNo ratings yet
- Admission and DischargeDocument4 pagesAdmission and DischargeTribhuwan KushwahaNo ratings yet
- Final 2021 Protocol ALL Compressed 1Document209 pagesFinal 2021 Protocol ALL Compressed 1nathaniel perryNo ratings yet
- Preclinical Behavioral Science and Social Sciences Review 2023: For USMLE Step 1 and COMLEX-USA Level 1From EverandPreclinical Behavioral Science and Social Sciences Review 2023: For USMLE Step 1 and COMLEX-USA Level 1No ratings yet
- Complex Regional Pain Syndrome: A Clinical GuideFrom EverandComplex Regional Pain Syndrome: A Clinical GuideErin F. LawsonNo ratings yet
- PEST AnalysisDocument3 pagesPEST Analysisgekk0No ratings yet
- Daikin AC University Training Course Guide PDFDocument37 pagesDaikin AC University Training Course Guide PDFLeonard FransiscoNo ratings yet
- A 481 - 94 R00 QTQ4MQDocument3 pagesA 481 - 94 R00 QTQ4MQdelta lab sangliNo ratings yet
- BOSCH 01 Family OriginsDocument7 pagesBOSCH 01 Family OriginsAntonela ElenaNo ratings yet
- Lecture 2-Environmental Health HazardsDocument13 pagesLecture 2-Environmental Health HazardsAzizulHuqueNo ratings yet
- Application Form NNT EFDocument5 pagesApplication Form NNT EFRizky Aulya AkbarNo ratings yet
- Ae 191 Lesson 1Document14 pagesAe 191 Lesson 1Erna DavidNo ratings yet
- The Iconic Influence of Queen Elizabeth IIDocument2 pagesThe Iconic Influence of Queen Elizabeth IIpatriciasusckind_574No ratings yet
- Manitou Telehandler MLT 840 MLT 1040 Ps JD St4 s1 Genuine Parts Catalogue 647541en 09 2015Document22 pagesManitou Telehandler MLT 840 MLT 1040 Ps JD St4 s1 Genuine Parts Catalogue 647541en 09 2015mscassandravasquez120985pgc100% (106)
- Table 60001 Concrete DurabilityDocument1 pageTable 60001 Concrete DurabilityZaid JamilNo ratings yet
- Title: Investigation of Agriculture Related Problems of Rural Women in District LayyahDocument10 pagesTitle: Investigation of Agriculture Related Problems of Rural Women in District LayyahMuhammad Asim Hafeez ThindNo ratings yet
- CORDILLERADocument27 pagesCORDILLERAmaria kyla andradeNo ratings yet
- Laboratory or Rabbit or Pet Animal Productions PDFDocument19 pagesLaboratory or Rabbit or Pet Animal Productions PDFPublic InterestNo ratings yet
- Infectious Laryngotracheitis in Poultry: Razol RazalanDocument27 pagesInfectious Laryngotracheitis in Poultry: Razol RazalanLemuel Lagasca Razalan IVNo ratings yet
- Inquiry 2 Evidence 3Document5 pagesInquiry 2 Evidence 3api-311720502No ratings yet
- Architect-Entrepreneurs in Post-Independence Pune (India)Document17 pagesArchitect-Entrepreneurs in Post-Independence Pune (India)smelsensNo ratings yet
- Shaheed Suhrawardy Medical College HospitalDocument3 pagesShaheed Suhrawardy Medical College HospitalDr. Mohammad Nazrul IslamNo ratings yet
- Homework Font DownloadDocument5 pagesHomework Font Downloader9rz5b2100% (1)
- Math 7-Q4-Module-3Document16 pagesMath 7-Q4-Module-3Peterson Dela Cruz Enriquez33% (3)
- Knights of The Dinner Table 254Document70 pagesKnights of The Dinner Table 254Royce A R Porter100% (2)
- Annual Dealtracker 2021Document94 pagesAnnual Dealtracker 2021Vikrant Vikram SinghNo ratings yet
- 1st English Maths PDFDocument216 pages1st English Maths PDFmadhumster1240No ratings yet
- Invinsense OMDRDocument7 pagesInvinsense OMDRinfoperceptNo ratings yet
- Effect of Gibberellins On Plant GrowthDocument9 pagesEffect of Gibberellins On Plant Growthjasmeet dhillonNo ratings yet
- Athena: Microsoft ® Encarta ® Encyclopedia 2002. © 1993-2001 Microsoft Corporation. All RightsDocument1 pageAthena: Microsoft ® Encarta ® Encyclopedia 2002. © 1993-2001 Microsoft Corporation. All RightsAnonymous ck0aGAqZlNo ratings yet
- Trimble R8s GNSS Receiver: User GuideDocument71 pagesTrimble R8s GNSS Receiver: User GuideSilvio Vuolo NetoNo ratings yet























































































