Download as pdf or txt
You might also like
- Controversies in Clear Aligner Therapy Contemporary PerspectivesDocument202 pagesControversies in Clear Aligner Therapy Contemporary PerspectivesDiego Lopez100% (7)
- This Study Resource Was: Running Head: Amira Quintona 1Document5 pagesThis Study Resource Was: Running Head: Amira Quintona 1Holly DeckelmanNo ratings yet
- Health Center/Clinic/Hospital: Out Patient Department (OPD) RegisterDocument4 pagesHealth Center/Clinic/Hospital: Out Patient Department (OPD) RegisterGetu Tadele100% (2)
- DR TB REGISTER A3 SizeDocument5 pagesDR TB REGISTER A3 Sizeabdullee354No ratings yet
- Health Centre /Clinic/Hospital Family Planning RegisterDocument4 pagesHealth Centre /Clinic/Hospital Family Planning RegisterAnuka YituNo ratings yet
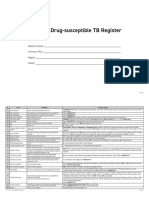
- Form 6a. Drug Susceptible TB RegisterDocument4 pagesForm 6a. Drug Susceptible TB RegisterAllen ChesterNo ratings yet
- DR Follow up registration_A3Document5 pagesDR Follow up registration_A3abdullee354No ratings yet
- Member Dental Claim Form: Mark All Applicable Boxes)Document4 pagesMember Dental Claim Form: Mark All Applicable Boxes)TreyNo ratings yet
- Out-Patient Department (OPD) Register: Health Information System 3.0 MorbidityDocument5 pagesOut-Patient Department (OPD) Register: Health Information System 3.0 Morbidityhelawi'sNo ratings yet
- Emt Physical FormDocument1 pageEmt Physical FormLeeann LopezNo ratings yet
- Leishman Register_A3Document3 pagesLeishman Register_A3abdullee354No ratings yet
- PNC - A3-1Document5 pagesPNC - A3-1dabashgetNo ratings yet
- Cytogenetics_Hematology_OncologyDocument3 pagesCytogenetics_Hematology_OncologysiradanbilgilerNo ratings yet
- Clinical Treatment PDFDocument1 pageClinical Treatment PDFDanielle YoderNo ratings yet
- Afp 2013Document2 pagesAfp 2013rhu silagoNo ratings yet
- Medical Survey: Covid-19 Tests: RT-PCR - Rapid Antigen - SerologicDocument1 pageMedical Survey: Covid-19 Tests: RT-PCR - Rapid Antigen - SerologicSales DptNo ratings yet
- Printable Version - Approval Reference No - 60247630Document2 pagesPrintable Version - Approval Reference No - 60247630sohaibkhaled5858No ratings yet
- Adobe Scan Mar 12, 2021Document9 pagesAdobe Scan Mar 12, 2021Nemish ShahNo ratings yet
- Claim Form B Medical Attendant CertificateDocument1 pageClaim Form B Medical Attendant Certificatesuja01974No ratings yet
- The Benefits Center P.O. Box 100158 Columbia, SC 29202-3158 Toll-Free: 1-800-858-6843 Fax: 1-800-447-2498 Call Toll-Free Monday Through Friday, 8 A.M. To 8 P.M. (Eastern Time)Document2 pagesThe Benefits Center P.O. Box 100158 Columbia, SC 29202-3158 Toll-Free: 1-800-858-6843 Fax: 1-800-447-2498 Call Toll-Free Monday Through Friday, 8 A.M. To 8 P.M. (Eastern Time)paul geyerNo ratings yet
- Nigeria ART Program Evaluation Data Extraction TooDocument9 pagesNigeria ART Program Evaluation Data Extraction TooALEMAYEHU SHIFERAWNo ratings yet
- Acn BlankDocument1 pageAcn BlankDiego ProanoNo ratings yet
- C5Document2 pagesC5ijustwanawriteNo ratings yet
- Discharge Planning TBDocument2 pagesDischarge Planning TBNurida LatipahNo ratings yet
- 5.sample Case Report CRF Template FormDocument32 pages5.sample Case Report CRF Template FormmilenabogojevskaNo ratings yet
- Patient: Print Form Reset FormDocument2 pagesPatient: Print Form Reset FormAlyssa DavidNo ratings yet
- 2019 Coronavirus Disease (Covid-19) : 1. Patient ProfileDocument1 page2019 Coronavirus Disease (Covid-19) : 1. Patient ProfileMarythel CamachoNo ratings yet
- TRF A1059360 ORfd615084db974a95afe23RVL 2022-01-20T13 41 50.822Document2 pagesTRF A1059360 ORfd615084db974a95afe23RVL 2022-01-20T13 41 50.822traveltreatsteluguNo ratings yet
- Clinical Treatment Form: I DIAGNOSES (Must Be To The Highest Level of Specificity)Document1 pageClinical Treatment Form: I DIAGNOSES (Must Be To The Highest Level of Specificity)Danielle YoderNo ratings yet
- Health Centre /Clinic/Hospital MAM Treatment For 6-59 MonthsDocument3 pagesHealth Centre /Clinic/Hospital MAM Treatment For 6-59 MonthsAmenti FiromsaNo ratings yet
- Surgical Site Infection (SSI) : Event DetailsDocument4 pagesSurgical Site Infection (SSI) : Event DetailsLhaineVennetNo ratings yet
- Zika IcifDocument2 pagesZika IcifMarav SymbNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormMizraim TupazNo ratings yet
- DRTB Treatment CardDocument11 pagesDRTB Treatment CardMaycel DumayaNo ratings yet
- GOS18 Referral Form 1Document2 pagesGOS18 Referral Form 1parvathyNo ratings yet
- AMITYDocument1 pageAMITYTRTNo ratings yet
- Standard Insurance Company: Attending Dentist's Statement Treatment Plan and Insurance Claim ReportDocument2 pagesStandard Insurance Company: Attending Dentist's Statement Treatment Plan and Insurance Claim ReportAfzal ImamNo ratings yet
- Unit TB Register A3Document6 pagesUnit TB Register A3abdullee354No ratings yet
- CIF RotavirusDocument1 pageCIF RotavirusIvy marie BonNo ratings yet
- KipiDocument1 pageKipiHeRha DAniarNo ratings yet
- UB-04 Claim Form InstructionsDocument10 pagesUB-04 Claim Form InstructionsJonna CaballeroNo ratings yet
- Medical OpinionDocument1 pageMedical OpinionefmezahnNo ratings yet
- PFIZER 5 17 All in 1 FormDocument3 pagesPFIZER 5 17 All in 1 Formrenz jNo ratings yet
- N.A.B.H. Parameter Sheet: Network Hospital Grading ProformaDocument7 pagesN.A.B.H. Parameter Sheet: Network Hospital Grading ProformaDhananjay SainiNo ratings yet
- Adobe Scan 18-Mar-2023Document2 pagesAdobe Scan 18-Mar-2023sachin.kr21No ratings yet
- 'NEXtCARE Egypt - Reimbursement FormDocument1 page'NEXtCARE Egypt - Reimbursement FormMohyee Eldin RagebNo ratings yet
- Finished ChartDocument14 pagesFinished Chartapi-340832560No ratings yet
- Manila, Philippines: I. Patient InformationDocument1 pageManila, Philippines: I. Patient InformationJoa QuinNo ratings yet
- Manila, Philippines: I. Patient InformationDocument1 pageManila, Philippines: I. Patient InformationJoa QuinNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument2 pagesCoronavirus Disease (COVID-19) : Case Investigation FormShiela E. EladNo ratings yet
- Form 1: Cashless Request Form Iffco Tokio General Insurance Company LimitedDocument2 pagesForm 1: Cashless Request Form Iffco Tokio General Insurance Company LimitedRaju.PalNo ratings yet
- Health Declaration FormDocument12 pagesHealth Declaration FormAmelia Delos ReyesNo ratings yet
- Las Piñas CIFDocument1 pageLas Piñas CIFchrisNo ratings yet
- Hospital Seal (Must Contain Hospital ID) : Patient / Insured Name & SignatureDocument6 pagesHospital Seal (Must Contain Hospital ID) : Patient / Insured Name & SignaturePrince GargNo ratings yet
- Standard Medical Report TemplateDocument3 pagesStandard Medical Report TemplateAlvin WongNo ratings yet
- Pre Authorization FormDocument1 pagePre Authorization FormMurugan RamalingamNo ratings yet
- HSTP II HMIS Hospital Heath Centre and Health PostDocument367 pagesHSTP II HMIS Hospital Heath Centre and Health PostDagmawitNo ratings yet
- Commercial Drivers Licence Medical ReportDocument2 pagesCommercial Drivers Licence Medical ReportChameera Madusanka YapaNo ratings yet
- Male Female TS/TG Male Female TS/TG Male Female TS/TG Male Female TS/TG Male Female TS/TGDocument4 pagesMale Female TS/TG Male Female TS/TG Male Female TS/TG Male Female TS/TG Male Female TS/TGINSANE IDEASNo ratings yet