Download as pdf or txt
You might also like
- List of Pharmaceutical Companies in Ahmedabad WithDocument22 pagesList of Pharmaceutical Companies in Ahmedabad Withsandipsc88% (8)
- Pidsr CifDocument17 pagesPidsr CifAbraham Asto100% (4)
- Soap NoteDocument2 pagesSoap Notetopopirate100% (4)
- Chapter 1 - Introduction To The Food and Beverage IndustryDocument64 pagesChapter 1 - Introduction To The Food and Beverage IndustryPn Firdaus92% (12)
- Laboratory Request FormDocument1 pageLaboratory Request FormEric Nagum100% (2)
- Best 25 Question and Answer For Boiler First and Second Class Operator Viva Examination 2017 - ASKPOWERPLANTDocument32 pagesBest 25 Question and Answer For Boiler First and Second Class Operator Viva Examination 2017 - ASKPOWERPLANTRaju Maity100% (5)
- CASESHEETPHARMDDocument6 pagesCASESHEETPHARMDSai SharathNo ratings yet
- Examination and Result Management System - TutorialsDuniya PDFDocument56 pagesExamination and Result Management System - TutorialsDuniya PDFAishwaryaNo ratings yet
- Instructions For Leishmanises Register: Day / Month / Year (DD/MM/YY) (EC)Document2 pagesInstructions For Leishmanises Register: Day / Month / Year (DD/MM/YY) (EC)Dagnachew MulugetaNo ratings yet
- MOH 405 ANC Register 1Document4 pagesMOH 405 ANC Register 1S DonoughNo ratings yet
- DR TB REGISTER A3 SizeDocument5 pagesDR TB REGISTER A3 Sizeabdullee354No ratings yet
- PNC - A3-1Document5 pagesPNC - A3-1dabashgetNo ratings yet
- Health Center/Clinic/Hospital: Out Patient Department (OPD) RegisterDocument4 pagesHealth Center/Clinic/Hospital: Out Patient Department (OPD) RegisterGetu Tadele100% (2)
- DR Follow up registration_A3Document5 pagesDR Follow up registration_A3abdullee354No ratings yet
- 3.anc A3Document3 pages3.anc A3dabashgetNo ratings yet
- HSTP II HMIS Hospital Heath Centre and Health PostDocument367 pagesHSTP II HMIS Hospital Heath Centre and Health PostDagmawitNo ratings yet
- Unit TB Register A3Document6 pagesUnit TB Register A3abdullee354No ratings yet
- Health Centre /Clinic/Hospital MAM Treatment For 6-59 MonthsDocument3 pagesHealth Centre /Clinic/Hospital MAM Treatment For 6-59 MonthsAmenti FiromsaNo ratings yet
- CERTIFICATE OF HEALTH (To Be Filled Out by A Physician) - Page 1Document2 pagesCERTIFICATE OF HEALTH (To Be Filled Out by A Physician) - Page 1gnzbdbNo ratings yet
- Health Centre /Clinic/Hospital Family Planning RegisterDocument4 pagesHealth Centre /Clinic/Hospital Family Planning RegisterAnuka YituNo ratings yet
- Form 6a. Drug Susceptible TB RegisterDocument4 pagesForm 6a. Drug Susceptible TB RegisterAllen ChesterNo ratings yet
- Health DeclarationDocument5 pagesHealth Declarationust dol100% (1)
- Health Declaration and Medical Examination Form: Scholarship DivisionDocument5 pagesHealth Declaration and Medical Examination Form: Scholarship Divisionnazrin sarajuddinNo ratings yet
- Clinical Case Study Guideline and TemplateDocument19 pagesClinical Case Study Guideline and TemplateMikhaela Andree MarianoNo ratings yet
- GBV Register Final june20_2021_A3Document3 pagesGBV Register Final june20_2021_A3abdullee354No ratings yet
- Patient 2 Imst AmboDocument4 pagesPatient 2 Imst Amboapi-595102974No ratings yet
- Immediate/Case-based Surveillance Reporting Form IDSR 001ADocument58 pagesImmediate/Case-based Surveillance Reporting Form IDSR 001ASalihu MustaphaNo ratings yet
- PHEM ReportDocument2 pagesPHEM ReportmekuriaNo ratings yet
- Medical Examination: Subang Polyclinic SDN BHDDocument5 pagesMedical Examination: Subang Polyclinic SDN BHDSubang polylinicNo ratings yet
- Certificate of HealthDocument2 pagesCertificate of HealthmohamedydNo ratings yet