- Ej CRF Case Report FormDocument38 pagesEj CRF Case Report FormAgustina Díaz CazauxNo ratings yet
- Medical Coding ICD-10-CM: a QuickStudy Laminated Reference GuideFrom EverandMedical Coding ICD-10-CM: a QuickStudy Laminated Reference GuideNo ratings yet
- Item Prek OotDocument9 pagesItem Prek OotAmaliya 23No ratings yet
- AKL SYAF Price List E-Katalog 20092022Document6 pagesAKL SYAF Price List E-Katalog 20092022Y HWNo ratings yet
- Corrected Proposal Corrected.Document10 pagesCorrected Proposal Corrected.Preeti ChouhanNo ratings yet
- Spontaneous Swallowing Frequency in Post-Stroke Patients With and Without Oropharyngeal Dysphagia - An Observational StudyDocument11 pagesSpontaneous Swallowing Frequency in Post-Stroke Patients With and Without Oropharyngeal Dysphagia - An Observational StudyAlvina RusliNo ratings yet
- Maklumat Vaksinasi: Vaccination DetailsDocument2 pagesMaklumat Vaksinasi: Vaccination DetailsHariz ZahinNo ratings yet
- Appendix E - Sponsorship Certificate INI CET PG July 2021 SessionDocument1 pageAppendix E - Sponsorship Certificate INI CET PG July 2021 Sessionudham sudanNo ratings yet
- AyushDocument26 pagesAyushdurgesh choudharyNo ratings yet
- Jhpeigo Advert - Case Manager.Document2 pagesJhpeigo Advert - Case Manager.John EkerekeNo ratings yet
- Dabl Educational TrustMonitors For Self-Measurement of Blood Pressure (SBPM)Document1 pageDabl Educational TrustMonitors For Self-Measurement of Blood Pressure (SBPM)iranbengoaNo ratings yet
- English9 Q4 W4 Mod4Document16 pagesEnglish9 Q4 W4 Mod4Azlan SorrondaNo ratings yet
- Surat Penawaran Ambulance Complete Plus Isi RSKB Siaga1Document5 pagesSurat Penawaran Ambulance Complete Plus Isi RSKB Siaga1Halil GuramiNo ratings yet
- 49-Article Text-292-1-10-20201231Document8 pages49-Article Text-292-1-10-20201231meirin windyasariNo ratings yet
- 2nd Re Scho List Ug2023Document46 pages2nd Re Scho List Ug2023Rajnish kumar ThakurNo ratings yet
- Banned Drugs PDFDocument16 pagesBanned Drugs PDFJose mathewNo ratings yet
- HR Sheet 2023Document45 pagesHR Sheet 2023Cho LayNo ratings yet
- BooksDocument96 pagesBooksVINAY KUMAR DHAWANNo ratings yet
- Department of Health & Human ServicesDocument11 pagesDepartment of Health & Human Servicesgildardo ruizNo ratings yet
- Bunnell Life Pulse 204 Quick Reference GuideDocument12 pagesBunnell Life Pulse 204 Quick Reference GuideRafael RamirezNo ratings yet
- Current Concepts in The Management of The Difficult Airway HagbergDocument32 pagesCurrent Concepts in The Management of The Difficult Airway HagbergAlejandro PiedrahitaNo ratings yet
- Finshe P. Ybanez 1BSN-ADocument3 pagesFinshe P. Ybanez 1BSN-Ajerica abesamis100% (2)
- Percutaneous Interventional Cardiovascular Medicine - The PCR-EAPCI TextbookDocument18 pagesPercutaneous Interventional Cardiovascular Medicine - The PCR-EAPCI TextbookRanda TabbahNo ratings yet
- Notice Under Section 80, Code 0F Civil Procedure Against Public OfficerDocument4 pagesNotice Under Section 80, Code 0F Civil Procedure Against Public OfficerAditi TNo ratings yet
- pdfR2Document15 pagespdfR2నా పూకులో సనాతన ధర్మంNo ratings yet
- Suquamish News - Feb 2022-CompressedDocument16 pagesSuquamish News - Feb 2022-Compressedapi-542412193No ratings yet
- +Jurnal+Kesehatan 2Document13 pages+Jurnal+Kesehatan 2Gaidha NurfadhilahNo ratings yet
- Family: I Don'T Believe in Love AnymoreDocument52 pagesFamily: I Don'T Believe in Love AnymorevicNo ratings yet
- Closure of Midline Diastema by Direct Composite Resin Build-Up Using Putty Index - A CasereportDocument5 pagesClosure of Midline Diastema by Direct Composite Resin Build-Up Using Putty Index - A CasereportIJAR JOURNALNo ratings yet
- CertificateDocument1 pageCertificateZainab KhanNo ratings yet