- Case Investigation Form - Measles-RubellaDocument2 pagesCase Investigation Form - Measles-Rubellaclaverialc10No ratings yet
- Influenza FormDocument2 pagesInfluenza FormDipendra PoudelNo ratings yet
- LacernaDocument1 pageLacernaKaren AdamraNo ratings yet
- OSCE-Checklist-Measuring-Basic-Observations-Vital-SignsDocument2 pagesOSCE-Checklist-Measuring-Basic-Observations-Vital-SignsZamir KhanNo ratings yet
- 2019 Certificate of Health Letter SizeDocument1 page2019 Certificate of Health Letter SizeAnonymous YG4TA3No ratings yet
- 01.17bmQT10 Health Examination ReportDocument6 pages01.17bmQT10 Health Examination ReportKita 09No ratings yet
- PFIZER 5 17 All in 1 FormDocument3 pagesPFIZER 5 17 All in 1 Formrenz jNo ratings yet
- Dohs, Edcd Disease Recording/Reporting Form Hospital Name Email Current AddressDocument4 pagesDohs, Edcd Disease Recording/Reporting Form Hospital Name Email Current AddressPrasanna LamaNo ratings yet
- Typhoid Fever Surveillance ReportDocument2 pagesTyphoid Fever Surveillance ReportMarketing HydNo ratings yet
- Sample Form - New Pre-Employment - MEDEX 001Document3 pagesSample Form - New Pre-Employment - MEDEX 001Helmi C MahadyNo ratings yet
- Nigeria ART Program Evaluation Data Extraction TooDocument9 pagesNigeria ART Program Evaluation Data Extraction TooALEMAYEHU SHIFERAWNo ratings yet
- (FORM) Medical Report AllDocument2 pages(FORM) Medical Report AllIndah AcphNo ratings yet
- Standard Medical Report TemplateDocument3 pagesStandard Medical Report TemplateAlvin WongNo ratings yet
- Afp 2013Document2 pagesAfp 2013rhu silagoNo ratings yet
- Kolej Teknologi Darulnaim: Darulnaim College of TechnologyDocument5 pagesKolej Teknologi Darulnaim: Darulnaim College of TechnologyDaryanto SutejiNo ratings yet
- Out-Patient Department (OPD) Register: Health Information System 3.0 MorbidityDocument5 pagesOut-Patient Department (OPD) Register: Health Information System 3.0 Morbidityhelawi'sNo ratings yet
- NICU Register - A3 29008Document5 pagesNICU Register - A3 29008MesfinNo ratings yet
- Declaration of Good Health Form - With Covid QDocument2 pagesDeclaration of Good Health Form - With Covid QRajnish YadavNo ratings yet
- Week 05 - CLINICAL - STUDIES - DIAGNOSISDocument12 pagesWeek 05 - CLINICAL - STUDIES - DIAGNOSISEduard-Gabor HanțigNo ratings yet
- ISARIC COVID-19 CRF V1.3 24feb2020Document12 pagesISARIC COVID-19 CRF V1.3 24feb2020ARINTA DWI KOMALANo ratings yet
- MARCH NEWBORN.CENSUS 2023.csvDocument2 pagesMARCH NEWBORN.CENSUS 2023.csvPunsalan ChecaNo ratings yet
- NICU Register - A3Document5 pagesNICU Register - A3dabashgetNo ratings yet
- Botulism Toolkit: Emergency Recognition, Response and Anti Terrorism Training Associates (ERRATA, LLC.)Document18 pagesBotulism Toolkit: Emergency Recognition, Response and Anti Terrorism Training Associates (ERRATA, LLC.)Joko YantoNo ratings yet
- PEDIA PGI Endorsement Made by August Sept 2022 InternsDocument20 pagesPEDIA PGI Endorsement Made by August Sept 2022 InternsTrisNo ratings yet
- HM Medical Checkups at Project Sites Medical CampsDocument2 pagesHM Medical Checkups at Project Sites Medical Campsraj kumariNo ratings yet
- Anthrax CifDocument2 pagesAnthrax CifMary Anne Grace GarridoNo ratings yet
- Nursing Antenatal Activity TemplateDocument12 pagesNursing Antenatal Activity TemplateSteven ConejosNo ratings yet
- The Evaluation of Hematologic Screening and Perioperative Management in Patients With Noonan Syndrome: A Retrospective Chart ReviewDocument11 pagesThe Evaluation of Hematologic Screening and Perioperative Management in Patients With Noonan Syndrome: A Retrospective Chart ReviewMariaNo ratings yet
- Or 32 6 2836 PDFDocument9 pagesOr 32 6 2836 PDFJose SirittNo ratings yet
- Case Study Paper Template 11-12-23Document9 pagesCase Study Paper Template 11-12-23Syed Shams Haider MashhadiNo ratings yet
- Admission and DischargeDocument4 pagesAdmission and DischargeTribhuwan KushwahaNo ratings yet
- Final 2021 Protocol ALL Compressed 1Document209 pagesFinal 2021 Protocol ALL Compressed 1nathaniel perryNo ratings yet
- Preclinical Behavioral Science and Social Sciences Review 2023: For USMLE Step 1 and COMLEX-USA Level 1From EverandPreclinical Behavioral Science and Social Sciences Review 2023: For USMLE Step 1 and COMLEX-USA Level 1No ratings yet
- Complex Regional Pain Syndrome: A Clinical GuideFrom EverandComplex Regional Pain Syndrome: A Clinical GuideErin F. LawsonNo ratings yet
- PEST AnalysisDocument3 pagesPEST Analysisgekk0No ratings yet
- Daikin AC University Training Course Guide PDFDocument37 pagesDaikin AC University Training Course Guide PDFLeonard FransiscoNo ratings yet
- A 481 - 94 R00 QTQ4MQDocument3 pagesA 481 - 94 R00 QTQ4MQdelta lab sangliNo ratings yet
- BOSCH 01 Family OriginsDocument7 pagesBOSCH 01 Family OriginsAntonela ElenaNo ratings yet
- Lecture 2-Environmental Health HazardsDocument13 pagesLecture 2-Environmental Health HazardsAzizulHuqueNo ratings yet
- Application Form NNT EFDocument5 pagesApplication Form NNT EFRizky Aulya AkbarNo ratings yet
- Ae 191 Lesson 1Document14 pagesAe 191 Lesson 1Erna DavidNo ratings yet
- The Iconic Influence of Queen Elizabeth IIDocument2 pagesThe Iconic Influence of Queen Elizabeth IIpatriciasusckind_574No ratings yet
- Manitou Telehandler MLT 840 MLT 1040 Ps JD St4 s1 Genuine Parts Catalogue 647541en 09 2015Document22 pagesManitou Telehandler MLT 840 MLT 1040 Ps JD St4 s1 Genuine Parts Catalogue 647541en 09 2015mscassandravasquez120985pgc100% (106)
- Table 60001 Concrete DurabilityDocument1 pageTable 60001 Concrete DurabilityZaid JamilNo ratings yet
- Title: Investigation of Agriculture Related Problems of Rural Women in District LayyahDocument10 pagesTitle: Investigation of Agriculture Related Problems of Rural Women in District LayyahMuhammad Asim Hafeez ThindNo ratings yet
- CORDILLERADocument27 pagesCORDILLERAmaria kyla andradeNo ratings yet
- Laboratory or Rabbit or Pet Animal Productions PDFDocument19 pagesLaboratory or Rabbit or Pet Animal Productions PDFPublic InterestNo ratings yet
- Infectious Laryngotracheitis in Poultry: Razol RazalanDocument27 pagesInfectious Laryngotracheitis in Poultry: Razol RazalanLemuel Lagasca Razalan IVNo ratings yet
- Inquiry 2 Evidence 3Document5 pagesInquiry 2 Evidence 3api-311720502No ratings yet
- Architect-Entrepreneurs in Post-Independence Pune (India)Document17 pagesArchitect-Entrepreneurs in Post-Independence Pune (India)smelsensNo ratings yet
- Shaheed Suhrawardy Medical College HospitalDocument3 pagesShaheed Suhrawardy Medical College HospitalDr. Mohammad Nazrul IslamNo ratings yet
- Homework Font DownloadDocument5 pagesHomework Font Downloader9rz5b2100% (1)
- Math 7-Q4-Module-3Document16 pagesMath 7-Q4-Module-3Peterson Dela Cruz Enriquez33% (3)
- Knights of The Dinner Table 254Document70 pagesKnights of The Dinner Table 254Royce A R Porter100% (2)
- Annual Dealtracker 2021Document94 pagesAnnual Dealtracker 2021Vikrant Vikram SinghNo ratings yet
- 1st English Maths PDFDocument216 pages1st English Maths PDFmadhumster1240No ratings yet
- Invinsense OMDRDocument7 pagesInvinsense OMDRinfoperceptNo ratings yet
- Effect of Gibberellins On Plant GrowthDocument9 pagesEffect of Gibberellins On Plant Growthjasmeet dhillonNo ratings yet
- Athena: Microsoft ® Encarta ® Encyclopedia 2002. © 1993-2001 Microsoft Corporation. All RightsDocument1 pageAthena: Microsoft ® Encarta ® Encyclopedia 2002. © 1993-2001 Microsoft Corporation. All RightsAnonymous ck0aGAqZlNo ratings yet
- Trimble R8s GNSS Receiver: User GuideDocument71 pagesTrimble R8s GNSS Receiver: User GuideSilvio Vuolo NetoNo ratings yet